Download as pdf or txt
You might also like
- Succinct Pediatrics Evaluation and Management For Common and Critical Care 1st EditionDocument846 pagesSuccinct Pediatrics Evaluation and Management For Common and Critical Care 1st EditionMuhammad IkbarNo ratings yet
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- End of Course Assessment Review PracticeDocument194 pagesEnd of Course Assessment Review PracticeyoniNo ratings yet
- Abacus Mind Math Instruction Book Level 1: Step by Step Guide To Excel at Mind Math With Soroban, A Japanese Abacus (Volume 1)Document1 pageAbacus Mind Math Instruction Book Level 1: Step by Step Guide To Excel at Mind Math With Soroban, A Japanese Abacus (Volume 1)yasmin33% (3)
- Packrat 14 PDFDocument86 pagesPackrat 14 PDFkat100% (1)
- w13 RonaldDocument3 pagesw13 RonaldRonald LopezNo ratings yet
- Case Report Chronic LBP - P4Document14 pagesCase Report Chronic LBP - P4Sushi AfonsoNo ratings yet
- Asuhan Kefarmasian: Ahmad SalehDocument45 pagesAsuhan Kefarmasian: Ahmad SalehDjunaiddin FarmasiNo ratings yet
- NCM 109-NCP - PeregrinoDocument2 pagesNCM 109-NCP - PeregrinoJOYCE ANN PEREGRINONo ratings yet
- Head Nursing TemplateDocument10 pagesHead Nursing TemplateBianca MaeNo ratings yet
- Pelayanan Home CareDocument21 pagesPelayanan Home CareanggitaNo ratings yet
- Par Diagnostic Si TratamentDocument8 pagesPar Diagnostic Si TratamentValeria BostanNo ratings yet
- 65 - Approach To Patients With CancerDocument1 page65 - Approach To Patients With CancerRica Alyssa PepitoNo ratings yet
- Articulo Tto FibromialgiaDocument5 pagesArticulo Tto Fibromialgiadaniella FloresNo ratings yet
- Psoriasis AlgorithmDocument1 pagePsoriasis AlgorithmSeun MosesNo ratings yet
- Subacute Low Back PainDocument49 pagesSubacute Low Back Painsayid najibullahNo ratings yet
- JUVENILE IDIOPATHIC ARTHRITIS (JIA) : Introduction and Physical Therapy ManagementDocument1 pageJUVENILE IDIOPATHIC ARTHRITIS (JIA) : Introduction and Physical Therapy ManagementTushar SharmaNo ratings yet
- NCP PeregrinoDocument2 pagesNCP PeregrinoJOYCE ANN PEREGRINONo ratings yet
- CJSSDocument3 pagesCJSSj5khdwgywwNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Intervention EvaluationDocument4 pagesNursing Care Plan: Assessment Diagnosis Planning Intervention EvaluationPrincess LabasanNo ratings yet
- Ion of Risp Eridone IsDocument2 pagesIon of Risp Eridone IsKwin SaludaresNo ratings yet
- Jama - Management Parkisons DiseaseDocument2 pagesJama - Management Parkisons DiseaseLaura A. M. MontouroNo ratings yet
- Activity 4 F PsychiaLab DrugStudyDocument36 pagesActivity 4 F PsychiaLab DrugStudyVinz OñoNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanSiena KaleiNo ratings yet
- Diagnosis Schizophrenia 2Document1 pageDiagnosis Schizophrenia 2Bukola OgunnaikeNo ratings yet
- Psychotherapy Found Generally Effective For Borderline Personality Disorder - Psychiatric NewsDocument5 pagesPsychotherapy Found Generally Effective For Borderline Personality Disorder - Psychiatric NewsJosnelly HosoomelNo ratings yet
- Ra UpdateDocument28 pagesRa Updateqayyum consultantfpscNo ratings yet
- Haloperidol: College of Health SciencesDocument2 pagesHaloperidol: College of Health SciencesKervy JuntillaNo ratings yet
- Principles of Pain Management: Pediatric GuideDocument2 pagesPrinciples of Pain Management: Pediatric Guideblaziken123No ratings yet
- Neck Pain ProtocolsDocument3 pagesNeck Pain Protocolsrizk86No ratings yet
- Behavioral Health Care PlanDocument12 pagesBehavioral Health Care Planapi-520841770100% (1)
- Methadone HCLDocument2 pagesMethadone HCLtiffanald50% (2)
- Asuhan KefarmasianDocument45 pagesAsuhan KefarmasianEllan EltitahNo ratings yet
- Review of CBTDocument11 pagesReview of CBTSyeda AlizaNo ratings yet
- DRUG STUDY (Zuclopenthixol Decanoate) - SANGUYO, CB.Document5 pagesDRUG STUDY (Zuclopenthixol Decanoate) - SANGUYO, CB.Camille SanguyoNo ratings yet
