
Prevalence and Prognostic Relevance of Invasive Fungal Disease During Veno-Arterial ECMO - A Retrospective Single-Center Study
Prevalence and Prognostic Relevance of Invasive Fungal Disease During Veno-Arterial ECMO - A Retrospective Single-Center Study
You might also like
- ASTM 6365 - 99 - Spark TestDocument4 pagesASTM 6365 - 99 - Spark Testjudith_ayala_10No ratings yet
- OM Stafilococo (Clase Observacionales)Document7 pagesOM Stafilococo (Clase Observacionales)Jairo Camilo Guevara FaríasNo ratings yet
- Ioi80197 463 473Document11 pagesIoi80197 463 473Phạm LinhNo ratings yet
- Fernando Et Al 2023 ICMDocument11 pagesFernando Et Al 2023 ICMpaul00040No ratings yet
- Predictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary TumorsDocument6 pagesPredictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary Tumorsfabian arassiNo ratings yet
- Systemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyDocument37 pagesSystemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyJuliana SanjayaNo ratings yet
- Ektub 1Document7 pagesEktub 1Muhamad ArwaniNo ratings yet
- Saving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportDocument11 pagesSaving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportSara MendesNo ratings yet
- Pola 2017Document10 pagesPola 2017RobertoNo ratings yet
- Allou 2018Document7 pagesAllou 2018jq4rhbh2pzNo ratings yet
- 20 - 3016 Faraz MansoorDocument5 pages20 - 3016 Faraz MansoorAwais ChatthaNo ratings yet
- Central Nervous System Infection Following Allogeneic Hematopoietic Stem Cell TransplantationDocument7 pagesCentral Nervous System Infection Following Allogeneic Hematopoietic Stem Cell Transplantationadilla kusumaNo ratings yet
- 2020 Covid 19 ECMO and LymphopeniaDocument1 page2020 Covid 19 ECMO and LymphopeniaDidier AdodoNo ratings yet
- Gordana Pavliša, Marina Labor, Hrvoje Puretić, Ana Hećimović, Marko Jakopović, Miroslav SamaržijaDocument12 pagesGordana Pavliša, Marina Labor, Hrvoje Puretić, Ana Hećimović, Marko Jakopović, Miroslav SamaržijaAngelo GarinoNo ratings yet
- 4 PBDocument6 pages4 PBarfikNo ratings yet
- Decreasing External Ventricular Drain Infection Rates in The Neurocritical Care Unit: 12-Year Longitudinal Experience at A Single InstitutionDocument13 pagesDecreasing External Ventricular Drain Infection Rates in The Neurocritical Care Unit: 12-Year Longitudinal Experience at A Single Institutionkhaled msalbiNo ratings yet
- CC 12570Document9 pagesCC 12570Kornelis AribowoNo ratings yet
- Ivcf SrmaDocument20 pagesIvcf SrmaabdulazizalsharydahNo ratings yet
- Clinical Microbiology and Infection: Research NoteDocument4 pagesClinical Microbiology and Infection: Research NoteNoorNo ratings yet
- Gopalakrishnan 2020Document8 pagesGopalakrishnan 2020jq4rhbh2pzNo ratings yet
- Duygu 2020Document4 pagesDuygu 2020Aditya HendraNo ratings yet
- Ebrahim 2021Document8 pagesEbrahim 2021wiyay34652ceoshubcomNo ratings yet
- PIIS0022510X20304998Document7 pagesPIIS0022510X20304998dhea handyaraNo ratings yet
- Complication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011Document6 pagesComplication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011JT DanielsNo ratings yet
- Teori Eosinopenia DewasaDocument7 pagesTeori Eosinopenia DewasaNurlyanti RustamNo ratings yet
- Antifungal Treatment Duration in Hematology Patients With Invasive Mold Infections A Real-Life UpdateDocument9 pagesAntifungal Treatment Duration in Hematology Patients With Invasive Mold Infections A Real-Life UpdateNelly Mabel Quiroz HernandezNo ratings yet
