
Taller Cirugía Preprotesica
Taller Cirugía Preprotesica
You might also like
- Spare Parts Catalog: 4 WG 160 Material Number: 4656.054.039 Current Date: 10.06.2020Document70 pagesSpare Parts Catalog: 4 WG 160 Material Number: 4656.054.039 Current Date: 10.06.2020Romuald Pogorzelczyk100% (2)
- ERTEKIN - & - ATIK - 2015 - Sustainable Markets - Motivating Factors, Barriers, and Remedies For Mobilization of Slow FashionDocument17 pagesERTEKIN - & - ATIK - 2015 - Sustainable Markets - Motivating Factors, Barriers, and Remedies For Mobilization of Slow FashionEstudanteSaxNo ratings yet
- Scenario Summary: Cost of Car Down Payment APR Years Monthly Payment Total To Repaid Total Interest PaidDocument5 pagesScenario Summary: Cost of Car Down Payment APR Years Monthly Payment Total To Repaid Total Interest PaidSomil GuptaNo ratings yet
- HPV-Vaccine Hesitancy in Colombia A Mixed-Methods StudyDocument16 pagesHPV-Vaccine Hesitancy in Colombia A Mixed-Methods Studyandrea sanabria pedrazaNo ratings yet
- XXXXDocument15 pagesXXXXpangaribuansantaNo ratings yet
- Effectiveness of Health Education Program On Knowledge and Attitude of Human Papillomavirus Vaccine in Female Adolescent Students in North-East MalaysiaDocument10 pagesEffectiveness of Health Education Program On Knowledge and Attitude of Human Papillomavirus Vaccine in Female Adolescent Students in North-East MalaysiaLili YaacobNo ratings yet
- Qi PlanDocument7 pagesQi Planapi-661765354No ratings yet
- Ijerph 15 00645Document13 pagesIjerph 15 00645Adam HafizNo ratings yet
- Fpubh 09 616456Document9 pagesFpubh 09 616456Berliana SitanggangNo ratings yet
- HPV Vaccination Acceptability in Young BoysDocument6 pagesHPV Vaccination Acceptability in Young BoyslupitaNo ratings yet
- Alder Et Al., 2015Document8 pagesAlder Et Al., 2015Balqis BaslemanNo ratings yet
- 1 s2.0 S2590136222000018 MainDocument12 pages1 s2.0 S2590136222000018 MainmariaNo ratings yet
- Assessment of Myths and Facts Associated With Covid 19 VaccinationDocument18 pagesAssessment of Myths and Facts Associated With Covid 19 Vaccinationnayab rafiqNo ratings yet
- HPV ObsosDocument5 pagesHPV ObsosRyan SadonoNo ratings yet
- Knowledge, Decision-Making and Acceptance of Human Papilloma Virus Vaccination Among Parents of Primary School Students in Kota Bharu, Kelantan, MalaysiaDocument6 pagesKnowledge, Decision-Making and Acceptance of Human Papilloma Virus Vaccination Among Parents of Primary School Students in Kota Bharu, Kelantan, MalaysiaMeidina DewatiNo ratings yet
- Behavioralinterventions PDFDocument11 pagesBehavioralinterventions PDFDeif MadNo ratings yet
- Knowledge, Attitude and Practices of Students Enrolled in Health Related Courses at Saint Louis University Towards Human Papillomavirus (Philippines)Document8 pagesKnowledge, Attitude and Practices of Students Enrolled in Health Related Courses at Saint Louis University Towards Human Papillomavirus (Philippines)Alexander DeckerNo ratings yet
- HPV VaccineDocument15 pagesHPV VaccineSimran ChauhanNo ratings yet
- VasavanSharangi Assign2Document11 pagesVasavanSharangi Assign2sharangiivNo ratings yet
- Articles: Kaja Abbas, Katelyn Jison Yoo, Kiesha Prem, and Mark JitDocument10 pagesArticles: Kaja Abbas, Katelyn Jison Yoo, Kiesha Prem, and Mark JitcapawatywidyNo ratings yet
- Proposal AnneDocument14 pagesProposal AnneLakshmi RjNo ratings yet
