Download as pdf or txt
You might also like
- Mystical Stitches Downloadable PDFDocument51 pagesMystical Stitches Downloadable PDFJudit Lozano Peiró67% (3)
- Field Guide To Lens DesignDocument158 pagesField Guide To Lens DesignTasawar Khan JadoonNo ratings yet
- Air Pollution - Its Effects On Human Health and How To Improve ItDocument12 pagesAir Pollution - Its Effects On Human Health and How To Improve ItBeanzi LeiNo ratings yet
- Respiratory Tract Infections and Associated Environmental Factors in Port Harcourt MetropolisDocument10 pagesRespiratory Tract Infections and Associated Environmental Factors in Port Harcourt Metropolisijmb333No ratings yet
- Children's Vulnerability To Environmental Health An OverviewDocument4 pagesChildren's Vulnerability To Environmental Health An OverviewKIU PUBLICATION AND EXTENSIONNo ratings yet
- Task 2 - Identification of A Specific Problematic SituationDocument11 pagesTask 2 - Identification of A Specific Problematic SituationMayra Alejandra Quintero ValenciaNo ratings yet
- Landri Ingles WorkDocument13 pagesLandri Ingles WorkMilagros MartinezNo ratings yet
- Municipal Solid Waste Management and Adverse Health Outcomes: A Systematic ReviewDocument28 pagesMunicipal Solid Waste Management and Adverse Health Outcomes: A Systematic ReviewClaudio CostaNo ratings yet
- Ezati 2002 - Review - The Health Impacts of Exposure To Indoor Air Pollution From Solid Fuels inDocument12 pagesEzati 2002 - Review - The Health Impacts of Exposure To Indoor Air Pollution From Solid Fuels ineuripideavokpahoNo ratings yet
- Preventing Disease 5Document24 pagesPreventing Disease 5Dan KwekuNo ratings yet
- Diseases Due To Unhealthy Environments: An Updated Estimate of The Global Burden of Disease Attributable To Environmental Determinants of HealthDocument12 pagesDiseases Due To Unhealthy Environments: An Updated Estimate of The Global Burden of Disease Attributable To Environmental Determinants of HealthcthjgfytvfnoNo ratings yet
- Mercita Q. Queddeng: Incidence of Respiratory Diseases As Related To The Environmental Hazards in Region IDocument11 pagesMercita Q. Queddeng: Incidence of Respiratory Diseases As Related To The Environmental Hazards in Region IMaureen Joy Cascayan EspirituNo ratings yet
- Aqi 2Document11 pagesAqi 2Even AmsikanNo ratings yet
- Hernndez-Gordillo2021 Article RecentAdvancementsInLow-costPoDocument22 pagesHernndez-Gordillo2021 Article RecentAdvancementsInLow-costPozarrarhaiderabulkhairiNo ratings yet
- MODULE 17 Part1 Slides PDFDocument30 pagesMODULE 17 Part1 Slides PDFMuhammad Akmal HossainNo ratings yet
- Task 4 - Final Evaluation - ColoaborativoDocument13 pagesTask 4 - Final Evaluation - ColoaborativoKATERINENo ratings yet
- Environmental Research: Review ArticleDocument7 pagesEnvironmental Research: Review ArticleMaria Jose Altamirano CastroNo ratings yet
- Science of The Total EnvironmentDocument5 pagesScience of The Total EnvironmentJoel E ValenciaNo ratings yet
- Enfermedades de Tranms. AlimentariaDocument8 pagesEnfermedades de Tranms. AlimentariaAlejandra Dominguez RazoNo ratings yet
- State of The Art: Fiona C. Goldizen,, Peter D. Sly,, and Luke D. KnibbsDocument15 pagesState of The Art: Fiona C. Goldizen,, Peter D. Sly,, and Luke D. KnibbsKarina Aguirre AlvarezNo ratings yet
- What Does Risk' Mean in Municipal Solid Waste Management?Document20 pagesWhat Does Risk' Mean in Municipal Solid Waste Management?Juan Antonio Araiza AguilarNo ratings yet
