Download as pdf or txt
You might also like
- (MRR) Forgiveness-WorkbookDocument67 pages(MRR) Forgiveness-WorkbookKausar Imran100% (6)
- Hirschsprung 'S Disease: Incidence and Classi FicationDocument6 pagesHirschsprung 'S Disease: Incidence and Classi FicationGhina Mauizha WulandariNo ratings yet
- Hirschsprung's Disease: Surgery (Oxford) November 2016Document6 pagesHirschsprung's Disease: Surgery (Oxford) November 2016sytaNo ratings yet
- Intestinal Pathology III Hirschsprung'S Disease: DR Nzau MuangeDocument21 pagesIntestinal Pathology III Hirschsprung'S Disease: DR Nzau MuangeNzau MuangeNo ratings yet
- Pathology of Intestinal Motor DisordersDocument31 pagesPathology of Intestinal Motor DisorderslegrangedanitaNo ratings yet
- Hirschsprung DiseaseDocument18 pagesHirschsprung DiseaseResianaPutriNo ratings yet
- Hirchsprung Correlated GeneticDocument12 pagesHirchsprung Correlated GeneticAlpascaFirdausNo ratings yet
- New Frontiers in The Treatment of Hirschsprung.17Document3 pagesNew Frontiers in The Treatment of Hirschsprung.17Hayati Rizki PutriNo ratings yet
- Hirsch SprungDocument20 pagesHirsch SprungrisaNo ratings yet
- HSCR DiseaseDocument17 pagesHSCR DiseaseKikyTriachristyNo ratings yet
- Hirschsprung Disease PDFDocument8 pagesHirschsprung Disease PDFAlchemistalazkaNo ratings yet
- Hirschsprung's DiseaseDocument3 pagesHirschsprung's DiseaserjalavazoNo ratings yet
- p1319 PDFDocument4 pagesp1319 PDFSyairodhiNo ratings yet
- Hirschsprung - Megacólon CongênitoDocument17 pagesHirschsprung - Megacólon CongênitoBarbara NevesNo ratings yet
- 2021 Article 268Document10 pages2021 Article 268lorena.rivera.1912No ratings yet
- Hirschsprung DiseaseDocument13 pagesHirschsprung Diseaseganesh reddyNo ratings yet
- Hirschsprung'S Disease: Peter MatteiDocument1 pageHirschsprung'S Disease: Peter MatteiJulia Wibawa HaryantoNo ratings yet
- Hirschsprung DiseaseDocument21 pagesHirschsprung Diseaseeatingchoice100% (1)
- 729 FullDocument11 pages729 FullAndikaNo ratings yet
- Background: Hirschsprung Disease. Contrast Enema Demonstrating Transition Zone in The Rectosigmoid RegionDocument9 pagesBackground: Hirschsprung Disease. Contrast Enema Demonstrating Transition Zone in The Rectosigmoid RegionWeny SyifaNo ratings yet
- Hirschsprung Disease - A SAGES Wiki ArticleDocument12 pagesHirschsprung Disease - A SAGES Wiki ArticleIndra GunawanNo ratings yet
- HirschsprungDocument11 pagesHirschsprungKarl JoseNo ratings yet
- Congenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasDocument6 pagesCongenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasSyakilla AuliaNo ratings yet
- January - Hirschsprung's Disease in Africa 21 CenturyDocument27 pagesJanuary - Hirschsprung's Disease in Africa 21 CenturyVita MadmoNo ratings yet
- Placino HIRSCHPRUNG DX PDFDocument15 pagesPlacino HIRSCHPRUNG DX PDFSiena PlacinoNo ratings yet
- HirschprungDocument6 pagesHirschprungVanessa CasingalNo ratings yet
- Hirschsprung's Disease: (Congenital Aganglionic Megacolon)Document16 pagesHirschsprung's Disease: (Congenital Aganglionic Megacolon)umiNo ratings yet
- Hirschsprung 1socaDocument34 pagesHirschsprung 1socaDianNo ratings yet
- Hirschsprung Disease: Historical NotesDocument17 pagesHirschsprung Disease: Historical Notesdesthalia cyatraningtyasNo ratings yet
- Hirsch SprungDocument84 pagesHirsch SprungobligatraftelNo ratings yet
- Antenatal Diagnosis ofDocument6 pagesAntenatal Diagnosis ofnskhldNo ratings yet
- Ultrasound Features of Spermatic Cord Hydrocele in ChildrenDocument3 pagesUltrasound Features of Spermatic Cord Hydrocele in ChildrenEnricoFermihutagalungNo ratings yet
- Hirschsprung DiseaseDocument4 pagesHirschsprung DiseaseMahmoud SalmanNo ratings yet
