Download as pdf or txt
You might also like
- Hosp BillDocument1 pageHosp BillFoxtrot Lima100% (1)
- Middle East Healthcare Directory Database Excel Format SampleDocument1 pageMiddle East Healthcare Directory Database Excel Format SampleKunal KhandelwalNo ratings yet
- Review Notes in Pharmacology - NCLEXDocument1 pageReview Notes in Pharmacology - NCLEXLalaine April E. Ortiola79% (29)
- Laboratory Sample Collection Form - Swine-5Document1 pageLaboratory Sample Collection Form - Swine-5Mary Grace LozadaNo ratings yet
- Heal and Balance Your Chakras With Reiki PDFDocument79 pagesHeal and Balance Your Chakras With Reiki PDFpalash100% (4)
- Final 1 - Mankind Pharma ReportDocument133 pagesFinal 1 - Mankind Pharma ReportMahabalaNo ratings yet
- 18-Qbase Anaesthesia Vol 4-Freemedicalbooks2014Document178 pages18-Qbase Anaesthesia Vol 4-Freemedicalbooks2014karan270100% (2)
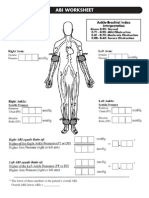
- Abi SheetsDocument2 pagesAbi Sheetszaky soewandi0% (1)
- Plugin-Mental Status ExamDocument32 pagesPlugin-Mental Status ExamSam100% (1)
- For Laboratory & Procedure Services: Letter of Authorization To ProviderDocument1 pageFor Laboratory & Procedure Services: Letter of Authorization To Providerlovely lantacaNo ratings yet
- Guerrero, Marietta IDocument1 pageGuerrero, Marietta I40-GALOLO ANDREA PAULINENo ratings yet
- Generate LOADocument1 pageGenerate LOAangel.domingo0309No ratings yet
- Generate LOADocument1 pageGenerate LOAdead9122No ratings yet
- De Lal Pathaabs: SM Bandana-DwvediDocument1 pageDe Lal Pathaabs: SM Bandana-DwvediSankalp RajputNo ratings yet
- Explanation of Benefits Medical: Jena Brown 8739 Moon Crater Ave LAS VEGAS, NV 89178-6535Document3 pagesExplanation of Benefits Medical: Jena Brown 8739 Moon Crater Ave LAS VEGAS, NV 89178-6535JenaNo ratings yet
- De Leon, Charmagne BDocument1 pageDe Leon, Charmagne BHasmin CortezNo ratings yet
- Report - 2023-03-23T141246.354Document3 pagesReport - 2023-03-23T141246.354G Anil KumarNo ratings yet
- Sudhir - 122980 - Dengue - Hospital SummaryDocument17 pagesSudhir - 122980 - Dengue - Hospital SummarySudhir PatelNo ratings yet
- Lab ReportDocument1 pageLab Reportnishitagupta750No ratings yet
- Generate LOADocument1 pageGenerate LOAalaizafrancisco94No ratings yet
- Revised Proforma Invoice-2443 Depil 500 TabDocument1 pageRevised Proforma Invoice-2443 Depil 500 TabNavi ThakurNo ratings yet
- Provisional Marksheet: INC - Incomplete Result UFM - Unfair MeansDocument1 pageProvisional Marksheet: INC - Incomplete Result UFM - Unfair MeansEdusoft AcademyNo ratings yet
- SettlementLetterHi 1706629011454Document2 pagesSettlementLetterHi 1706629011454mailing.intern1No ratings yet
- Jugao, TeresitaDocument1 pageJugao, Teresitamobai.li.yuNo ratings yet
- 8000100608762655-65083371-Form FDocument1 page8000100608762655-65083371-Form FSinar DuniaNo ratings yet
- SR User Access 2017 - New UserDocument5 pagesSR User Access 2017 - New Userclient napNo ratings yet
- Jeisys - Intracel - Edge One - Tribeam 206593-2016-CE-KOR-NADocument3 pagesJeisys - Intracel - Edge One - Tribeam 206593-2016-CE-KOR-NAFarid AbushovNo ratings yet
- Soa HospitalDocument1 pageSoa HospitalJocyl GonzagaNo ratings yet
- Revised Proforma Invoice-2443 Tant It TabDocument1 pageRevised Proforma Invoice-2443 Tant It TabNavi ThakurNo ratings yet
- Foreign Worker's Hospitalization & Surgical Scheme (FWHS) Policy ScheduleDocument3 pagesForeign Worker's Hospitalization & Surgical Scheme (FWHS) Policy ScheduleOng wkNo ratings yet
