Download as pdf or txt
You might also like
- Anatomic Exposure in Vascular Surgery, 3E (2013) (PDF) (UnitedVRG)Document605 pagesAnatomic Exposure in Vascular Surgery, 3E (2013) (PDF) (UnitedVRG)Rafael Castillo85% (13)
- Fetal Echocardiography Reporting FormatDocument1 pageFetal Echocardiography Reporting FormatMulugeta Abeneh100% (1)
- Cardiology Krok 2Document14 pagesCardiology Krok 2Suha AbdullahNo ratings yet
- Sabiston Textbook of Surgery 17th Ed 2005Document2,477 pagesSabiston Textbook of Surgery 17th Ed 2005Kyo Kusanagy38% (13)
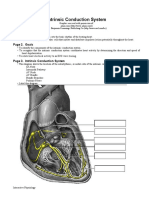
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- Estoya, Gen Paulo C. - Deep Vein Thrombosis NCP - NCM 112 LecDocument2 pagesEstoya, Gen Paulo C. - Deep Vein Thrombosis NCP - NCM 112 LecGen Paulo EstoyaNo ratings yet
- Cerebrovascular Disease MCQDocument25 pagesCerebrovascular Disease MCQDr. Kishore Kumar Ubrangala85% (13)
- 37 1Document3 pages37 1MoneymakerNo ratings yet
- Vascular and Peritoneal AccessDocument91 pagesVascular and Peritoneal AccessFrida AtallahNo ratings yet
- Vascular Access For Dialytic Therapies: Jan H. M. TordoirDocument1 pageVascular Access For Dialytic Therapies: Jan H. M. TordoirYuliastuti Mamah ChelseaNo ratings yet
- Eriko Shibata, Kojiro Nagai, Risa Takeuchi, (2015)Document3 pagesEriko Shibata, Kojiro Nagai, Risa Takeuchi, (2015)Aufa AdliaNo ratings yet
- Jeac 239Document4 pagesJeac 239Spam MailerNo ratings yet
- (CVP Journal) Vallo, Josef Dale T.Document2 pages(CVP Journal) Vallo, Josef Dale T.Josef ValloNo ratings yet
- Portal Hypertension SurgeryDocument6 pagesPortal Hypertension SurgeryjackSNMMCNo ratings yet
- Dialysis Access and Recirculation: Toros Kapoian Jeffrey L. Kaufman John Nosher Richard A. ShermanDocument14 pagesDialysis Access and Recirculation: Toros Kapoian Jeffrey L. Kaufman John Nosher Richard A. ShermanaeleandrosNo ratings yet
- Fistula USGDocument20 pagesFistula USGsamuelNo ratings yet
- AVF NewDocument81 pagesAVF NewBasit AliNo ratings yet
- Overview of Hemodialysis Access and Assessment - PMCDocument17 pagesOverview of Hemodialysis Access and Assessment - PMCvwyldrNo ratings yet
- Dr. Farsana - TK Junior ResidentDocument30 pagesDr. Farsana - TK Junior ResidentKmct Radiology Dpt.No ratings yet
- Arterial LineDocument2 pagesArterial LineRaghav Goyal100% (1)
- Aneurysm Abdominal AortaDocument8 pagesAneurysm Abdominal AortaMochammad Halim NNo ratings yet
- Original ArticlesDocument8 pagesOriginal ArticlesHugoNo ratings yet
- A Review Article: Access Recirculation Among End Stage Renal Disease Pa-Tients Undergoing Maintenance HemodialysisDocument6 pagesA Review Article: Access Recirculation Among End Stage Renal Disease Pa-Tients Undergoing Maintenance HemodialysisIrma HermaliaNo ratings yet
- Conduits For Coronary Bypass: Vein Grafts: Hendrick B Barner, M.D., Emily A Farkas, M.DDocument12 pagesConduits For Coronary Bypass: Vein Grafts: Hendrick B Barner, M.D., Emily A Farkas, M.DGaetano Di GiovanniNo ratings yet
- HarrisDocument25 pagesHarrisHafiz AlfarizieNo ratings yet
- ImpellaDocument5 pagesImpellapuspaNo ratings yet
- Tumor Kanker TiroidDocument9 pagesTumor Kanker TiroidyuliantoNo ratings yet
- Prospective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsDocument5 pagesProspective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsIvor WilopoNo ratings yet