- Outcome and Clinical Characteristics of Nosocomial Infection in Adult Patients Undergoing Extracorporeal Membrane OxygenationDocument11 pagesOutcome and Clinical Characteristics of Nosocomial Infection in Adult Patients Undergoing Extracorporeal Membrane OxygenationGilberto Díaz PérezNo ratings yet
- Taccone2015 Article EpidemiologyOfInvasiveAspergilDocument15 pagesTaccone2015 Article EpidemiologyOfInvasiveAspergilsafaridikaNo ratings yet
- (RCT) Cardiovascular Injuries After Covid-19 InfectionDocument7 pages(RCT) Cardiovascular Injuries After Covid-19 InfectionPatrick NunsioNo ratings yet
- Endocardita InfectioasaDocument8 pagesEndocardita InfectioasaFlavia CarpNo ratings yet
- Meta 4Document4 pagesMeta 4Jonathan AiresNo ratings yet
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- Incidence, Outcome and Risk Factors For Sepsis - A Two Year Retrospective Study at Surgical ICU of A Tertiary Hospital in Pakistan.Document6 pagesIncidence, Outcome and Risk Factors For Sepsis - A Two Year Retrospective Study at Surgical ICU of A Tertiary Hospital in Pakistan.faraz.mirza1No ratings yet
- s41598 023 27465 yDocument9 pagess41598 023 27465 yMarcela MahechaNo ratings yet
- Lander 2016Document2 pagesLander 2016Jocilene Dantas Torres NascimentoNo ratings yet
- December 2020 - Volume 7 - Article 614569Document11 pagesDecember 2020 - Volume 7 - Article 614569elza pratiwiNo ratings yet
- Wu Et Al 2017 - Epidemiology and Risk Factors of Infective Endocarditis in Children in ChinaDocument10 pagesWu Et Al 2017 - Epidemiology and Risk Factors of Infective Endocarditis in Children in ChinaOktadoni SaputraNo ratings yet
- LiquorDocument8 pagesLiquorFanel PutraNo ratings yet
- Acute Kidney Injury Following Multisystem Infammatory Syndrome Associated With SARS CoV 2 Infection in ChildrenDocument14 pagesAcute Kidney Injury Following Multisystem Infammatory Syndrome Associated With SARS CoV 2 Infection in ChildrenBlack ManNo ratings yet
- 1 s2.0 S0022480422008150 MainDocument11 pages1 s2.0 S0022480422008150 MainYodi SoebadiNo ratings yet
- Ournal of Linical Ncology: PurposeDocument11 pagesOurnal of Linical Ncology: PurposeRicky Cornelius TariganNo ratings yet
- Art 3A10.1186 2Fcc3188Document174 pagesArt 3A10.1186 2Fcc3188mfhfhfNo ratings yet
- Invasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanDocument9 pagesInvasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanAngelin LigiantoNo ratings yet
- The Journal of Arthroplasty: Aaron J. Casp, MD, James A. Browne, MD, Nicole E. Durig, MD, MS, Brian C. Werner, MDDocument4 pagesThe Journal of Arthroplasty: Aaron J. Casp, MD, James A. Browne, MD, Nicole E. Durig, MD, MS, Brian C. Werner, MDLussy Tri OctavianiNo ratings yet
- Acute Kidney Injury and Risk of Death After.27 PDFDocument8 pagesAcute Kidney Injury and Risk of Death After.27 PDFtasya claudiaNo ratings yet
- Sharshar 2009 Debil y EstadiaDocument7 pagesSharshar 2009 Debil y EstadiaStefania Anahi MartelNo ratings yet
- A Propensity Score Matched Analysis of Open Versus Minimally Invasive Transthoracic Esophagectomy in The NetherlandsDocument8 pagesA Propensity Score Matched Analysis of Open Versus Minimally Invasive Transthoracic Esophagectomy in The NetherlandsLuca BellaioNo ratings yet
- Fungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrDocument18 pagesFungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrGiselle BaiãoNo ratings yet
- Perioperative Pulmonary Outcomes With OsaDocument9 pagesPerioperative Pulmonary Outcomes With OsawandapandabebeNo ratings yet