- Awareness of HPV and HPV Vaccines, Acceptance To VDocument6 pagesAwareness of HPV and HPV Vaccines, Acceptance To VMa. Isabel LadiaNo ratings yet
- Vaccine: Joan R. Cates, Sandra J. Diehl, Jamie L. Crandell, Tamera Coyne-BeasleyDocument8 pagesVaccine: Joan R. Cates, Sandra J. Diehl, Jamie L. Crandell, Tamera Coyne-BeasleyPAINEMNo ratings yet
- Literature Review - EditedDocument30 pagesLiterature Review - EditedOnesmus IgukuNo ratings yet
- Final Compilation - Group D ProjectDocument75 pagesFinal Compilation - Group D ProjectRukaiya Auwal AliNo ratings yet
- RESEARCH 1 Fi 2Document20 pagesRESEARCH 1 Fi 2Alondra SagarioNo ratings yet
- Cheruvu 2017 USADocument12 pagesCheruvu 2017 USAgabriela martinezNo ratings yet
- Articulo NorovirusDocument2 pagesArticulo Norovirusmarianagonzalezgil11No ratings yet
- Knowledge, Attitudes, and Behaviors of Parents Towards Varicella and Its VaccinationDocument8 pagesKnowledge, Attitudes, and Behaviors of Parents Towards Varicella and Its VaccinationkrishnasreeNo ratings yet
- Predicting Human Papillomavirus Vaccination Behaviour Among Adolescent Girls in England: Results From A Prospective SurveyDocument10 pagesPredicting Human Papillomavirus Vaccination Behaviour Among Adolescent Girls in England: Results From A Prospective SurveyVeronica Cordoba SanchezNo ratings yet
- Cagayan State University College of MedicineDocument28 pagesCagayan State University College of MedicineNhelia Santos BañagaNo ratings yet
- HPV DeliverableDocument9 pagesHPV DeliverableCAMILA LUCIANA LUNA VICTORIA RAMOSNo ratings yet
- HPVDocument4 pagesHPVAuboo7No ratings yet
- Keim-Malpass2017 - ApoiadoresDocument8 pagesKeim-Malpass2017 - ApoiadoresMarcella AndradeNo ratings yet
- The Impact of Health Education Interventions On HPV Vaccination Uptake, Awareness, and Acceptance Among People Under 30 Years Old in India: A Literature Review With Systematic SearchDocument11 pagesThe Impact of Health Education Interventions On HPV Vaccination Uptake, Awareness, and Acceptance Among People Under 30 Years Old in India: A Literature Review With Systematic SearchMargareta OktavianiNo ratings yet
- Vaccines 08 00124 PDFDocument21 pagesVaccines 08 00124 PDFSaúl Alberto Kohan BocNo ratings yet
- PIIS2214109X24000093Document2 pagesPIIS2214109X24000093MesutHasipiNo ratings yet
- JurnalDocument16 pagesJurnalTrysna Ayu SukardiNo ratings yet
- Acceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefDocument12 pagesAcceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefamalliaNo ratings yet
- Literature Review MMR VaccineDocument7 pagesLiterature Review MMR Vaccineafmzmxkayjyoso100% (1)
- Chapter I-1Document3 pagesChapter I-1Secret AdmirerNo ratings yet
- Final Program ProposalDocument8 pagesFinal Program Proposalotienocliff7No ratings yet
- Research PowerpointDocument14 pagesResearch Powerpointapi-546731047No ratings yet
- Research Paper On Child VaccinationsDocument7 pagesResearch Paper On Child Vaccinationspwvgqccnd100% (1)
- Factors Affecting COVID-19 Vaccine Acceptance: An International Survey Among Low-And Middle-Income CountriesDocument19 pagesFactors Affecting COVID-19 Vaccine Acceptance: An International Survey Among Low-And Middle-Income Countriesmercadia5997No ratings yet
- Human Papillomavirus Vaccine Effectiveness by Age at Vaccination A Systematic ReviewDocument20 pagesHuman Papillomavirus Vaccine Effectiveness by Age at Vaccination A Systematic ReviewdeasyarchikaalvaresNo ratings yet