- Manajemen Transfusi Perioperatif Pada Pasien Bedah Jantung Dewasa DenganDocument18 pagesManajemen Transfusi Perioperatif Pada Pasien Bedah Jantung Dewasa DenganGambar DoangNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- Malgor 2013Document4 pagesMalgor 2013vas25No ratings yet
- Management Acute Variceal BleedingDocument7 pagesManagement Acute Variceal BleedingSilminaNo ratings yet
- Cateteres Arteriaes, Central y Arteria PulmonarDocument13 pagesCateteres Arteriaes, Central y Arteria PulmonarmmsNo ratings yet
- Carotid PSV Song YDocument6 pagesCarotid PSV Song YthunderparthNo ratings yet
- Cardiac Complications of Arteriovenous Fistulas in Patients With End-Stage Renal DiseaseDocument12 pagesCardiac Complications of Arteriovenous Fistulas in Patients With End-Stage Renal Diseasetenty isniNo ratings yet
- JUMDC 6 Arterio VenousDocument6 pagesJUMDC 6 Arterio VenousMudassar SaeedNo ratings yet
- Flow Ands Cardiac ComplicationsDocument4 pagesFlow Ands Cardiac ComplicationsRenov OmpusungguNo ratings yet
- Ateriovenous FistulaDocument31 pagesAteriovenous Fistulaapi-265849428No ratings yet
- Potri Hafisah B. Macadaya Group 2 BSN 3Document26 pagesPotri Hafisah B. Macadaya Group 2 BSN 3Marivic Diano100% (2)
- Vascular Access HemodialysisDocument19 pagesVascular Access Hemodialysisplethoraldork100% (1)
- Endoscopicmanagementof Portalhypertension-Related Bleeding: Andrew Nett,, Kenneth F. BinmoellerDocument17 pagesEndoscopicmanagementof Portalhypertension-Related Bleeding: Andrew Nett,, Kenneth F. BinmoellerAlonso CayaniNo ratings yet
- Emborrhoid Technique Performed On A Patient With Portal Hypertension and Chronic Hemorrhoidal Bleeding As A Salvage TherapyDocument4 pagesEmborrhoid Technique Performed On A Patient With Portal Hypertension and Chronic Hemorrhoidal Bleeding As A Salvage TherapydianisaindiraNo ratings yet
- Fluid Management in Acute Kidney InjuryDocument8 pagesFluid Management in Acute Kidney InjuryHGZ 83 MoreliaNo ratings yet
- Assessment of Av FistulaDocument49 pagesAssessment of Av Fistulaatul_desai_3100% (1)
- Vascular Access For HemodialysisDocument25 pagesVascular Access For HemodialysisKartika JuwitaNo ratings yet
- Adenosine-Induced Transient Asystole: Gavin W. Britz, M.D., M.P.HDocument4 pagesAdenosine-Induced Transient Asystole: Gavin W. Britz, M.D., M.P.HAnkitaNo ratings yet
- What Is FFR?: How Can FFR Affect Treatment of The Patient?Document3 pagesWhat Is FFR?: How Can FFR Affect Treatment of The Patient?Anonymous 2wt1RiNo ratings yet
- 2016 - Mukhtar - Modulation of Splanchnic CirculationDocument12 pages2016 - Mukhtar - Modulation of Splanchnic CirculationJZNo ratings yet
- AAAkateDocument5 pagesAAAkateprem kotiNo ratings yet
- Arterial DopplerDocument29 pagesArterial DopplerAudrey100% (20)
- Phlebology 2012 Gloviczki 2 9Document9 pagesPhlebology 2012 Gloviczki 2 9Peet UpNo ratings yet
- I1524-5012-16-3-243 IMPELLADocument7 pagesI1524-5012-16-3-243 IMPELLAzairakuri32No ratings yet
- Robertson 2017Document10 pagesRobertson 2017tnsourceNo ratings yet
- CVP Evaluation Interpretation PDFDocument3 pagesCVP Evaluation Interpretation PDFMegan LewisNo ratings yet
- The Role of Color Doppler Ultrasound in Living Donor Liver Transplantation 2008 Journal of Medical UltrasoundDocument11 pagesThe Role of Color Doppler Ultrasound in Living Donor Liver Transplantation 2008 Journal of Medical UltrasoundIman Ru-ancaNo ratings yet
- Doppler-Atlas VasospasmDocument5 pagesDoppler-Atlas VasospasmdanielNo ratings yet
- mn58 Pleno Dialysis UnumaDocument2 pagesmn58 Pleno Dialysis UnumaBashir AhmedNo ratings yet
