Download as docx, pdf, or txt
You might also like
- Growth Genetics or AspirationDocument249 pagesGrowth Genetics or AspirationEdwin Ivan Yucra Quispe25% (4)
- External Frame Factors - Hand-OutsDocument5 pagesExternal Frame Factors - Hand-OutsNegros Occidental Houses100% (2)
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareFrom EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareNo ratings yet
- Abigail Harvey (Mcmahan) Galen College of Nursing BSN Program NSG 3100 Ms. Johnson March 25, 2021Document9 pagesAbigail Harvey (Mcmahan) Galen College of Nursing BSN Program NSG 3100 Ms. Johnson March 25, 2021api-581984607No ratings yet
- NURS - FPX 5005 - Brendan Madden - Assessment - 2-1Document9 pagesNURS - FPX 5005 - Brendan Madden - Assessment - 2-1SohaibNo ratings yet
- Quality of Nursing Care Practices Among Select Hospitals in Bataan EditedDocument23 pagesQuality of Nursing Care Practices Among Select Hospitals in Bataan EditedZonllam Aryl DialorNo ratings yet
- All India Hospital ListDocument42 pagesAll India Hospital ListSRINIVASARAO JONNALANo ratings yet
- Analysis of A Pertinent Healthcare IssueDocument6 pagesAnalysis of A Pertinent Healthcare Issuejossy MulingeNo ratings yet
- The Topic ofDocument3 pagesThe Topic ofaineyboneyNo ratings yet
- Chapter 1-2 Communication Skills Practiced in UB Nursing StudentsDocument7 pagesChapter 1-2 Communication Skills Practiced in UB Nursing StudentsSittie Haliza C. MacmodNo ratings yet
- Assignment ON Continuing EducationDocument6 pagesAssignment ON Continuing EducationDebashrita MisraNo ratings yet
- Hypo FPX 4020 Assessment 3Document14 pagesHypo FPX 4020 Assessment 3Sheela malhiNo ratings yet
- IdentidadDocument12 pagesIdentidadEdgarsito AyalaNo ratings yet
- Lived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationDocument20 pagesLived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationPsychology and Education: A Multidisciplinary JournalNo ratings yet
- 9796371Document19 pages9796371adri90No ratings yet
- Summary ResearchDocument6 pagesSummary ResearchLance SilvaNo ratings yet
- Increasing Identification of Domestic Violence in Emergency DepartmentsDocument42 pagesIncreasing Identification of Domestic Violence in Emergency Departmentselisha OwaisNo ratings yet
- Research PaperDocument8 pagesResearch PaperJunnel DavadNo ratings yet
- Perceived Level of Clinical Competence and Turnover Intention Among Newly Passed Nurses - Basis For A Retention ProgramDocument29 pagesPerceived Level of Clinical Competence and Turnover Intention Among Newly Passed Nurses - Basis For A Retention ProgramRey John BucadNo ratings yet
- Journal Summary For Surgery WardDocument1 pageJournal Summary For Surgery WardlordwinjohnbernardoNo ratings yet
- Jurnal IPE B1.1Document15 pagesJurnal IPE B1.1fikri syafiqNo ratings yet
- Notes Nurse PolicyDocument6 pagesNotes Nurse PolicyChristian HawthorneNo ratings yet
- Week 7 Discussion - Nursing LeadershipDocument6 pagesWeek 7 Discussion - Nursing LeadershipFranklin Mung'athia BettNo ratings yet
- Nurse To Nurse Communication 2Document7 pagesNurse To Nurse Communication 2api-314566363No ratings yet
- Van Patten 2019Document6 pagesVan Patten 2019Amrinder RandhawaNo ratings yet
- BSN 3a2 A - Chap 1 3Document32 pagesBSN 3a2 A - Chap 1 3Pollen Siega BunalNo ratings yet
- Nursing Report in BriefDocument4 pagesNursing Report in Briefgilbertangelus812No ratings yet
- Final Paper RheaDocument25 pagesFinal Paper RheaNeweeJoonYowNo ratings yet
- Present L6Document6 pagesPresent L6TONo ratings yet
- NONPF EditedDocument6 pagesNONPF EditedViotry ChepkwonyNo ratings yet
- Developing Professional Communication Skills in Nursing Students - Research Paper ExampleDocument3 pagesDeveloping Professional Communication Skills in Nursing Students - Research Paper Examplemtahir777945No ratings yet
- Impact of Social Media On Nurses Service Delivery - EditedDocument14 pagesImpact of Social Media On Nurses Service Delivery - EditedMaina PeterNo ratings yet