- Factors Associated With Parents Willingness To Enroll Their Children in Trials For COVID 19 VaccinationDocument6 pagesFactors Associated With Parents Willingness To Enroll Their Children in Trials For COVID 19 VaccinationanitadwishantiNo ratings yet
- Key Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicDocument3 pagesKey Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicnpidasNo ratings yet
- 1 s2.0 S2210600612000597 MainDocument8 pages1 s2.0 S2210600612000597 MainpangaribuansantaNo ratings yet
- Attitude, Perception and Practice Towards Human Papilloma Virus Vaccination Among Nurses in The Federal Medical Centre, Abeokuta, Ogun State, NigeriaDocument18 pagesAttitude, Perception and Practice Towards Human Papilloma Virus Vaccination Among Nurses in The Federal Medical Centre, Abeokuta, Ogun State, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Efeito de Intervenção Educativa para Adesão de Adolescentes EscolaresDocument9 pagesEfeito de Intervenção Educativa para Adesão de Adolescentes EscolaresasdasdasdasNo ratings yet
- Parental Perceptions of The COVID 19 Vaccine For 5 To 11 Year Old Children Focus Group Findings From Worcester MassachusettsDocument10 pagesParental Perceptions of The COVID 19 Vaccine For 5 To 11 Year Old Children Focus Group Findings From Worcester MassachusettsIrene KoutsodontiNo ratings yet
- G2 Nursing Research FinalDocument26 pagesG2 Nursing Research FinalABELLO LAILA S.No ratings yet
- Effectiveness of A Third Dose of MMR Vaccine For Mumps Outbreak ControlDocument10 pagesEffectiveness of A Third Dose of MMR Vaccine For Mumps Outbreak ControlMuhammad FachrurozieNo ratings yet
- Chapter 25: Education, Training, and Communication For HPV VaccinesDocument9 pagesChapter 25: Education, Training, and Communication For HPV Vaccineshst939No ratings yet
- Do Parental Education and Income Matter? A Nationwide Register-Based Study On HPV Vaccine Uptake in The School-Based Immunisation Programme in NorwayDocument10 pagesDo Parental Education and Income Matter? A Nationwide Register-Based Study On HPV Vaccine Uptake in The School-Based Immunisation Programme in NorwayVeronica Cordoba SanchezNo ratings yet
- ART Pandemic Influenza Planning Addressing The Needs of ChildrenDocument6 pagesART Pandemic Influenza Planning Addressing The Needs of ChildrenMharianniNo ratings yet
- Amidst of PandemicDocument3 pagesAmidst of PandemicPATRICK GIGANTENo ratings yet
- HIV-positive Gay Men's Knowledge and Perceptions of Human Papillomavirus (HPV) and HPV Vaccination A Qualitative StudyDocument14 pagesHIV-positive Gay Men's Knowledge and Perceptions of Human Papillomavirus (HPV) and HPV Vaccination A Qualitative StudyLlamencio Kolotikpilli LlamaNo ratings yet
- HPV Vaccination CEADocument10 pagesHPV Vaccination CEAredrojo1987No ratings yet
- Health Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central JavaDocument11 pagesHealth Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central Javaadilla kusumaNo ratings yet
- Interventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsDocument10 pagesInterventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsMariaNo ratings yet
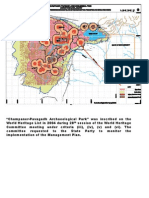
- Champaner and HampiDocument67 pagesChampaner and HampiKrisha Desai100% (2)