- PIIS2213260022005355Document16 pagesPIIS2213260022005355evelyn.minichNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptSyaiful ArifinNo ratings yet
- RVM y MedistinitisDocument5 pagesRVM y MedistinitisMartha CeciliaNo ratings yet
- 加拿大食道癌Document8 pages加拿大食道癌Joseph ChenNo ratings yet
- Chen 2015Document6 pagesChen 2015nurminsyahNo ratings yet
- Acute Pulmonary Embolism Associated With COVID-19 Pneumonia Detected With Pulmonary CT AngiographyDocument3 pagesAcute Pulmonary Embolism Associated With COVID-19 Pneumonia Detected With Pulmonary CT AngiographyAdriano OliveiraNo ratings yet
- Infected Post TEVARDocument12 pagesInfected Post TEVARYahya AlmalkiNo ratings yet
- Ofab 174Document4 pagesOfab 174MarioNo ratings yet
- Mortality Risk Assessment Using CHA 2 DS 2 VASc Scores - 2020 - The American JoDocument7 pagesMortality Risk Assessment Using CHA 2 DS 2 VASc Scores - 2020 - The American JoM. Haseeb ShahzadNo ratings yet
- Neutrophil To Lymphocyte Ratio and Periprosthetic Joint Infection A Systematic Review and Meta-AnalysisDocument8 pagesNeutrophil To Lymphocyte Ratio and Periprosthetic Joint Infection A Systematic Review and Meta-AnalysisJD2750No ratings yet
- 1 s2.0 S0163445320302085 Main PDFDocument7 pages1 s2.0 S0163445320302085 Main PDFJorgeNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Diversity of Wolbachia Infections in Sri Lankan Mosquitoes With A New Record of Wolbachia Supergroup B Infecting Aedes Aegypti Vector PopulationsDocument13 pagesDiversity of Wolbachia Infections in Sri Lankan Mosquitoes With A New Record of Wolbachia Supergroup B Infecting Aedes Aegypti Vector Populationsjd.jeffdahmerNo ratings yet
- International Journal of Food MicrobiologyDocument10 pagesInternational Journal of Food Microbiologyjd.jeffdahmerNo ratings yet
- Morphomolecular Characterization of Invasive Fruit Borer Infesting AppleDocument18 pagesMorphomolecular Characterization of Invasive Fruit Borer Infesting Applejd.jeffdahmerNo ratings yet
- Occurrence of Gastrointestinal Nematodes in Lambs in Norway, As Assessed by Copromicroscopy and Droplet Digital Polymerase Chain ReactionDocument11 pagesOccurrence of Gastrointestinal Nematodes in Lambs in Norway, As Assessed by Copromicroscopy and Droplet Digital Polymerase Chain Reactionjd.jeffdahmerNo ratings yet
- Tle CSS Mod5Document2 pagesTle CSS Mod5john kingNo ratings yet
- (U) Daily Activity Report: Marshall DistrictDocument5 pages(U) Daily Activity Report: Marshall DistrictFauquier NowNo ratings yet
- Chapter 7 - Morphing Skin Foams - 2018 - Morphing Wing TechnologiesDocument24 pagesChapter 7 - Morphing Skin Foams - 2018 - Morphing Wing TechnologiesRichardNo ratings yet
- Application FormDocument8 pagesApplication FormCrystal KleistNo ratings yet
- Pengaruh Konsentrasi Pupuk Bio Organik Terhadap PertumbuhanDocument14 pagesPengaruh Konsentrasi Pupuk Bio Organik Terhadap Pertumbuhansyariman sinjaiNo ratings yet
- Enfield Saheli: Funding NEWSDocument5 pagesEnfield Saheli: Funding NEWSenfieldclubhouseNo ratings yet
- LV Panel ReportDocument71 pagesLV Panel ReportMudassirNo ratings yet
- Nameplate PDFDocument8 pagesNameplate PDFobida adailehNo ratings yet
- SDM-v1 0Document32 pagesSDM-v1 0Franz NussmannNo ratings yet
- Copper (RJ-45) SFP: Technical SpecificationsDocument1 pageCopper (RJ-45) SFP: Technical SpecificationsDanielLopezNo ratings yet
- 10 Transport in Plants Neet Biology Model Question PaperDocument5 pages10 Transport in Plants Neet Biology Model Question PaperJosephNo ratings yet
- 2020 Proposal Online CarolingDocument2 pages2020 Proposal Online CarolingPel Vincent CruzNo ratings yet