- Ezzati Kammen 2001 Quantifying The Effects of Exposure To Indoor Air Pollution From Biomass CombustDocument8 pagesEzzati Kammen 2001 Quantifying The Effects of Exposure To Indoor Air Pollution From Biomass CombustsabriNo ratings yet
- Environmental Pollution and The Global Burden of Disease: David BriggsDocument24 pagesEnvironmental Pollution and The Global Burden of Disease: David BriggsFerly OktriyediNo ratings yet
- Global, National, and Urban Burdens of Paediatric Asthma Incidence Attributable To Ambient NO2 Pollution: Estimates From Global DatasetsDocument13 pagesGlobal, National, and Urban Burdens of Paediatric Asthma Incidence Attributable To Ambient NO2 Pollution: Estimates From Global DatasetsCTV Vancouver100% (1)
- The Joint Associations of Ambient Air Pollutants and Weathe - 2024 - Science ofDocument10 pagesThe Joint Associations of Ambient Air Pollutants and Weathe - 2024 - Science ofDana MateiNo ratings yet
- Assengment Community Health Ahmed Mohamed SaladDocument4 pagesAssengment Community Health Ahmed Mohamed SaladAhmed Mohammed salaadNo ratings yet
- Anca Maria Moldoveanu Editor Air Pollution - New DevelopmentsDocument334 pagesAnca Maria Moldoveanu Editor Air Pollution - New Developmentsنيرمين احمدNo ratings yet
- Preview PDFDocument163 pagesPreview PDFSameer NepalNo ratings yet
- Perceived Impact of Air Quality and Its Implications For A Sustainable Environment in Rivers StateDocument10 pagesPerceived Impact of Air Quality and Its Implications For A Sustainable Environment in Rivers StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AttachmentDocument7 pagesAttachmentdurojauyeNo ratings yet
- Review: Junfeng Zhang, Denise L Mauzerall, Tong Zhu, Song Liang, Majid Ezzati, Justin V RemaisDocument10 pagesReview: Junfeng Zhang, Denise L Mauzerall, Tong Zhu, Song Liang, Majid Ezzati, Justin V RemaisKarina Aguirre AlvarezNo ratings yet
- Chapter IDocument15 pagesChapter Ichn pastranaNo ratings yet
- Grupo VIDocument11 pagesGrupo VILuís ChongololaNo ratings yet
- Effectiveness of Planned Teaching Programme On Knowledge Regarding Environmental Health Among Women in Selected Setting, ChennaiDocument3 pagesEffectiveness of Planned Teaching Programme On Knowledge Regarding Environmental Health Among Women in Selected Setting, ChennaiEditor IJTSRDNo ratings yet
- Pollen AbortionDocument9 pagesPollen AbortionLuis F AmatoNo ratings yet
- Environmental Health Hazards Today and FutureDocument44 pagesEnvironmental Health Hazards Today and FuturePrince JoseNo ratings yet
- The Lancet Commissions: Executive SummaryDocument51 pagesThe Lancet Commissions: Executive SummaryHeera PaulNo ratings yet
- 2020 Wastewater Treatment Plant Workers Exposure and Methods For Risk Evaluation of Their ExposureDocument10 pages2020 Wastewater Treatment Plant Workers Exposure and Methods For Risk Evaluation of Their ExposureAna CamachoNo ratings yet
- Chapter 2.3 Environmental Impacts and Health Risks: Notes On This ChapterDocument3 pagesChapter 2.3 Environmental Impacts and Health Risks: Notes On This ChapterEr Barun SoniNo ratings yet
- Pollution Knows No BordersDocument54 pagesPollution Knows No Bordersmagizh tamizhiniNo ratings yet
- Dispersion Modeling of Traffic-Related Air Pollutant Exposures and Health Effects Among Children With Asthma in Detroit, MichiganDocument9 pagesDispersion Modeling of Traffic-Related Air Pollutant Exposures and Health Effects Among Children With Asthma in Detroit, MichiganSoumitaNo ratings yet