- (Download PDF) Networking and Kubernetes A Layered Approach 1St Edition James Strong Ebook Online Full ChapterDocument53 pages(Download PDF) Networking and Kubernetes A Layered Approach 1St Edition James Strong Ebook Online Full Chaptersiquancurte100% (5)
- Concert Report On Tchaikovsky's Fantasy-Overture 'Romeo and Juliet'Document13 pagesConcert Report On Tchaikovsky's Fantasy-Overture 'Romeo and Juliet'Hamdy Ahmed HassanNo ratings yet
- Assignment 1 (Internal Control)Document23 pagesAssignment 1 (Internal Control)Ali WaqarNo ratings yet
- Unit 6 - Automated Storage and Retrieval SystemsDocument11 pagesUnit 6 - Automated Storage and Retrieval Systemssri7877No ratings yet
- Pang-Yao-Professor Research-PjDocument4 pagesPang-Yao-Professor Research-Pjapi-510190176No ratings yet
- Math 270 5.4Document11 pagesMath 270 5.4airies mae orpianoNo ratings yet
- Biologic Considerations of Enamel Structure and Its Clinical Significance in Practice of Operative DentistryDocument25 pagesBiologic Considerations of Enamel Structure and Its Clinical Significance in Practice of Operative DentistryAmee PatelNo ratings yet
- Directors Report To The Shareholders of Idlc Finance Limited 2019 944529Document9 pagesDirectors Report To The Shareholders of Idlc Finance Limited 2019 944529sajibarafatsiddiquiNo ratings yet
- Photography QuestionnaireDocument2 pagesPhotography Questionnaires2sarathNo ratings yet
- Vis2ion EiglishDocument29 pagesVis2ion EiglishSandip Olee100% (1)
- Yokogawa: Y/11DM Pneumatic Differential Pressure Transmitter User's ManualDocument5 pagesYokogawa: Y/11DM Pneumatic Differential Pressure Transmitter User's ManualRabah AmidiNo ratings yet
- Project:SASEC Mugling-Pokhara Highway Improvement Phase I Project (SMPHIP) Contract No. SMPHIP/OCB/MAP/2 Contractor: Anhui Kaiyuan Highway and Bridge Co. LTDDocument4 pagesProject:SASEC Mugling-Pokhara Highway Improvement Phase I Project (SMPHIP) Contract No. SMPHIP/OCB/MAP/2 Contractor: Anhui Kaiyuan Highway and Bridge Co. LTDugrasen chaudharyNo ratings yet
- Econ 2D03 Outline F17 KabirDocument2 pagesEcon 2D03 Outline F17 Kabiraccount0% (1)
- Sasmo 2020 G8Document16 pagesSasmo 2020 G8Məhəmməd CəbrayıllıNo ratings yet
- UNIT 2 Reading Lesson PlanDocument7 pagesUNIT 2 Reading Lesson PlanThanh BlueNo ratings yet
- Hooverphonic Biography (2000)Document4 pagesHooverphonic Biography (2000)6980MulhollandDriveNo ratings yet
- Smith Et Al., 2018 (Analytical Chemistry)Document7 pagesSmith Et Al., 2018 (Analytical Chemistry)Leticia SakaiNo ratings yet
- Treasure and Dirt Chapter SamplerDocument33 pagesTreasure and Dirt Chapter SamplerAllen & Unwin0% (1)
- Geometry Volume - Cylinders - ConeDocument2 pagesGeometry Volume - Cylinders - ConemaheshwaNo ratings yet
- Engine Variant: V2527-A5Document12 pagesEngine Variant: V2527-A5Kartika Ningtyas100% (1)
- MPF Multi-Pole Automotive Fuses: Technical Data 10602Document2 pagesMPF Multi-Pole Automotive Fuses: Technical Data 10602Darren DeVoseNo ratings yet
- Lev Vygotsky PaperDocument7 pagesLev Vygotsky Paperapi-301414901No ratings yet
- 4th Unit Test Grade 8Document30 pages4th Unit Test Grade 8Ella Mae CabungcalNo ratings yet
- Hso422567 Issue2Document13 pagesHso422567 Issue2Александр ЩербаковNo ratings yet
- Max 487 Max 485 IcsDocument19 pagesMax 487 Max 485 IcsPra100% (1)
- NEC - 2017-10-26 - High Frequency TradingDocument53 pagesNEC - 2017-10-26 - High Frequency TradingAlexander GloyNo ratings yet
























































