- Epaper 20 October 2022Document22 pagesEpaper 20 October 2022Tauya DauramanziNo ratings yet
- Alm, Car BaselDocument4 pagesAlm, Car BaselAayush RawatNo ratings yet
- Tanguar Avijatrik - 2,3,4Document4 pagesTanguar Avijatrik - 2,3,4K. M. Ziauar RahmanNo ratings yet
- Clinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What IsDocument5 pagesClinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What Isarranguezjr5991No ratings yet
- D154-85 (2009) Standard Guide For Testing VarnishesDocument4 pagesD154-85 (2009) Standard Guide For Testing VarnishesRonny100% (1)
- P - Chapter 7Document17 pagesP - Chapter 7usa2017lapNo ratings yet
- Variable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitraDocument63 pagesVariable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitrabsbhavaniNo ratings yet
- Tecan Sunrise Absorbance Reader Analyser - User ManualDocument74 pagesTecan Sunrise Absorbance Reader Analyser - User Manualomer oartbNo ratings yet
- The Food Chain Consists of Four Main PartsDocument3 pagesThe Food Chain Consists of Four Main PartskoiaitraazNo ratings yet
- Nutri QuizDocument26 pagesNutri QuizChona Candace Christian AndalNo ratings yet
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- Septic Tank Leaching Chamber PDFDocument7 pagesSeptic Tank Leaching Chamber PDFJohan Shane CarsidoNo ratings yet
- DSFSDFSDF Advanced Construction TechnologiesDocument3 pagesDSFSDFSDF Advanced Construction Technologiessarveshfdk48No ratings yet
- IMRaD - Week 3 & 4Document8 pagesIMRaD - Week 3 & 4Ariana FiestaNo ratings yet
- Major Trauma Fellowship Senior Fellow Job Description: VisionDocument10 pagesMajor Trauma Fellowship Senior Fellow Job Description: VisionM LubisNo ratings yet
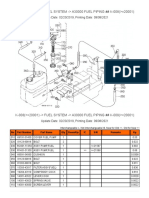
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- 7B ReportDocument12 pages7B ReportRowena A. TomalabcadNo ratings yet





























































































Download as pdf or txt
You might also like
- ASTM 6365 - 99 - Spark TestDocument4 pagesASTM 6365 - 99 - Spark Testjudith_ayala_10No ratings yet
- OM Stafilococo (Clase Observacionales)Document7 pagesOM Stafilococo (Clase Observacionales)Jairo Camilo Guevara FaríasNo ratings yet
- Ioi80197 463 473Document11 pagesIoi80197 463 473Phạm LinhNo ratings yet
- Fernando Et Al 2023 ICMDocument11 pagesFernando Et Al 2023 ICMpaul00040No ratings yet
- Predictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary TumorsDocument6 pagesPredictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary Tumorsfabian arassiNo ratings yet
- Systemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyDocument37 pagesSystemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyJuliana SanjayaNo ratings yet
- Ektub 1Document7 pagesEktub 1Muhamad ArwaniNo ratings yet
- Saving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportDocument11 pagesSaving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportSara MendesNo ratings yet
- Pola 2017Document10 pagesPola 2017RobertoNo ratings yet
- Allou 2018Document7 pagesAllou 2018jq4rhbh2pzNo ratings yet
- 20 - 3016 Faraz MansoorDocument5 pages20 - 3016 Faraz MansoorAwais ChatthaNo ratings yet
- Central Nervous System Infection Following Allogeneic Hematopoietic Stem Cell TransplantationDocument7 pagesCentral Nervous System Infection Following Allogeneic Hematopoietic Stem Cell Transplantationadilla kusumaNo ratings yet
- 2020 Covid 19 ECMO and LymphopeniaDocument1 page2020 Covid 19 ECMO and LymphopeniaDidier AdodoNo ratings yet
