Download as pdf or txt
You might also like
- American Board of Family Medicine: 2020 Questions & AnswersDocument112 pagesAmerican Board of Family Medicine: 2020 Questions & AnswersthanaaNo ratings yet
- Fascial SpacesDocument17 pagesFascial SpacesAlaa MoradNo ratings yet
- Viva PathologyDocument10 pagesViva PathologyKumar KP75% (4)
- Pathophysiology of Atrial FibrillationDocument12 pagesPathophysiology of Atrial FibrillationAndrew Surya Putra SccNo ratings yet
- Space Infection: Dr. Amit T. Suryawanshi Oral and Maxillofacial Surgeon Pune, India Contact Details: Email IDDocument121 pagesSpace Infection: Dr. Amit T. Suryawanshi Oral and Maxillofacial Surgeon Pune, India Contact Details: Email IDBinek NeupaneNo ratings yet
- Facial Space InfectionsDocument76 pagesFacial Space InfectionsPrathusha UmakhanthNo ratings yet
- Odontogenic Infection & Surgical ManagementDocument296 pagesOdontogenic Infection & Surgical ManagementYazid Eriansyah Pradanta100% (2)
- Space Infection - Theory ClassDocument264 pagesSpace Infection - Theory ClassMelese AbebeNo ratings yet
- Space InfectionDocument44 pagesSpace InfectionArun panwarNo ratings yet
- Space Infections: Dr. Amit Gupta Reader Department of Oral PathologyDocument54 pagesSpace Infections: Dr. Amit Gupta Reader Department of Oral PathologyAMIT GUPTANo ratings yet
- Diagnosis and Management of Odontogenic InfectionsDocument52 pagesDiagnosis and Management of Odontogenic InfectionsAhmed EmadNo ratings yet
- Deep Neck Infection1deep Neck Space InfectionDocument53 pagesDeep Neck Infection1deep Neck Space Infectionwhitelotusoo7No ratings yet
- Fascial SpacesDocument93 pagesFascial SpacesRobins Dhakal50% (2)
- Pariyanan Jaruchinda Department of Otolaryngology Phramongkutklao HospitalDocument40 pagesPariyanan Jaruchinda Department of Otolaryngology Phramongkutklao HospitalWidi HadiNo ratings yet
- Oro-Facial Infection and ManagementDocument80 pagesOro-Facial Infection and ManagementEticha EmbaboNo ratings yet
- Space InfectionsDocument60 pagesSpace InfectionsDan 04No ratings yet
- Facial SpacesDocument26 pagesFacial SpacesVadim Viţu0% (1)
- Odontogenic Infection Dentist6Document39 pagesOdontogenic Infection Dentist6Kimya Zand100% (1)
- InfectionDocument33 pagesInfectionHesham EljamlNo ratings yet
- Spread of Oral InfectionDocument67 pagesSpread of Oral InfectionAMIT GUPTANo ratings yet
- Odontogenic Infection EttingerDocument50 pagesOdontogenic Infection EttingerBunga Erlita RosaliaNo ratings yet
- Fascial Space InfectionsDocument28 pagesFascial Space InfectionsArun panwarNo ratings yet
- 10.0 Maxillofacial Infections: Learning OutcomesDocument10 pages10.0 Maxillofacial Infections: Learning OutcomesDentist Dina SamyNo ratings yet
- Maxillarysinus 170705134531 PDFDocument93 pagesMaxillarysinus 170705134531 PDFmelaniaNo ratings yet
- The PRINCIPLES in Management of ODONTOGEN InfectionDocument40 pagesThe PRINCIPLES in Management of ODONTOGEN InfectionRakenzon Adhi Sakti SantosaNo ratings yet
- Multiple Space Infection and Current Treatment StrategiesDocument30 pagesMultiple Space Infection and Current Treatment StrategiesSibaniNo ratings yet
- Chapter-18 - Orofacial Infection and Its SpreadDocument6 pagesChapter-18 - Orofacial Infection and Its Spreadbjahboi2No ratings yet
- M S I & C: Andibular Pace Nfections OmplicationsDocument89 pagesM S I & C: Andibular Pace Nfections OmplicationsArun panwarNo ratings yet
- Space Infections PDFDocument98 pagesSpace Infections PDFRamya ReddyNo ratings yet
- Abcesele Lojilor Profunde Și Flegmoanele OMFDocument58 pagesAbcesele Lojilor Profunde Și Flegmoanele OMFSalameh Abu MUSSANo ratings yet
- Deep Neck InfectionsDocument54 pagesDeep Neck InfectionsAmr ElsaadenyNo ratings yet
- Abses SubmandibularDocument17 pagesAbses Submandibularhoney_hannieNo ratings yet