Download as pdf or txt
You might also like
- Spare Parts Catalog: 4 WG 160 Material Number: 4656.054.039 Current Date: 10.06.2020Document70 pagesSpare Parts Catalog: 4 WG 160 Material Number: 4656.054.039 Current Date: 10.06.2020Romuald Pogorzelczyk100% (2)
- ERTEKIN - & - ATIK - 2015 - Sustainable Markets - Motivating Factors, Barriers, and Remedies For Mobilization of Slow FashionDocument17 pagesERTEKIN - & - ATIK - 2015 - Sustainable Markets - Motivating Factors, Barriers, and Remedies For Mobilization of Slow FashionEstudanteSaxNo ratings yet
- Scenario Summary: Cost of Car Down Payment APR Years Monthly Payment Total To Repaid Total Interest PaidDocument5 pagesScenario Summary: Cost of Car Down Payment APR Years Monthly Payment Total To Repaid Total Interest PaidSomil GuptaNo ratings yet
- HPV-Vaccine Hesitancy in Colombia A Mixed-Methods StudyDocument16 pagesHPV-Vaccine Hesitancy in Colombia A Mixed-Methods Studyandrea sanabria pedrazaNo ratings yet
- XXXXDocument15 pagesXXXXpangaribuansantaNo ratings yet
- Effectiveness of Health Education Program On Knowledge and Attitude of Human Papillomavirus Vaccine in Female Adolescent Students in North-East MalaysiaDocument10 pagesEffectiveness of Health Education Program On Knowledge and Attitude of Human Papillomavirus Vaccine in Female Adolescent Students in North-East MalaysiaLili YaacobNo ratings yet
- Qi PlanDocument7 pagesQi Planapi-661765354No ratings yet
- Ijerph 15 00645Document13 pagesIjerph 15 00645Adam HafizNo ratings yet
- Fpubh 09 616456Document9 pagesFpubh 09 616456Berliana SitanggangNo ratings yet
- HPV Vaccination Acceptability in Young BoysDocument6 pagesHPV Vaccination Acceptability in Young BoyslupitaNo ratings yet
- Alder Et Al., 2015Document8 pagesAlder Et Al., 2015Balqis BaslemanNo ratings yet
- 1 s2.0 S2590136222000018 MainDocument12 pages1 s2.0 S2590136222000018 MainmariaNo ratings yet
- Assessment of Myths and Facts Associated With Covid 19 VaccinationDocument18 pagesAssessment of Myths and Facts Associated With Covid 19 Vaccinationnayab rafiqNo ratings yet
- HPV ObsosDocument5 pagesHPV ObsosRyan SadonoNo ratings yet
- Knowledge, Decision-Making and Acceptance of Human Papilloma Virus Vaccination Among Parents of Primary School Students in Kota Bharu, Kelantan, MalaysiaDocument6 pagesKnowledge, Decision-Making and Acceptance of Human Papilloma Virus Vaccination Among Parents of Primary School Students in Kota Bharu, Kelantan, MalaysiaMeidina DewatiNo ratings yet
- Behavioralinterventions PDFDocument11 pagesBehavioralinterventions PDFDeif MadNo ratings yet
- Knowledge, Attitude and Practices of Students Enrolled in Health Related Courses at Saint Louis University Towards Human Papillomavirus (Philippines)Document8 pagesKnowledge, Attitude and Practices of Students Enrolled in Health Related Courses at Saint Louis University Towards Human Papillomavirus (Philippines)Alexander DeckerNo ratings yet
- HPV VaccineDocument15 pagesHPV VaccineSimran ChauhanNo ratings yet
- VasavanSharangi Assign2Document11 pagesVasavanSharangi Assign2sharangiivNo ratings yet
- Articles: Kaja Abbas, Katelyn Jison Yoo, Kiesha Prem, and Mark JitDocument10 pagesArticles: Kaja Abbas, Katelyn Jison Yoo, Kiesha Prem, and Mark JitcapawatywidyNo ratings yet
- Proposal AnneDocument14 pagesProposal AnneLakshmi RjNo ratings yet