- Adobe Scan Jan 29, 2024Document1 pageAdobe Scan Jan 29, 2024mj digitalNo ratings yet
- 4010ip-03083292001 QTDocument4 pages4010ip-03083292001 QTMayank SharmaNo ratings yet
- Lippincott Illustrated Reviews - Pharmacology 7th EditionDocument1 pageLippincott Illustrated Reviews - Pharmacology 7th EditionRanjan MishraNo ratings yet
- GeM Bidding 4286394Document13 pagesGeM Bidding 4286394Hetal PatelNo ratings yet
- ContractDocument183 pagesContractTrúc NguyễnNo ratings yet
- Act02 Billing-BubanDocument1 pageAct02 Billing-BubanJennica BubanNo ratings yet
- Axa IDocument2 pagesAxa IalredhamuhamadNo ratings yet
- ST - Clare'S Medical Center, Inc.: 1838 Dian Street, Makati City, Metro ManilaDocument1 pageST - Clare'S Medical Center, Inc.: 1838 Dian Street, Makati City, Metro ManilaKristine TaguiamNo ratings yet
- Musamadya AUTHDocument2 pagesMusamadya AUTHLyn PedzaiNo ratings yet
- Relevant-Docs Infection Control MeasuresDocument85 pagesRelevant-Docs Infection Control MeasuresTatavarti AnandNo ratings yet
- V Trans India Limited - WC Quote - PDFDocument3 pagesV Trans India Limited - WC Quote - PDFVANAJAKSHI SNo ratings yet
- HCL Technologies LTD: Hospitalization Treatment Claim Summary FormDocument3 pagesHCL Technologies LTD: Hospitalization Treatment Claim Summary FormYeseswini0% (1)
- Outpatient Diagnostic & Procedure Form Letter of Guarantee (Log)Document1 pageOutpatient Diagnostic & Procedure Form Letter of Guarantee (Log)selinaberina18No ratings yet
- DCL Report - Hygitech HSDocument2 pagesDCL Report - Hygitech HSFarhan RashidNo ratings yet
- ZACHCHCHDocument1 pageZACHCHCHBay watchNo ratings yet
- Minimum Standard Requirements For 150 AdmissionsDocument3 pagesMinimum Standard Requirements For 150 Admissionsujjawal_46No ratings yet
- Personal Form For Professional IndemnityDocument1 pagePersonal Form For Professional IndemnityLilammani ChapagainNo ratings yet
- Backupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830Document2 pagesBackupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830MahanNo ratings yet
- Colour PrintDocument7 pagesColour PrintSubhadeep GhoshNo ratings yet
- Revised Medical Expense Statement - Oct 22Document3 pagesRevised Medical Expense Statement - Oct 22rita sarkarNo ratings yet
- Arcega Maria Lucia R. 3 15 24 RevisedDocument1 pageArcega Maria Lucia R. 3 15 24 RevisedMark BaniagaNo ratings yet
- Claim Settlement Letter 1688616797349Document6 pagesClaim Settlement Letter 1688616797349mailing.intern1No ratings yet
- Benefit 1Document10 pagesBenefit 1HL LauNo ratings yet
- We7e7061701 - Ge - Logiq® E9Document1 pageWe7e7061701 - Ge - Logiq® E9Younes ODMNo ratings yet
- Business Standard 27 Nov 18Document16 pagesBusiness Standard 27 Nov 18JintuboraNo ratings yet
- BD SalaryDocument1 pageBD Salaryabul skNo ratings yet
- Infinity Medical Systems: InvoiceDocument1 pageInfinity Medical Systems: InvoiceVijay AnandNo ratings yet
- Sabal Hospital Inc.: Summary of FeesDocument2 pagesSabal Hospital Inc.: Summary of FeesQuinio ReyNo ratings yet
- Occupational Medical Aptitude Certificate DE Entry ExamDocument28 pagesOccupational Medical Aptitude Certificate DE Entry ExamScribdTranslationsNo ratings yet
- Notice (8) : Patient Cash ReceiptDocument1 pageNotice (8) : Patient Cash ReceiptArjun Singh ChoudharyNo ratings yet
- Invoice - Ims048 GOVERNMENT MEDICAL COLLEGEDocument1 pageInvoice - Ims048 GOVERNMENT MEDICAL COLLEGEVijay AnandNo ratings yet
- Authorization LetterDocument8 pagesAuthorization Lettermanjusk0102No ratings yet