- 10 Consejos en La SedacionDocument3 pages10 Consejos en La SedacionAntonio AlonsoNo ratings yet
- Lidocaine and Bupivacaine Local AnesthesiaDocument2 pagesLidocaine and Bupivacaine Local AnesthesiaEmer NicolasNo ratings yet
- Di Abetes Insipidus: Collaboration & Referral - PhysicianDocument1 pageDi Abetes Insipidus: Collaboration & Referral - PhysicianDaisy Jane KoNo ratings yet
- DISH TreatmentDocument6 pagesDISH TreatmentBorsecNo ratings yet
- Drug Study (Newborn Screening)Document2 pagesDrug Study (Newborn Screening)Aaron Christian AlmoiteNo ratings yet
- Depression in Dialysis: ReviewDocument13 pagesDepression in Dialysis: ReviewDoc RuthNo ratings yet
- NRN 202 Concept Map Patho-Altered Mental StatusDocument1 pageNRN 202 Concept Map Patho-Altered Mental StatusWendy Gilbert50% (2)
- The Reappraisal of Benzodiazepines in The Treatment of Anxiety and Related DisordersDocument12 pagesThe Reappraisal of Benzodiazepines in The Treatment of Anxiety and Related DisordersI SNo ratings yet
- Brief Cognitive Therapy For Avoidant Personality DisorderDocument11 pagesBrief Cognitive Therapy For Avoidant Personality DisorderCMSNo ratings yet
- Can Pyridoxine Successfully Reduce Behavioral Side.15Document4 pagesCan Pyridoxine Successfully Reduce Behavioral Side.15ilonaskorinNo ratings yet
- ADR ReportingDocument1 pageADR ReportingPrakash GuptaNo ratings yet
- Asuhan KefarmasianDocument45 pagesAsuhan Kefarmasiankamar obat pkm tamanNo ratings yet
- Drug Study (Acetaminophen)Document1 pageDrug Study (Acetaminophen)Kian HerreraNo ratings yet
- Asthma Interactive0712Document87 pagesAsthma Interactive0712Putri AyuNo ratings yet
- Practice A Mental HDocument1 pagePractice A Mental HroNo ratings yet
- ConceptmapDocument1 pageConceptmapapi-406249579No ratings yet
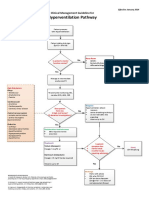
- Hyperventilation CMGDocument1 pageHyperventilation CMGizzati94No ratings yet
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDocument4 pagesKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNo ratings yet
- 2019-20159-008 TabDocument30 pages2019-20159-008 TabLuciana OliveiraNo ratings yet
- Ards DSDocument11 pagesArds DSP BNo ratings yet
- Jurnal Polifarmasi BipolarDocument18 pagesJurnal Polifarmasi BipolarDeisy KesumawatiNo ratings yet
- Div Class Title A Retrospective Examination of Care Pathways in Individuals With Treatment Resistant Depression DivDocument11 pagesDiv Class Title A Retrospective Examination of Care Pathways in Individuals With Treatment Resistant Depression DivSamanNo ratings yet
- Nursing Care Plan: HypertensionDocument3 pagesNursing Care Plan: HypertensionJasmin T. RegaspiNo ratings yet
- Pain Agitation and Delirium (PAD) UHL Critical Care GuidelineDocument35 pagesPain Agitation and Delirium (PAD) UHL Critical Care GuidelineLollapallooza 23No ratings yet
- Neuroleptic Malignant Syndrome A Guide For PsychiatristsDocument10 pagesNeuroleptic Malignant Syndrome A Guide For Psychiatristssari azzahroNo ratings yet
- Perioperative Pain ManagementFrom EverandPerioperative Pain ManagementFelicia CoxNo ratings yet
- Basic Biostatistics for Geneticists and Epidemiologists: A Practical ApproachFrom EverandBasic Biostatistics for Geneticists and Epidemiologists: A Practical ApproachNo ratings yet
- 2010 Drug-Induced Long QT SyndromeDocument22 pages2010 Drug-Induced Long QT SyndromeyasminNo ratings yet
- Soroban Exercises SVFPFKDocument1 pageSoroban Exercises SVFPFKyasminNo ratings yet
- ValidityDocument1 pageValidityyasminNo ratings yet
- DR - Yasamin Ali Bashar Arab Board Trainee Family MedicineDocument11 pagesDR - Yasamin Ali Bashar Arab Board Trainee Family MedicineyasminNo ratings yet
- Criterios de Clsificacion de Espondilitis AnquilosanteDocument16 pagesCriterios de Clsificacion de Espondilitis AnquilosanteWilkerson PerezNo ratings yet