- Gordana Pavliša, Marina Labor, Hrvoje Puretić, Ana Hećimović, Marko Jakopović, Miroslav SamaržijaDocument12 pagesGordana Pavliša, Marina Labor, Hrvoje Puretić, Ana Hećimović, Marko Jakopović, Miroslav SamaržijaAngelo GarinoNo ratings yet
- 4 PBDocument6 pages4 PBarfikNo ratings yet
- Decreasing External Ventricular Drain Infection Rates in The Neurocritical Care Unit: 12-Year Longitudinal Experience at A Single InstitutionDocument13 pagesDecreasing External Ventricular Drain Infection Rates in The Neurocritical Care Unit: 12-Year Longitudinal Experience at A Single Institutionkhaled msalbiNo ratings yet
- CC 12570Document9 pagesCC 12570Kornelis AribowoNo ratings yet
- Ivcf SrmaDocument20 pagesIvcf SrmaabdulazizalsharydahNo ratings yet
- Clinical Microbiology and Infection: Research NoteDocument4 pagesClinical Microbiology and Infection: Research NoteNoorNo ratings yet
- Gopalakrishnan 2020Document8 pagesGopalakrishnan 2020jq4rhbh2pzNo ratings yet
- Duygu 2020Document4 pagesDuygu 2020Aditya HendraNo ratings yet
- Ebrahim 2021Document8 pagesEbrahim 2021wiyay34652ceoshubcomNo ratings yet
- PIIS0022510X20304998Document7 pagesPIIS0022510X20304998dhea handyaraNo ratings yet
- Complication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011Document6 pagesComplication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011JT DanielsNo ratings yet
- Teori Eosinopenia DewasaDocument7 pagesTeori Eosinopenia DewasaNurlyanti RustamNo ratings yet
- Antifungal Treatment Duration in Hematology Patients With Invasive Mold Infections A Real-Life UpdateDocument9 pagesAntifungal Treatment Duration in Hematology Patients With Invasive Mold Infections A Real-Life UpdateNelly Mabel Quiroz HernandezNo ratings yet
- Outcome and Clinical Characteristics of Nosocomial Infection in Adult Patients Undergoing Extracorporeal Membrane OxygenationDocument11 pagesOutcome and Clinical Characteristics of Nosocomial Infection in Adult Patients Undergoing Extracorporeal Membrane OxygenationGilberto Díaz PérezNo ratings yet
- Taccone2015 Article EpidemiologyOfInvasiveAspergilDocument15 pagesTaccone2015 Article EpidemiologyOfInvasiveAspergilsafaridikaNo ratings yet
- (RCT) Cardiovascular Injuries After Covid-19 InfectionDocument7 pages(RCT) Cardiovascular Injuries After Covid-19 InfectionPatrick NunsioNo ratings yet
- Endocardita InfectioasaDocument8 pagesEndocardita InfectioasaFlavia CarpNo ratings yet
- Meta 4Document4 pagesMeta 4Jonathan AiresNo ratings yet
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- Incidence, Outcome and Risk Factors For Sepsis - A Two Year Retrospective Study at Surgical ICU of A Tertiary Hospital in Pakistan.Document6 pagesIncidence, Outcome and Risk Factors For Sepsis - A Two Year Retrospective Study at Surgical ICU of A Tertiary Hospital in Pakistan.faraz.mirza1No ratings yet
- s41598 023 27465 yDocument9 pagess41598 023 27465 yMarcela MahechaNo ratings yet
- Lander 2016Document2 pagesLander 2016Jocilene Dantas Torres NascimentoNo ratings yet
- December 2020 - Volume 7 - Article 614569Document11 pagesDecember 2020 - Volume 7 - Article 614569elza pratiwiNo ratings yet
- Wu Et Al 2017 - Epidemiology and Risk Factors of Infective Endocarditis in Children in ChinaDocument10 pagesWu Et Al 2017 - Epidemiology and Risk Factors of Infective Endocarditis in Children in ChinaOktadoni SaputraNo ratings yet
- LiquorDocument8 pagesLiquorFanel PutraNo ratings yet
- Acute Kidney Injury Following Multisystem Infammatory Syndrome Associated With SARS CoV 2 Infection in ChildrenDocument14 pagesAcute Kidney Injury Following Multisystem Infammatory Syndrome Associated With SARS CoV 2 Infection in ChildrenBlack ManNo ratings yet