- Patient Safety A Literature Review To Inform An Evaluation of A Maternity ServiceDocument5 pagesPatient Safety A Literature Review To Inform An Evaluation of A Maternity ServicetdqmodcndNo ratings yet
- FPX4020 WilsonChelsea Assessment4 1Document17 pagesFPX4020 WilsonChelsea Assessment4 1FrancisNo ratings yet
- IntroductionDocument7 pagesIntroductionshadrack mutindaNo ratings yet
- File For Plagiarism Checking (Fizza)Document16 pagesFile For Plagiarism Checking (Fizza)Iqra AsimNo ratings yet
- A Thesis (Proposal) Presented To The Faculty of The College of Nursing Adamson UniversityDocument22 pagesA Thesis (Proposal) Presented To The Faculty of The College of Nursing Adamson UniversityRaidis PangilinanNo ratings yet
- Professional Meeting PaperDocument8 pagesProfessional Meeting Paperapi-739007989No ratings yet
- Changing Practice PowerpointDocument18 pagesChanging Practice PowerpointSarah BayouthNo ratings yet
- Professional Nursing Practice Impact On Organizational and Patient Outcomes FinDocument8 pagesProfessional Nursing Practice Impact On Organizational and Patient Outcomes FinGudyne WafubwaNo ratings yet
- Part A: PLAN (NURS 711) : Michelle StimsonDocument24 pagesPart A: PLAN (NURS 711) : Michelle Stimsonapi-270067627No ratings yet
- Qi Nursing Communication Final - Nurs 484Document12 pagesQi Nursing Communication Final - Nurs 484api-558100249No ratings yet
- Policy MakersDocument6 pagesPolicy MakersPoonam ThakurNo ratings yet
- 2019 LeapfrogToValue PDFDocument57 pages2019 LeapfrogToValue PDFJamey DAVIDSONNo ratings yet
- Patient Safety in Psychiatric Inpatient Care A Literature ReviewDocument12 pagesPatient Safety in Psychiatric Inpatient Care A Literature ReviewcigyofxgfNo ratings yet
- Researh ProblemsDocument7 pagesResearh ProblemsPrincess Arah AquinoNo ratings yet
- Trends and Issues in Nursing (CPD)Document13 pagesTrends and Issues in Nursing (CPD)Maizatul Akmar IbrahimNo ratings yet
- Evaluation of A Pregnancy Loss Education Intervention For Undergraduate Nursing Students in Northern Ireland: A Pre-And Post - Test StudyDocument10 pagesEvaluation of A Pregnancy Loss Education Intervention For Undergraduate Nursing Students in Northern Ireland: A Pre-And Post - Test Studyamelbos001No ratings yet
- Barriers of Advanced Practice NursingDocument5 pagesBarriers of Advanced Practice NursingBernardkimNo ratings yet
- Praktek Komunikasi Di Ruangan ANak Petecost Hospital MadinaDocument9 pagesPraktek Komunikasi Di Ruangan ANak Petecost Hospital Madinaatika indriyadiNo ratings yet
- Ethical Issues in Healthcare ManagementDocument44 pagesEthical Issues in Healthcare ManagementTravel with NiroNo ratings yet
- Assessment 2 Activity 1 Health PolicyDocument2 pagesAssessment 2 Activity 1 Health PolicyMahal PaetNo ratings yet
- Therapeutic Communication Through Simulation PDFDocument5 pagesTherapeutic Communication Through Simulation PDFNicole GadrinabNo ratings yet
- Charis Class 4050 Assmt 3.EditedDocument9 pagesCharis Class 4050 Assmt 3.EditedsirdeankenyaNo ratings yet
- Amanda Putri Z-SummarizingDocument4 pagesAmanda Putri Z-SummarizingAmanda putri ZuliantyNo ratings yet
- Course Outline NURS 4524 W 24Document19 pagesCourse Outline NURS 4524 W 24cydeykulgmzarinlhkNo ratings yet
- Primary Care Impact On Health Outcomes A Literature ReviewDocument6 pagesPrimary Care Impact On Health Outcomes A Literature Reviewm1dyhuh1jud2No ratings yet
- Future Direction of NursingDocument4 pagesFuture Direction of Nursingmerin sunil100% (1)
- Developing Organizational Policies and Practices ADocument7 pagesDeveloping Organizational Policies and Practices Amutisya johnboscoNo ratings yet
- Administration Assignment 2Document4 pagesAdministration Assignment 2wwwking341No ratings yet
- Reed - Reflection Paper Nurs631Document10 pagesReed - Reflection Paper Nurs631api-215994182No ratings yet
- Nurses Contributions to Quality Health OutcomesFrom EverandNurses Contributions to Quality Health OutcomesMarianne BaernholdtNo ratings yet