- L25 Microbiology in EndodonticsDocument57 pagesL25 Microbiology in Endodonticselle70503No ratings yet
- Grand Rounds Index UTMB Otolaryngology Home PageDocument6 pagesGrand Rounds Index UTMB Otolaryngology Home PageWiwie Dwi FitriNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument21 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherStefana NanuNo ratings yet
- Fascial Space InfectionsDocument15 pagesFascial Space Infectionsali tiwanaNo ratings yet
- 9 Odontogenic Infections and Pyogenic Infections of The Soft TissuesDocument9 pages9 Odontogenic Infections and Pyogenic Infections of The Soft Tissuesاحمد سلامNo ratings yet
- Odontogenic Infections: Ickman Setoaji W, DRG., MMDocument66 pagesOdontogenic Infections: Ickman Setoaji W, DRG., MMAmeliza Putri AlindNo ratings yet
- Space Infections ClassificationDocument3 pagesSpace Infections ClassificationRameesa MithilajNo ratings yet
- OMFS Mandibular Space InfectionDocument27 pagesOMFS Mandibular Space InfectionsoorajNo ratings yet
- Deep Neck Infections: ProblemDocument14 pagesDeep Neck Infections: ProblemAmy KochNo ratings yet
- Space InfectionsDocument79 pagesSpace Infectionssridevi sivaramakrishnanNo ratings yet
- 3,2 - Spread of InflamationDocument14 pages3,2 - Spread of Inflamationحمزة تلاحمةNo ratings yet
- Bagaimana Menangani Infeksi OdontogenikDocument37 pagesBagaimana Menangani Infeksi OdontogenikTiara IkaNo ratings yet
- Fascialspaceinfections 140219122023 Phpapp01Document58 pagesFascialspaceinfections 140219122023 Phpapp01muhamed sayedNo ratings yet
- Management of The Infections of The Masticatory Spaces Gathered by Mohammed AlhayaniDocument10 pagesManagement of The Infections of The Masticatory Spaces Gathered by Mohammed Alhayaniمحمد عامر حكمت جبيرNo ratings yet
- Deep Space Neck (EDocFind - Com)Document100 pagesDeep Space Neck (EDocFind - Com)boomb162006No ratings yet
- Mycology For DentistryDocument35 pagesMycology For DentistryErizka RivaniNo ratings yet
- PBL - Fascial Space - SubmandibularDocument10 pagesPBL - Fascial Space - SubmandibularAlbert LawNo ratings yet
- Jcedv 10 I 5 P 495Document4 pagesJcedv 10 I 5 P 495Yohana SimanjuntakNo ratings yet
- Principles of Management and Prevention of Odontogenic InfectionsDocument167 pagesPrinciples of Management and Prevention of Odontogenic InfectionsNur IbrahimNo ratings yet
- Deep Neck Space InfectionsDocument43 pagesDeep Neck Space InfectionsmariscaclaudiaaNo ratings yet
- TBR Odontogenic InfectionsDocument34 pagesTBR Odontogenic InfectionsGiePramaNo ratings yet
- Surgery - Orofacial InfectionsDocument11 pagesSurgery - Orofacial InfectionsBatool HusseinNo ratings yet
- Spread of InflamationDocument14 pagesSpread of InflamationShadeeBreijiehNo ratings yet
- 4 Profound Phlegmon Maxillofacial AreaDocument21 pages4 Profound Phlegmon Maxillofacial AreaАлександр ВолошанNo ratings yet
- Odontogenic Infections Of Upper Jaw: حلا ــف دمحم ةـشـئاع Group: C2Document24 pagesOdontogenic Infections Of Upper Jaw: حلا ــف دمحم ةـشـئاع Group: C2Hayder HussienNo ratings yet
- Abcesele Spațiilor SuperficialeDocument60 pagesAbcesele Spațiilor SuperficialeSalameh Abu MUSSANo ratings yet
- Ludwig AnginaDocument6 pagesLudwig AnginarichardananNo ratings yet
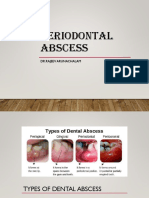
- Periodontal Abscess: DR - Rajeev ArunachalamDocument44 pagesPeriodontal Abscess: DR - Rajeev Arunachalamdamien teeNo ratings yet
- Hemangioma and Vascular MalformationDocument62 pagesHemangioma and Vascular MalformationMugdha FrancisNo ratings yet
- Management of ImpactionsDocument58 pagesManagement of ImpactionsMugdha FrancisNo ratings yet
- Immediate Loading Implants - Treatment Planning To Recent AdvancesDocument168 pagesImmediate Loading Implants - Treatment Planning To Recent AdvancesMugdha FrancisNo ratings yet