- Awareness of HPV and HPV Vaccines, Acceptance To VDocument6 pagesAwareness of HPV and HPV Vaccines, Acceptance To VMa. Isabel LadiaNo ratings yet
- Vaccine: Joan R. Cates, Sandra J. Diehl, Jamie L. Crandell, Tamera Coyne-BeasleyDocument8 pagesVaccine: Joan R. Cates, Sandra J. Diehl, Jamie L. Crandell, Tamera Coyne-BeasleyPAINEMNo ratings yet
- Literature Review - EditedDocument30 pagesLiterature Review - EditedOnesmus IgukuNo ratings yet
- Final Compilation - Group D ProjectDocument75 pagesFinal Compilation - Group D ProjectRukaiya Auwal AliNo ratings yet
- RESEARCH 1 Fi 2Document20 pagesRESEARCH 1 Fi 2Alondra SagarioNo ratings yet
- Cheruvu 2017 USADocument12 pagesCheruvu 2017 USAgabriela martinezNo ratings yet
- Articulo NorovirusDocument2 pagesArticulo Norovirusmarianagonzalezgil11No ratings yet
- Knowledge, Attitudes, and Behaviors of Parents Towards Varicella and Its VaccinationDocument8 pagesKnowledge, Attitudes, and Behaviors of Parents Towards Varicella and Its VaccinationkrishnasreeNo ratings yet
- Predicting Human Papillomavirus Vaccination Behaviour Among Adolescent Girls in England: Results From A Prospective SurveyDocument10 pagesPredicting Human Papillomavirus Vaccination Behaviour Among Adolescent Girls in England: Results From A Prospective SurveyVeronica Cordoba SanchezNo ratings yet
- Cagayan State University College of MedicineDocument28 pagesCagayan State University College of MedicineNhelia Santos BañagaNo ratings yet
- HPV DeliverableDocument9 pagesHPV DeliverableCAMILA LUCIANA LUNA VICTORIA RAMOSNo ratings yet
- HPVDocument4 pagesHPVAuboo7No ratings yet
- Keim-Malpass2017 - ApoiadoresDocument8 pagesKeim-Malpass2017 - ApoiadoresMarcella AndradeNo ratings yet
- The Impact of Health Education Interventions On HPV Vaccination Uptake, Awareness, and Acceptance Among People Under 30 Years Old in India: A Literature Review With Systematic SearchDocument11 pagesThe Impact of Health Education Interventions On HPV Vaccination Uptake, Awareness, and Acceptance Among People Under 30 Years Old in India: A Literature Review With Systematic SearchMargareta OktavianiNo ratings yet
- Vaccines 08 00124 PDFDocument21 pagesVaccines 08 00124 PDFSaúl Alberto Kohan BocNo ratings yet
- PIIS2214109X24000093Document2 pagesPIIS2214109X24000093MesutHasipiNo ratings yet
- JurnalDocument16 pagesJurnalTrysna Ayu SukardiNo ratings yet
- Acceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefDocument12 pagesAcceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefamalliaNo ratings yet
- Literature Review MMR VaccineDocument7 pagesLiterature Review MMR Vaccineafmzmxkayjyoso100% (1)
- Chapter I-1Document3 pagesChapter I-1Secret AdmirerNo ratings yet
- Final Program ProposalDocument8 pagesFinal Program Proposalotienocliff7No ratings yet
- Research PowerpointDocument14 pagesResearch Powerpointapi-546731047No ratings yet
- Research Paper On Child VaccinationsDocument7 pagesResearch Paper On Child Vaccinationspwvgqccnd100% (1)
- Factors Affecting COVID-19 Vaccine Acceptance: An International Survey Among Low-And Middle-Income CountriesDocument19 pagesFactors Affecting COVID-19 Vaccine Acceptance: An International Survey Among Low-And Middle-Income Countriesmercadia5997No ratings yet
- Human Papillomavirus Vaccine Effectiveness by Age at Vaccination A Systematic ReviewDocument20 pagesHuman Papillomavirus Vaccine Effectiveness by Age at Vaccination A Systematic ReviewdeasyarchikaalvaresNo ratings yet