- 2019 PE - PollutionKnowsNoBordersOnlineDocument54 pages2019 PE - PollutionKnowsNoBordersOnlinefrank HuepeNo ratings yet
- 2023 TFOS Lifestyle Report - Environmental ConditionDocument52 pages2023 TFOS Lifestyle Report - Environmental Conditionrisingsun9823No ratings yet
- Environmental HealthDocument3 pagesEnvironmental HealthoisloeNo ratings yet
- EAWAG SANDEC 2008 Sandec Training Tool Module 2 Environmental Health LectureDocument37 pagesEAWAG SANDEC 2008 Sandec Training Tool Module 2 Environmental Health LectureEddiemtongaNo ratings yet
- Environmental Justice and Undeserved Communities (Pollutants)Document16 pagesEnvironmental Justice and Undeserved Communities (Pollutants)Juan CardenasNo ratings yet
- Chiabai Et Al 2020 Ecological EconomicsDocument10 pagesChiabai Et Al 2020 Ecological EconomicsSilvestre Garcia de JalonNo ratings yet
- Wildfire and Smoke Association With COVID-19 Cases in The Pantanal Wetland, BrazilDocument9 pagesWildfire and Smoke Association With COVID-19 Cases in The Pantanal Wetland, BrazilpaulofevrierNo ratings yet
- The Human Health Impact of Waste Management PractiDocument24 pagesThe Human Health Impact of Waste Management Practibelledelara68No ratings yet
- Breathe In, Breathe Out: Asthmatics and Environmental Challenges in Grand-Lome, TogoDocument7 pagesBreathe In, Breathe Out: Asthmatics and Environmental Challenges in Grand-Lome, TogoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S026974912201987X MainDocument12 pages1 s2.0 S026974912201987X Mainإكرام النايبNo ratings yet
- Hunt 2000 Review TextDocument25 pagesHunt 2000 Review TextCha GuingabNo ratings yet
- Document HasanDocument11 pagesDocument HasanHatem ShafelNo ratings yet
- BMC Infectious DiseasesDocument8 pagesBMC Infectious DiseasesrizkiNo ratings yet
- Geography Plagiarism CheckDocument5 pagesGeography Plagiarism Checkhum aur hamari lifeNo ratings yet
- 215 779 1 PBDocument8 pages215 779 1 PBSalsa BilaNo ratings yet
- Ehp 6334Document10 pagesEhp 6334Mohammad Zamir TaqwaNo ratings yet
- Pubs - Kovats.Wilkinson CAMBIO CLIMATICO EN ESPAÑADocument11 pagesPubs - Kovats.Wilkinson CAMBIO CLIMATICO EN ESPAÑAGregorio ChavezNo ratings yet
- Modern Environmental Health Hazards: A Public Health Issue of Increasing Significance in AfricaDocument9 pagesModern Environmental Health Hazards: A Public Health Issue of Increasing Significance in AfricaIman SuwonoNo ratings yet
- Environmental Impact Assessment ReviewDocument10 pagesEnvironmental Impact Assessment ReviewPipe GonzalezNo ratings yet
- Advanced Topics in Environmental Health and Air Pollution Case StudiesDocument482 pagesAdvanced Topics in Environmental Health and Air Pollution Case StudiesMicaelutza MicaNo ratings yet
- National Guidelines For DATA QUALITY in SurveysDocument112 pagesNational Guidelines For DATA QUALITY in SurveysBidhubhusan MahapatraNo ratings yet
- Performance IndicatorsDocument90 pagesPerformance IndicatorsBidhubhusan MahapatraNo ratings yet
- VAF Population Survey 2023Document83 pagesVAF Population Survey 2023Bidhubhusan MahapatraNo ratings yet
- PRM FY-2023-PRM-General-NGO-GuidelinesDocument100 pagesPRM FY-2023-PRM-General-NGO-GuidelinesBidhubhusan MahapatraNo ratings yet
- Ryerson EthicsDocument20 pagesRyerson EthicssinghbabaNo ratings yet