- 1 s2.0 S0022480422008150 MainDocument11 pages1 s2.0 S0022480422008150 MainYodi SoebadiNo ratings yet
- Ournal of Linical Ncology: PurposeDocument11 pagesOurnal of Linical Ncology: PurposeRicky Cornelius TariganNo ratings yet
- Art 3A10.1186 2Fcc3188Document174 pagesArt 3A10.1186 2Fcc3188mfhfhfNo ratings yet
- Invasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanDocument9 pagesInvasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanAngelin LigiantoNo ratings yet
- The Journal of Arthroplasty: Aaron J. Casp, MD, James A. Browne, MD, Nicole E. Durig, MD, MS, Brian C. Werner, MDDocument4 pagesThe Journal of Arthroplasty: Aaron J. Casp, MD, James A. Browne, MD, Nicole E. Durig, MD, MS, Brian C. Werner, MDLussy Tri OctavianiNo ratings yet
- Acute Kidney Injury and Risk of Death After.27 PDFDocument8 pagesAcute Kidney Injury and Risk of Death After.27 PDFtasya claudiaNo ratings yet
- Sharshar 2009 Debil y EstadiaDocument7 pagesSharshar 2009 Debil y EstadiaStefania Anahi MartelNo ratings yet
- A Propensity Score Matched Analysis of Open Versus Minimally Invasive Transthoracic Esophagectomy in The NetherlandsDocument8 pagesA Propensity Score Matched Analysis of Open Versus Minimally Invasive Transthoracic Esophagectomy in The NetherlandsLuca BellaioNo ratings yet
- Fungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrDocument18 pagesFungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrGiselle BaiãoNo ratings yet
- Perioperative Pulmonary Outcomes With OsaDocument9 pagesPerioperative Pulmonary Outcomes With OsawandapandabebeNo ratings yet
- PIIS2213260022005355Document16 pagesPIIS2213260022005355evelyn.minichNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptSyaiful ArifinNo ratings yet
- RVM y MedistinitisDocument5 pagesRVM y MedistinitisMartha CeciliaNo ratings yet
- 加拿大食道癌Document8 pages加拿大食道癌Joseph ChenNo ratings yet
- Chen 2015Document6 pagesChen 2015nurminsyahNo ratings yet
- Acute Pulmonary Embolism Associated With COVID-19 Pneumonia Detected With Pulmonary CT AngiographyDocument3 pagesAcute Pulmonary Embolism Associated With COVID-19 Pneumonia Detected With Pulmonary CT AngiographyAdriano OliveiraNo ratings yet
- Infected Post TEVARDocument12 pagesInfected Post TEVARYahya AlmalkiNo ratings yet
- Ofab 174Document4 pagesOfab 174MarioNo ratings yet
- Mortality Risk Assessment Using CHA 2 DS 2 VASc Scores - 2020 - The American JoDocument7 pagesMortality Risk Assessment Using CHA 2 DS 2 VASc Scores - 2020 - The American JoM. Haseeb ShahzadNo ratings yet
- Neutrophil To Lymphocyte Ratio and Periprosthetic Joint Infection A Systematic Review and Meta-AnalysisDocument8 pagesNeutrophil To Lymphocyte Ratio and Periprosthetic Joint Infection A Systematic Review and Meta-AnalysisJD2750No ratings yet
- 1 s2.0 S0163445320302085 Main PDFDocument7 pages1 s2.0 S0163445320302085 Main PDFJorgeNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Diversity of Wolbachia Infections in Sri Lankan Mosquitoes With A New Record of Wolbachia Supergroup B Infecting Aedes Aegypti Vector PopulationsDocument13 pagesDiversity of Wolbachia Infections in Sri Lankan Mosquitoes With A New Record of Wolbachia Supergroup B Infecting Aedes Aegypti Vector Populationsjd.jeffdahmerNo ratings yet
- International Journal of Food MicrobiologyDocument10 pagesInternational Journal of Food Microbiologyjd.jeffdahmerNo ratings yet
- Morphomolecular Characterization of Invasive Fruit Borer Infesting AppleDocument18 pagesMorphomolecular Characterization of Invasive Fruit Borer Infesting Applejd.jeffdahmerNo ratings yet