- Factors Associated With Parents Willingness To Enroll Their Children in Trials For COVID 19 VaccinationDocument6 pagesFactors Associated With Parents Willingness To Enroll Their Children in Trials For COVID 19 VaccinationanitadwishantiNo ratings yet
- Key Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicDocument3 pagesKey Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicnpidasNo ratings yet
- 1 s2.0 S2210600612000597 MainDocument8 pages1 s2.0 S2210600612000597 MainpangaribuansantaNo ratings yet
- Attitude, Perception and Practice Towards Human Papilloma Virus Vaccination Among Nurses in The Federal Medical Centre, Abeokuta, Ogun State, NigeriaDocument18 pagesAttitude, Perception and Practice Towards Human Papilloma Virus Vaccination Among Nurses in The Federal Medical Centre, Abeokuta, Ogun State, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Efeito de Intervenção Educativa para Adesão de Adolescentes EscolaresDocument9 pagesEfeito de Intervenção Educativa para Adesão de Adolescentes EscolaresasdasdasdasNo ratings yet
- Parental Perceptions of The COVID 19 Vaccine For 5 To 11 Year Old Children Focus Group Findings From Worcester MassachusettsDocument10 pagesParental Perceptions of The COVID 19 Vaccine For 5 To 11 Year Old Children Focus Group Findings From Worcester MassachusettsIrene KoutsodontiNo ratings yet
- G2 Nursing Research FinalDocument26 pagesG2 Nursing Research FinalABELLO LAILA S.No ratings yet
- Effectiveness of A Third Dose of MMR Vaccine For Mumps Outbreak ControlDocument10 pagesEffectiveness of A Third Dose of MMR Vaccine For Mumps Outbreak ControlMuhammad FachrurozieNo ratings yet
- Chapter 25: Education, Training, and Communication For HPV VaccinesDocument9 pagesChapter 25: Education, Training, and Communication For HPV Vaccineshst939No ratings yet
- Do Parental Education and Income Matter? A Nationwide Register-Based Study On HPV Vaccine Uptake in The School-Based Immunisation Programme in NorwayDocument10 pagesDo Parental Education and Income Matter? A Nationwide Register-Based Study On HPV Vaccine Uptake in The School-Based Immunisation Programme in NorwayVeronica Cordoba SanchezNo ratings yet
- ART Pandemic Influenza Planning Addressing The Needs of ChildrenDocument6 pagesART Pandemic Influenza Planning Addressing The Needs of ChildrenMharianniNo ratings yet
- Amidst of PandemicDocument3 pagesAmidst of PandemicPATRICK GIGANTENo ratings yet
- HIV-positive Gay Men's Knowledge and Perceptions of Human Papillomavirus (HPV) and HPV Vaccination A Qualitative StudyDocument14 pagesHIV-positive Gay Men's Knowledge and Perceptions of Human Papillomavirus (HPV) and HPV Vaccination A Qualitative StudyLlamencio Kolotikpilli LlamaNo ratings yet
- HPV Vaccination CEADocument10 pagesHPV Vaccination CEAredrojo1987No ratings yet
- Health Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central JavaDocument11 pagesHealth Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central Javaadilla kusumaNo ratings yet
- Interventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsDocument10 pagesInterventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsMariaNo ratings yet
- Champaner and HampiDocument67 pagesChampaner and HampiKrisha Desai100% (2)