- Arteriovenous FistulasDocument21 pagesArteriovenous FistulasDragos GarofilNo ratings yet
- Venous Congestion ChapterDocument8 pagesVenous Congestion ChapterpcarrascoeNo ratings yet
- Blalock Taussig Shunt PDFDocument4 pagesBlalock Taussig Shunt PDFzuraini_mdnoorNo ratings yet
- Brain HemorrhagesDocument9 pagesBrain HemorrhagesAyashopia AyaNo ratings yet
- VExUS Nexus Bedside Assessment of Venous CongestiDocument10 pagesVExUS Nexus Bedside Assessment of Venous Congestilegap27No ratings yet
- AvfrdingDocument4 pagesAvfrdingyelisha05No ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Diagnostic and Interventional Radiology of Arteriovenous Accesses for HemodialysisFrom EverandDiagnostic and Interventional Radiology of Arteriovenous Accesses for HemodialysisNo ratings yet
- T3 - Pack Code DetailsDocument302 pagesT3 - Pack Code DetailskiranNo ratings yet
- Atrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhDocument60 pagesAtrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
- Anatomy of The Ventricular Septal Defect in Congenital Heart DefectDocument8 pagesAnatomy of The Ventricular Septal Defect in Congenital Heart DefectFajar YuniftiadiNo ratings yet
- CVS Tables FranzDocument7 pagesCVS Tables FranzCole GoNo ratings yet
- Matsushita 2010Document7 pagesMatsushita 2010Arankesh MNo ratings yet
- THROMBOSISDocument11 pagesTHROMBOSISChandan DebbarmaNo ratings yet
- Basic Coronary Angiography All SlidesDocument55 pagesBasic Coronary Angiography All SlidesSaud ShirwanNo ratings yet
- Waksman 2018Document7 pagesWaksman 2018harry pribadiNo ratings yet
- Moya MoyaDocument5 pagesMoya MoyaNick Junior100% (1)
- Do Any Supplements Help For Varicose Veins or Chronic Venous Insufficiency?Document2 pagesDo Any Supplements Help For Varicose Veins or Chronic Venous Insufficiency?PeterNo ratings yet
- Cardiovascular Pathology 1:: Blood VesselsDocument48 pagesCardiovascular Pathology 1:: Blood VesselsRaiver CadenNo ratings yet
- Blood CirculationDocument42 pagesBlood CirculationAshu kumar100% (1)
- Tissues and Intro To Circulation 2014 2Document51 pagesTissues and Intro To Circulation 2014 2Chantae JulienNo ratings yet
- Basic EcmoDocument62 pagesBasic EcmoBasantkumar SinghNo ratings yet
- Biochemical Markers For Clinical Monitoring of Tissue PerfusionDocument14 pagesBiochemical Markers For Clinical Monitoring of Tissue PerfusionTrọng MPNo ratings yet
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanNo ratings yet
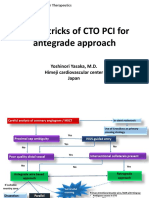
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 pagesTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNo ratings yet
- Tim Gilbert and Nicola Rudge Chief of Medicine 1 Service and Chief PharmacistDocument39 pagesTim Gilbert and Nicola Rudge Chief of Medicine 1 Service and Chief PharmacistjellyjohnNo ratings yet
- Congestive Heart FailureDocument1 pageCongestive Heart Failuredr_654737902No ratings yet
- Measurement of CENTRAL VENOUS PRESSURE Via A TransducerDocument22 pagesMeasurement of CENTRAL VENOUS PRESSURE Via A TransducerJasleen KaurNo ratings yet
- A Simple and Fast Experimental Model: Laboratory InvestigationDocument4 pagesA Simple and Fast Experimental Model: Laboratory InvestigationAjay PeddiNo ratings yet
- Management of Acute Limb Ischemia in The Pediatric PopulationDocument5 pagesManagement of Acute Limb Ischemia in The Pediatric PopulationPendidikan Dokter Unsyiah 2015No ratings yet
- DobutaminDocument15 pagesDobutaminInnocence AmandaNo ratings yet