- Complications of Orthognathic SurgeryDocument75 pagesComplications of Orthognathic SurgeryMugdha FrancisNo ratings yet
- Zygomatic Bone FractureDocument77 pagesZygomatic Bone FractureMugdha FrancisNo ratings yet
- Salivary Gland TumorsDocument68 pagesSalivary Gland TumorsMugdha FrancisNo ratings yet
- Prof .B. Srinivasan. B.SC, MDSDocument128 pagesProf .B. Srinivasan. B.SC, MDSMugdha FrancisNo ratings yet
- Churchill PocketbookDocument30 pagesChurchill PocketbookMugdha Francis100% (1)
- TMJ AnkylosisDocument42 pagesTMJ AnkylosisMugdha FrancisNo ratings yet
- Approaches To The Facial SkeletonDocument117 pagesApproaches To The Facial SkeletonMugdha FrancisNo ratings yet
- Bone Grafts For Maxillofacial ReconstructionDocument77 pagesBone Grafts For Maxillofacial ReconstructionMugdha FrancisNo ratings yet
- Atlas of Oculoplastic and Orbital SurgeryDocument338 pagesAtlas of Oculoplastic and Orbital Surgeryxakos16766No ratings yet
- Rehab After OsteotomyDocument2 pagesRehab After OsteotomyMiguel OrdoñezNo ratings yet
- Vasculopatia LivedoidaDocument4 pagesVasculopatia LivedoidaJasNo ratings yet
- Emnc 4 North Drug StudyDocument12 pagesEmnc 4 North Drug StudyFrancesca Aurea MagumunNo ratings yet
- VT Guidelines PDFDocument74 pagesVT Guidelines PDFgabrimarteNo ratings yet
- Avoid Blood Clots in LegsDocument10 pagesAvoid Blood Clots in Legslewako4040No ratings yet
- 111Document80 pages111Amrut HosmaniNo ratings yet
- Coronary CirculationDocument47 pagesCoronary CirculationSuresh KumarNo ratings yet
- Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewDocument13 pagesPathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewBryan Diaz LopezNo ratings yet
- SNC Module 1 - Medical Background 0Document42 pagesSNC Module 1 - Medical Background 0shadi alshadafanNo ratings yet
- Management of Patients With Vascular Disorders: Venous ArterialDocument56 pagesManagement of Patients With Vascular Disorders: Venous ArterialHamss AhmedNo ratings yet
- Extrahepatic Portal Venous Obstruction PDFDocument2 pagesExtrahepatic Portal Venous Obstruction PDFSusanNo ratings yet
- EltrombopagDocument10 pagesEltrombopagkhangsiean89No ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisGladys YaresNo ratings yet
- Cerebral AneurysmDocument69 pagesCerebral AneurysmDiksha chaudharyNo ratings yet
- Strongyles Journal ArticleDocument4 pagesStrongyles Journal ArticleSam FanelliNo ratings yet
- Drugs For Circulatory DisordersDocument32 pagesDrugs For Circulatory Disordersnk999999No ratings yet
- Bipolar Disorders - 2023 - Ponzer - Lithium and Risk of Cardiovascular Disease Dementia and Venous ThromboembolismDocument11 pagesBipolar Disorders - 2023 - Ponzer - Lithium and Risk of Cardiovascular Disease Dementia and Venous ThromboembolismKonstantinos RantisNo ratings yet
- Immediate Care in PostnatalDocument12 pagesImmediate Care in Postnatalvarshasharma05No ratings yet
- Thromboembolic DisordersDocument6 pagesThromboembolic DisordersadiNo ratings yet
- ESC Diagnosis and Management of Acute Deep Vein ThrombosisDocument14 pagesESC Diagnosis and Management of Acute Deep Vein ThrombosisNat DabuétNo ratings yet
- Epidemiology y Historia Natural TVPDocument14 pagesEpidemiology y Historia Natural TVPVirginia WongNo ratings yet
- The Commonest Causes of Anoxic Necrosis 11 September 2023Document66 pagesThe Commonest Causes of Anoxic Necrosis 11 September 2023Ardian AshadiNo ratings yet
- Neuroform 3Document4 pagesNeuroform 3neureportNo ratings yet
- Endothelium in Thrombosis JournalDocument6 pagesEndothelium in Thrombosis JournalRahmi NisaNo ratings yet
- Venous Disorders: DefinationDocument41 pagesVenous Disorders: DefinationRahul SinghNo ratings yet
- Disease That Related To Physiotherapy in Travel MedicineDocument2 pagesDisease That Related To Physiotherapy in Travel MedicineBambang Ulan AeiyuNo ratings yet