- (Download PDF) Networking and Kubernetes A Layered Approach 1St Edition James Strong Ebook Online Full ChapterDocument53 pages(Download PDF) Networking and Kubernetes A Layered Approach 1St Edition James Strong Ebook Online Full Chaptersiquancurte100% (5)
- Concert Report On Tchaikovsky's Fantasy-Overture 'Romeo and Juliet'Document13 pagesConcert Report On Tchaikovsky's Fantasy-Overture 'Romeo and Juliet'Hamdy Ahmed HassanNo ratings yet
- Assignment 1 (Internal Control)Document23 pagesAssignment 1 (Internal Control)Ali WaqarNo ratings yet
- Unit 6 - Automated Storage and Retrieval SystemsDocument11 pagesUnit 6 - Automated Storage and Retrieval Systemssri7877No ratings yet
- Pang-Yao-Professor Research-PjDocument4 pagesPang-Yao-Professor Research-Pjapi-510190176No ratings yet
- Math 270 5.4Document11 pagesMath 270 5.4airies mae orpianoNo ratings yet
- Biologic Considerations of Enamel Structure and Its Clinical Significance in Practice of Operative DentistryDocument25 pagesBiologic Considerations of Enamel Structure and Its Clinical Significance in Practice of Operative DentistryAmee PatelNo ratings yet
- Directors Report To The Shareholders of Idlc Finance Limited 2019 944529Document9 pagesDirectors Report To The Shareholders of Idlc Finance Limited 2019 944529sajibarafatsiddiquiNo ratings yet
- Photography QuestionnaireDocument2 pagesPhotography Questionnaires2sarathNo ratings yet
- Vis2ion EiglishDocument29 pagesVis2ion EiglishSandip Olee100% (1)
- Yokogawa: Y/11DM Pneumatic Differential Pressure Transmitter User's ManualDocument5 pagesYokogawa: Y/11DM Pneumatic Differential Pressure Transmitter User's ManualRabah AmidiNo ratings yet
- Project:SASEC Mugling-Pokhara Highway Improvement Phase I Project (SMPHIP) Contract No. SMPHIP/OCB/MAP/2 Contractor: Anhui Kaiyuan Highway and Bridge Co. LTDDocument4 pagesProject:SASEC Mugling-Pokhara Highway Improvement Phase I Project (SMPHIP) Contract No. SMPHIP/OCB/MAP/2 Contractor: Anhui Kaiyuan Highway and Bridge Co. LTDugrasen chaudharyNo ratings yet
- Econ 2D03 Outline F17 KabirDocument2 pagesEcon 2D03 Outline F17 Kabiraccount0% (1)
- Sasmo 2020 G8Document16 pagesSasmo 2020 G8Məhəmməd CəbrayıllıNo ratings yet
- UNIT 2 Reading Lesson PlanDocument7 pagesUNIT 2 Reading Lesson PlanThanh BlueNo ratings yet
- Hooverphonic Biography (2000)Document4 pagesHooverphonic Biography (2000)6980MulhollandDriveNo ratings yet
- Smith Et Al., 2018 (Analytical Chemistry)Document7 pagesSmith Et Al., 2018 (Analytical Chemistry)Leticia SakaiNo ratings yet
- Treasure and Dirt Chapter SamplerDocument33 pagesTreasure and Dirt Chapter SamplerAllen & Unwin0% (1)
- Geometry Volume - Cylinders - ConeDocument2 pagesGeometry Volume - Cylinders - ConemaheshwaNo ratings yet
- Engine Variant: V2527-A5Document12 pagesEngine Variant: V2527-A5Kartika Ningtyas100% (1)
- MPF Multi-Pole Automotive Fuses: Technical Data 10602Document2 pagesMPF Multi-Pole Automotive Fuses: Technical Data 10602Darren DeVoseNo ratings yet
- Lev Vygotsky PaperDocument7 pagesLev Vygotsky Paperapi-301414901No ratings yet
- 4th Unit Test Grade 8Document30 pages4th Unit Test Grade 8Ella Mae CabungcalNo ratings yet
- Hso422567 Issue2Document13 pagesHso422567 Issue2Александр ЩербаковNo ratings yet
- Max 487 Max 485 IcsDocument19 pagesMax 487 Max 485 IcsPra100% (1)
- NEC - 2017-10-26 - High Frequency TradingDocument53 pagesNEC - 2017-10-26 - High Frequency TradingAlexander GloyNo ratings yet