- Hirschsprung DiseaseDocument44 pagesHirschsprung DiseaseAhmad Abu KushNo ratings yet
- Cystic HygromaDocument4 pagesCystic HygromaafrisiammyNo ratings yet
- Hirschsprung DiseaseDocument24 pagesHirschsprung DiseaseRahayu AsmaraniNo ratings yet
- Hirschsprung's DiseaseDocument18 pagesHirschsprung's DiseaseanisyahNo ratings yet
- HIRSCHSPRUNG's DISEASE (Aganglionic Megacolon) Definition Presence of Large, Non-Functional DistalDocument3 pagesHIRSCHSPRUNG's DISEASE (Aganglionic Megacolon) Definition Presence of Large, Non-Functional Distalkhadzx100% (2)
- Hirsch Pung SDocument10 pagesHirsch Pung Sotto naftariNo ratings yet
- Hirsch SprungDocument6 pagesHirsch SprunghakimNo ratings yet
- Journal Reading: Hirschprung's Disease Devin Reynando 1210118602Document23 pagesJournal Reading: Hirschprung's Disease Devin Reynando 1210118602Devin RNo ratings yet
- Butlertjaden 2013Document15 pagesButlertjaden 2013Raluca MosoiaNo ratings yet
- Enfermedad de Hirschsprung: Diagnóstico Y Manejo en Niños Y AdultosDocument5 pagesEnfermedad de Hirschsprung: Diagnóstico Y Manejo en Niños Y AdultosAlexander Castillo CalderónNo ratings yet
- Hirschprung Disease: Department of Radiology Medical Faculty of Hasanuddin University, MakassarDocument15 pagesHirschprung Disease: Department of Radiology Medical Faculty of Hasanuddin University, Makassardewi sartikaNo ratings yet
- Journal of Pediatric Surgery Case Reports: Moaied A. Hassan, Hasan K. Gatea, Thura K. Ja'afar, Ahmed O. Fahad TDocument3 pagesJournal of Pediatric Surgery Case Reports: Moaied A. Hassan, Hasan K. Gatea, Thura K. Ja'afar, Ahmed O. Fahad TVero MeidyNo ratings yet
- Restoring Normal Anatomy in Female Patients With Atypical GenitaliaDocument5 pagesRestoring Normal Anatomy in Female Patients With Atypical GenitaliaCuidados Enfermagem DomicílioNo ratings yet
- Hirsch SprungDocument16 pagesHirsch SprungjessyNo ratings yet
- IJKD - News Letter1 20 26Document8 pagesIJKD - News Letter1 20 26Kapil SejpalNo ratings yet
- Case Report: Hirschsprung Disease: Aprilia Silambi, Tri Setyawati, Alfreth LangitanDocument5 pagesCase Report: Hirschsprung Disease: Aprilia Silambi, Tri Setyawati, Alfreth LangitanSabrina brinNo ratings yet
- Cirugi A Espan Ola: Clinical Xenotransplantation, A Closer Reality: Literature ReviewDocument11 pagesCirugi A Espan Ola: Clinical Xenotransplantation, A Closer Reality: Literature ReviewMaritsa PerHerNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- 1 s2.0 S2049080121010074 MainDocument4 pages1 s2.0 S2049080121010074 Maintithania insanilahiaNo ratings yet
- Intussusception TransDocument4 pagesIntussusception TransJames Maravillas100% (1)
- Caudal Duplication SyndromeDocument3 pagesCaudal Duplication Syndromekhumaira1982No ratings yet
- Green 2016Document6 pagesGreen 2016Donny Artya KesumaNo ratings yet
- HirscDocument33 pagesHirscBambang SchrickNo ratings yet
- Hirschsprung Disease: Waardenburg Syndrome Mowat-Wilson Syndrome Congenital Central Hypoventilation SyndromeDocument22 pagesHirschsprung Disease: Waardenburg Syndrome Mowat-Wilson Syndrome Congenital Central Hypoventilation SyndromeRizki Nandasari SulbahriNo ratings yet
- Hirschsprung Disease: Nadia Ismael Muse Safia Ahmed-Yassin SH: Ali Ilham Saed JirdeDocument24 pagesHirschsprung Disease: Nadia Ismael Muse Safia Ahmed-Yassin SH: Ali Ilham Saed Jirdesafia ahmedNo ratings yet
- Hirschsprung DiseaseDocument25 pagesHirschsprung DiseaseMuhammad Zaniar RamadhaniNo ratings yet
- Lesson Plan Hisschsprung DiseaseDocument10 pagesLesson Plan Hisschsprung DiseasePPG Selvi Jebakani IsaacNo ratings yet
- Solving the riddle of cancer: new genetic approaches to treatmentFrom EverandSolving the riddle of cancer: new genetic approaches to treatmentNo ratings yet