- Naac_Criteria-6_6.3.3.Professional Development Administrative Training Programmes Organized by the Institution for Teaching and Non- Teaching Staff During the Last Five Years_2.Reports,Attendance,Pics_4.Reports,Attendance,PicsDocument111 pagesNaac_Criteria-6_6.3.3.Professional Development Administrative Training Programmes Organized by the Institution for Teaching and Non- Teaching Staff During the Last Five Years_2.Reports,Attendance,Pics_4.Reports,Attendance,PicstechnewsNo ratings yet
- Product Catalog 2017: Home TherapiesDocument52 pagesProduct Catalog 2017: Home TherapiesAbidNo ratings yet
- Bitumen Burn Card - For Print PDFDocument2 pagesBitumen Burn Card - For Print PDFJelian GraceNo ratings yet
- Clear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewDocument4 pagesClear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Topic 1 What Is Patient Safety?: (Concepts and Prospects)Document21 pagesTopic 1 What Is Patient Safety?: (Concepts and Prospects)Reda ZizoNo ratings yet
- Drogueria SAN DIEGODocument8 pagesDrogueria SAN DIEGOJulieth CastiblancoNo ratings yet
- 15.boala Parkinson (Dana)Document48 pages15.boala Parkinson (Dana)Adriana AdrianaNo ratings yet
- Manual de Uso Videocolonoscopio Ec-530wlDocument60 pagesManual de Uso Videocolonoscopio Ec-530wlEddy Fernando Ruiz AvilaNo ratings yet
- List of Private Testing Labs in Kerala For Covid 19 As On October 22Document19 pagesList of Private Testing Labs in Kerala For Covid 19 As On October 22pushpanarayananNo ratings yet
- When You: The Nonviolent Requests GuideDocument1 pageWhen You: The Nonviolent Requests GuideFarukHosenRajNo ratings yet
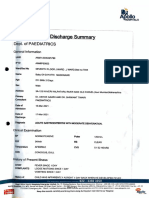
- Discharge Summary: Dept. of PaediatricsDocument3 pagesDischarge Summary: Dept. of PaediatricsGayatri MadkaikarNo ratings yet
- ITLS BROCHURE January 2021Document4 pagesITLS BROCHURE January 2021VickyMackanessNo ratings yet
- Poison GuideDocument31 pagesPoison GuideJarad KendrickNo ratings yet
- Resumen Unidad 2Document31 pagesResumen Unidad 2yeseniaram073No ratings yet
- Serht70 Rev.ADocument120 pagesSerht70 Rev.AFernando AlonsoNo ratings yet
- Kolkata HospitalDocument24 pagesKolkata HospitalKoushikKc ChatterjeeNo ratings yet
- Bridging The Gap: Understanding Medical Students' and Interns'perceptions of Radiology As A Career Choice at Taif University, Saudi ArabiaDocument8 pagesBridging The Gap: Understanding Medical Students' and Interns'perceptions of Radiology As A Career Choice at Taif University, Saudi ArabiaIJAR JOURNALNo ratings yet
- Atcn 2022Document10 pagesAtcn 2022Al RadyaNo ratings yet
- Linkages ITOCA - Facilitators GuideDocument54 pagesLinkages ITOCA - Facilitators GuideBonike MustaqiemNo ratings yet
- Acupuncture HistoryDocument3 pagesAcupuncture HistoryRahmah ThoyyibahNo ratings yet
- Effectivity of Vernonia Cinerea As An Anti-Microbial SalveDocument13 pagesEffectivity of Vernonia Cinerea As An Anti-Microbial SalveK8Y KattNo ratings yet
- 23. Đề thi thử TN THPT 2021 - Môn Tiếng anh - THPT Chuyên Trần Phú - Hải Phòng - Lần 1Document9 pages23. Đề thi thử TN THPT 2021 - Môn Tiếng anh - THPT Chuyên Trần Phú - Hải Phòng - Lần 1Linh CottonNo ratings yet
- PT Axelor Ultima Management 1Document72 pagesPT Axelor Ultima Management 1titin gusmayantuNo ratings yet
- Ecg - Partea I - Mircea CintezaDocument16 pagesEcg - Partea I - Mircea CintezaAndrei CiobotaruNo ratings yet
- Harare Dentist: Name Address Phone EmailDocument2 pagesHarare Dentist: Name Address Phone EmailTinotenda GambaraNo ratings yet
- Health Center and Catchment Area& Provision ofDocument2 pagesHealth Center and Catchment Area& Provision ofMuath HakeemNo ratings yet
- Update On COVID-19 Projections: Science Advisory and Modelling Consensus Tables September 28, 2021Document19 pagesUpdate On COVID-19 Projections: Science Advisory and Modelling Consensus Tables September 28, 2021Braydon WilliamsonNo ratings yet
- AVCN 2 Nhóm 2A 2Document25 pagesAVCN 2 Nhóm 2A 2FamiMeoNo ratings yet