- Head and Shoulders by Nausherwan Khan NiaziDocument27 pagesHead and Shoulders by Nausherwan Khan NiaziNausherwan Khan Niazi50% (2)
- 1 - Hassanpour Et Al., 2011. Plants and Secondary Metabolites (Tannins) A ReviewDocument7 pages1 - Hassanpour Et Al., 2011. Plants and Secondary Metabolites (Tannins) A ReviewFelipe Reyes PeñaililloNo ratings yet
- CHECKLIST OF REQUIREMENTS Annex CDocument1 pageCHECKLIST OF REQUIREMENTS Annex CLaarni RamirezNo ratings yet
- Reminder Card Booklet v13 Print FinalDocument8 pagesReminder Card Booklet v13 Print FinalMayur MulyeNo ratings yet
- Mini Paper Company Profile by Decky M.A (19110115)Document14 pagesMini Paper Company Profile by Decky M.A (19110115)Adelia FebriantiNo ratings yet
- THS Yearbook 1986Document88 pagesTHS Yearbook 1986Tiskilwa Historical SocietyNo ratings yet
- Cloud, David. For Love of The BibleDocument509 pagesCloud, David. For Love of The BiblePavelNo ratings yet
- 3 PTSD Checklist and ScoringDocument2 pages3 PTSD Checklist and ScoringAnchita KhuranaNo ratings yet
- 034 Liwag v. Happy Glen Loop Homeowners Association, Inc.Document6 pages034 Liwag v. Happy Glen Loop Homeowners Association, Inc.Alvin John Dela LunaNo ratings yet
- A Hero Is Someone Who Understands The Responsibility That Comes With His FreedomDocument2 pagesA Hero Is Someone Who Understands The Responsibility That Comes With His FreedomellyabNo ratings yet
- Fungal NutritionDocument3 pagesFungal NutritionArtemishaMtzNo ratings yet
- Pon Pure Chemical - R-31082018Document8 pagesPon Pure Chemical - R-31082018Games ZoneNo ratings yet
- History of BankingDocument14 pagesHistory of Bankingrajeshpathak9No ratings yet
- STRAMADocument4 pagesSTRAMALimuel Talastas DeguzmanNo ratings yet
- Angelo de DonatisDocument6 pagesAngelo de DonatisNandu RaviNo ratings yet
- PMBOK Guide 5th Edition - NotesDocument50 pagesPMBOK Guide 5th Edition - NotesJoaoCOS100% (1)
- ContinueDocument3 pagesContinueNeeraj SharmaNo ratings yet
- In Re Hill Trustees Preliminary Recommendation On Sanctions For Leslie PUIDA and GMM 17 Nov 2010Document9 pagesIn Re Hill Trustees Preliminary Recommendation On Sanctions For Leslie PUIDA and GMM 17 Nov 2010William A. Roper Jr.No ratings yet
- Female Psychology A-Z FREE GuideDocument37 pagesFemale Psychology A-Z FREE Guideklaus Beck100% (8)
- No Smoke Without FireDocument1 pageNo Smoke Without FireArdi Do0% (1)
- Discussion QuestionsDocument6 pagesDiscussion Questionselisha emilianNo ratings yet
- Elecciones Injustas, Una Cronología de Incidentes No Democráticos Desde 1999. Por Vladimir Chelminski (No Publicado)Document124 pagesElecciones Injustas, Una Cronología de Incidentes No Democráticos Desde 1999. Por Vladimir Chelminski (No Publicado)AgusGulman100% (1)
- (Download PDF) Fundamentals of Cost Accounting 7Th Edition William Lanen Full Chapter PDFDocument69 pages(Download PDF) Fundamentals of Cost Accounting 7Th Edition William Lanen Full Chapter PDFkqirajbelqis100% (7)
- Convection and Conduction Heat TransferDocument406 pagesConvection and Conduction Heat Transfertfemilian100% (2)
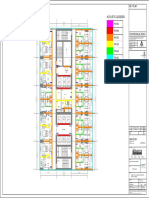
- Acoustic Legends:: Key PlanDocument1 pageAcoustic Legends:: Key PlanFaheem MushtaqNo ratings yet
- Antenatal Care (ANC)Document77 pagesAntenatal Care (ANC)tareNo ratings yet
- Weighted Least Squares Kinetic Upwind Method Using Eigen Vector BasisDocument55 pagesWeighted Least Squares Kinetic Upwind Method Using Eigen Vector BasiskonarkaroraNo ratings yet