- Argus Field Service Kit User Guide PDFDocument4 pagesArgus Field Service Kit User Guide PDFBeneDict Ben DNo ratings yet
- Road Signage and MarkingsDocument8 pagesRoad Signage and MarkingsNimako MichaelNo ratings yet
- Periodic Waveform Generation in FPGADocument7 pagesPeriodic Waveform Generation in FPGAnm2007kNo ratings yet
- Conversion and CalculationDocument40 pagesConversion and CalculationJhonel MelgarNo ratings yet
- Our Ultimate Reality Newsletter 22 July 2012Document3 pagesOur Ultimate Reality Newsletter 22 July 2012khaveiNo ratings yet
- 2009 Notes - HTMDocument4 pages2009 Notes - HTMlightingfastno808100% (2)
- Conduction Convection Radiation PowerpointDocument27 pagesConduction Convection Radiation PowerpointApet Satusembilansembilan JieNo ratings yet
- @canotes - Final Customs Question Bank May, Nov 20 by ICAI PDFDocument111 pages@canotes - Final Customs Question Bank May, Nov 20 by ICAI PDFPraneelNo ratings yet
- P1-F Revision For Midyear - Listening - The Sydney Opera HouseDocument4 pagesP1-F Revision For Midyear - Listening - The Sydney Opera HouseYusuf Can SözerNo ratings yet
- 6.5mm GrendelDocument3 pages6.5mm GrendelErich EshelmanNo ratings yet
- ChirdsDocument5 pagesChirdsWise FidelityNo ratings yet
- Crochet A Deer Pattern in 20 Minutes.Document17 pagesCrochet A Deer Pattern in 20 Minutes.Maria Elisa BalestriniNo ratings yet
- Production For Consultants v34 - Upload VersionDocument270 pagesProduction For Consultants v34 - Upload VersionsubquangaddNo ratings yet
- Food Fraud and Adulteration in ChinaDocument7 pagesFood Fraud and Adulteration in ChinaToroPolacoNo ratings yet
- Dexter 1x01 - PilotDocument67 pagesDexter 1x01 - PilotmarkayartNo ratings yet
- Cardiac Insufficiency Bisoprolol Study (CIBIS III) TrialDocument6 pagesCardiac Insufficiency Bisoprolol Study (CIBIS III) TrialClaudia TiffanyNo ratings yet
- Quality Control of Ready Mixed Concrete Can Be Divided Into Three Convenient Areas LikeDocument11 pagesQuality Control of Ready Mixed Concrete Can Be Divided Into Three Convenient Areas Likeee iabNo ratings yet
- Envi Scie QuizDocument5 pagesEnvi Scie QuizJenemarNo ratings yet
- Zirconium and Zirconium Alloy Strip, Sheet, and Plate: Standard Specification ForDocument10 pagesZirconium and Zirconium Alloy Strip, Sheet, and Plate: Standard Specification ForTuanbk NguyenNo ratings yet
- Week1 FAQ-2Document6 pagesWeek1 FAQ-2Baldau Gupta0% (1)
- FMG 4-24-13 Christopher McDaniel-CSI Technologies-Cement Spacer Design and TestingDocument20 pagesFMG 4-24-13 Christopher McDaniel-CSI Technologies-Cement Spacer Design and TestingDoni KurniawanNo ratings yet
- TO Bus Rapid Transit (BRT) System: Hemant TiwariDocument48 pagesTO Bus Rapid Transit (BRT) System: Hemant TiwariHemant Tiwari100% (2)
- Book - Chap.on - Renewableenergyandwastewater 2 36Document36 pagesBook - Chap.on - Renewableenergyandwastewater 2 36Layth ZubairiNo ratings yet
- Septic Tank DetailsDocument1 pageSeptic Tank DetailsEdciel EbuenNo ratings yet
- Corrosion Probe TypeDocument26 pagesCorrosion Probe TypeFirman MuttaqinNo ratings yet
- Antimony Leaching From Polyethylene Terephthalate (PET) Plastic Used For Bottled Drinking WaterDocument6 pagesAntimony Leaching From Polyethylene Terephthalate (PET) Plastic Used For Bottled Drinking WaterjesicagabrNo ratings yet
- Gillies Main MenuDocument2 pagesGillies Main MenugalgormNo ratings yet
- CID Foundation Only PermitDocument1 pageCID Foundation Only PermitOsvaldo CalderonUACJNo ratings yet
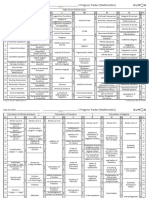
- Kumon Mathematics Progress Tracker Levels C To O PDFDocument2 pagesKumon Mathematics Progress Tracker Levels C To O PDFcharmradeekNo ratings yet