- Occurrence of Gastrointestinal Nematodes in Lambs in Norway, As Assessed by Copromicroscopy and Droplet Digital Polymerase Chain ReactionDocument11 pagesOccurrence of Gastrointestinal Nematodes in Lambs in Norway, As Assessed by Copromicroscopy and Droplet Digital Polymerase Chain Reactionjd.jeffdahmerNo ratings yet
- Tle CSS Mod5Document2 pagesTle CSS Mod5john kingNo ratings yet
- (U) Daily Activity Report: Marshall DistrictDocument5 pages(U) Daily Activity Report: Marshall DistrictFauquier NowNo ratings yet
- Chapter 7 - Morphing Skin Foams - 2018 - Morphing Wing TechnologiesDocument24 pagesChapter 7 - Morphing Skin Foams - 2018 - Morphing Wing TechnologiesRichardNo ratings yet
- Application FormDocument8 pagesApplication FormCrystal KleistNo ratings yet
- Pengaruh Konsentrasi Pupuk Bio Organik Terhadap PertumbuhanDocument14 pagesPengaruh Konsentrasi Pupuk Bio Organik Terhadap Pertumbuhansyariman sinjaiNo ratings yet
- Enfield Saheli: Funding NEWSDocument5 pagesEnfield Saheli: Funding NEWSenfieldclubhouseNo ratings yet
- LV Panel ReportDocument71 pagesLV Panel ReportMudassirNo ratings yet
- Nameplate PDFDocument8 pagesNameplate PDFobida adailehNo ratings yet
- SDM-v1 0Document32 pagesSDM-v1 0Franz NussmannNo ratings yet
- Copper (RJ-45) SFP: Technical SpecificationsDocument1 pageCopper (RJ-45) SFP: Technical SpecificationsDanielLopezNo ratings yet
- 10 Transport in Plants Neet Biology Model Question PaperDocument5 pages10 Transport in Plants Neet Biology Model Question PaperJosephNo ratings yet
- 2020 Proposal Online CarolingDocument2 pages2020 Proposal Online CarolingPel Vincent CruzNo ratings yet
- Epaper 20 October 2022Document22 pagesEpaper 20 October 2022Tauya DauramanziNo ratings yet
- Alm, Car BaselDocument4 pagesAlm, Car BaselAayush RawatNo ratings yet
- Tanguar Avijatrik - 2,3,4Document4 pagesTanguar Avijatrik - 2,3,4K. M. Ziauar RahmanNo ratings yet
- Clinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What IsDocument5 pagesClinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What Isarranguezjr5991No ratings yet
- D154-85 (2009) Standard Guide For Testing VarnishesDocument4 pagesD154-85 (2009) Standard Guide For Testing VarnishesRonny100% (1)
- P - Chapter 7Document17 pagesP - Chapter 7usa2017lapNo ratings yet
- Variable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitraDocument63 pagesVariable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitrabsbhavaniNo ratings yet
- Tecan Sunrise Absorbance Reader Analyser - User ManualDocument74 pagesTecan Sunrise Absorbance Reader Analyser - User Manualomer oartbNo ratings yet
- The Food Chain Consists of Four Main PartsDocument3 pagesThe Food Chain Consists of Four Main PartskoiaitraazNo ratings yet
- Nutri QuizDocument26 pagesNutri QuizChona Candace Christian AndalNo ratings yet
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- Septic Tank Leaching Chamber PDFDocument7 pagesSeptic Tank Leaching Chamber PDFJohan Shane CarsidoNo ratings yet
- DSFSDFSDF Advanced Construction TechnologiesDocument3 pagesDSFSDFSDF Advanced Construction Technologiessarveshfdk48No ratings yet
- IMRaD - Week 3 & 4Document8 pagesIMRaD - Week 3 & 4Ariana FiestaNo ratings yet
- Major Trauma Fellowship Senior Fellow Job Description: VisionDocument10 pagesMajor Trauma Fellowship Senior Fellow Job Description: VisionM LubisNo ratings yet
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- 7B ReportDocument12 pages7B ReportRowena A. TomalabcadNo ratings yet