- Drug Study - Nalbuphine (Nubain)Document3 pagesDrug Study - Nalbuphine (Nubain)Maria Theresa BuscasNo ratings yet
- Pulmonary Embolism and Deep Vein Thrombosis: Christopher KabrhelDocument23 pagesPulmonary Embolism and Deep Vein Thrombosis: Christopher KabrhelMukhtar AhmedNo ratings yet
- Psoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHADocument50 pagesPsoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHAEng Abdikariim AbdillahiNo ratings yet
- BDS 2ND Year New SchemeDocument3 pagesBDS 2ND Year New SchemeSumeet SodhiNo ratings yet
- Diploma in AcccupressureDocument7 pagesDiploma in AcccupressureKishore TadinadaNo ratings yet
- SUMAOANG - Maalox Drug StudyDocument4 pagesSUMAOANG - Maalox Drug StudyMina SumaoangNo ratings yet
- Smith Lemli Optiz Syndrome Group 7Document10 pagesSmith Lemli Optiz Syndrome Group 7EULA MARIE JOVERNo ratings yet
- Respiratory System: Copd (Bronchitis & Emphysema)Document7 pagesRespiratory System: Copd (Bronchitis & Emphysema)Rhea Lyn LamosteNo ratings yet
- Diabetes Mellitus and Pancreatitis - Cause or EffectDocument10 pagesDiabetes Mellitus and Pancreatitis - Cause or EffectRoberto Gutiérrez GonzálezNo ratings yet
- Alcoholic Liver DiseaseDocument21 pagesAlcoholic Liver DiseaseInsta GrammerNo ratings yet
- Calba Syst Review Surv PublishedDocument13 pagesCalba Syst Review Surv PublishedDian Muspitaloka HikmayatiNo ratings yet
- A. Facial Mask B. Non-Rebreather Mask C. Venturi MaskDocument17 pagesA. Facial Mask B. Non-Rebreather Mask C. Venturi Maskshivani kaushalNo ratings yet
- Ultrasonography of The Neck: O. Taeymans, DVM, Dip ECVDIDocument73 pagesUltrasonography of The Neck: O. Taeymans, DVM, Dip ECVDIKSNo ratings yet
- Ijtk 18 (2) 299-303Document5 pagesIjtk 18 (2) 299-303BARATHNo ratings yet
- Empirical Antibiotic Therapy in Children: Clinical GuidelineDocument2 pagesEmpirical Antibiotic Therapy in Children: Clinical GuidelineAna-Mihaela BalanuțaNo ratings yet
- Sample Healing With The Medicine of The Prophet PbuhDocument22 pagesSample Healing With The Medicine of The Prophet PbuhMaiyegun Nafisah AbiolaNo ratings yet
- Simple Ways To Test Dogs For Rabies - 9 Steps (With Pictures)Document5 pagesSimple Ways To Test Dogs For Rabies - 9 Steps (With Pictures)kaminiNo ratings yet
- Case of Grade 4 Bedsore Over Sacral Region With Management A Case ReportDocument3 pagesCase of Grade 4 Bedsore Over Sacral Region With Management A Case ReportAmna AliNo ratings yet
- CASE REPORT Rhinitis AlergyDocument36 pagesCASE REPORT Rhinitis AlergySiti MunirahNo ratings yet
- Hyperthermia Case StudyDocument28 pagesHyperthermia Case StudyJanelle GimenezNo ratings yet
- Subsection 2: Warranty Against Hidden Defects of or Encumbrances Upon The Thing Sold (Part 2)Document11 pagesSubsection 2: Warranty Against Hidden Defects of or Encumbrances Upon The Thing Sold (Part 2)WenjunNo ratings yet
- DR Lana Sundac - LGRS Urinary Tract InfectionsDocument4 pagesDR Lana Sundac - LGRS Urinary Tract Infectionsoxford_commaNo ratings yet
- Oral Medicine (PDFDrive)Document166 pagesOral Medicine (PDFDrive)Tasha FarahNo ratings yet
- Natural History OF Disease: Prepared by Krupa Mathew. M, Assistant ProfessorDocument25 pagesNatural History OF Disease: Prepared by Krupa Mathew. M, Assistant Professorkrupa mathewNo ratings yet
- Central Precocious Puberty: Revisiting The Diagnosis and Therapeutic ManagementDocument11 pagesCentral Precocious Puberty: Revisiting The Diagnosis and Therapeutic ManagementRESIDENCIA PEDIATRIANo ratings yet
- Velez College - Nursing F. Ramos ST., Cebu CityDocument26 pagesVelez College - Nursing F. Ramos ST., Cebu Cityfebie pachecoNo ratings yet
- Fluarix Tetra: 1. Name of Medicinal ProductDocument10 pagesFluarix Tetra: 1. Name of Medicinal ProductTeravut SuwansawaipholNo ratings yet