- Donald Court Warren, MI 48092-2793Document42 pagesDonald Court Warren, MI 48092-2793Nathan BlockNo ratings yet
- 22-07-77-17 (Tanveer Ahmed)Document2 pages22-07-77-17 (Tanveer Ahmed)Sohail RazaNo ratings yet
- Selecting Megavoltage Treatment Technologies in External Beam RadiotherapyFrom EverandSelecting Megavoltage Treatment Technologies in External Beam RadiotherapyNo ratings yet
- BEDINGDocument1 pageBEDINGMary Grace LozadaNo ratings yet
- Authority To Deduct From Wages Form - January 2015Document1 pageAuthority To Deduct From Wages Form - January 2015Mary Grace LozadaNo ratings yet
- Accomplishmentwk 37Document2 pagesAccomplishmentwk 37Mary Grace LozadaNo ratings yet
- Weekly Accomplishment ReportDocument1 pageWeekly Accomplishment ReportMary Grace LozadaNo ratings yet
- New RegistrationDocument3 pagesNew RegistrationMary Grace LozadaNo ratings yet
- Letter of Intent - RetirementDocument1 pageLetter of Intent - RetirementMary Grace LozadaNo ratings yet
- Accomplishmentwk 49Document2 pagesAccomplishmentwk 49Mary Grace LozadaNo ratings yet
- Accomplishmentwk 48Document3 pagesAccomplishmentwk 48Mary Grace LozadaNo ratings yet
- IHLABEXAM1Document2 pagesIHLABEXAM1Leigh ann BernaldezNo ratings yet
- Anuja StudyDocument2 pagesAnuja StudyAnuja MooneNo ratings yet
- PAGE 13-18: 1. Must 2. Must 3. Must Not 4. Must 5. Must Not Must NotDocument3 pagesPAGE 13-18: 1. Must 2. Must 3. Must Not 4. Must 5. Must Not Must NotNguyen Tran Anh Thu (FGW DN)No ratings yet
- Allison ResumeDocument2 pagesAllison Resumeapi-351570174No ratings yet
- UGT1A1 Allele Definition TableDocument7 pagesUGT1A1 Allele Definition TableElizaDiasNo ratings yet
- Giving Back To Gondwana Concert ProgramDocument24 pagesGiving Back To Gondwana Concert ProgramanguswoodsNo ratings yet
- Topic 2 - Adrenergic DrugsDocument52 pagesTopic 2 - Adrenergic DrugsAngeli Gregorio100% (1)
- Pharmacology of The Equine Foot Medical Pain Management For Laminitis 2021Document13 pagesPharmacology of The Equine Foot Medical Pain Management For Laminitis 2021guadialvarezNo ratings yet
- Odap NetherlandsDocument4 pagesOdap NetherlandsVarun ZotaNo ratings yet
- Complete Blood Count-2023-08-29t00 - 00 - 00Document2 pagesComplete Blood Count-2023-08-29t00 - 00 - 00Michamiel SerratoNo ratings yet
- Fellowship in Sports RehabilitationDocument6 pagesFellowship in Sports Rehabilitationsendilcoumarv83No ratings yet
- VSD Ventricular Septal Defect RepairDocument31 pagesVSD Ventricular Septal Defect RepairRedmond P. Burke MD100% (8)
- Self-Etching Bonding Agents: Clinical HintsDocument2 pagesSelf-Etching Bonding Agents: Clinical HintsJ SharaNo ratings yet
- CalibraDocument2 pagesCalibraDiaa Eldin SaadNo ratings yet
- Nursing Home ChargesDocument67 pagesNursing Home Chargesalmond2009No ratings yet
- Stability Is Key: Housing First For Individuals With SPMIDocument5 pagesStability Is Key: Housing First For Individuals With SPMIJack Id EstNo ratings yet
- SR Phonares II Tooth Mould ChartDocument8 pagesSR Phonares II Tooth Mould ChartSomnath SenguptaNo ratings yet
- Viral HepatitisDocument26 pagesViral HepatitisNasriah MacadatoNo ratings yet
- General PsychopathologyDocument35 pagesGeneral PsychopathologyMaria Ciorea100% (1)
- 1H 1,2,3 Triazoletethered Isatin 7 Chloroquinoline and 3hydroxyindole 7-Chloroquinoline Conjugates Synthesis and Antimalarial EvaluationDocument4 pages1H 1,2,3 Triazoletethered Isatin 7 Chloroquinoline and 3hydroxyindole 7-Chloroquinoline Conjugates Synthesis and Antimalarial EvaluationAcih AsihNo ratings yet
- Thyroid NodulesDocument7 pagesThyroid NodulesPravat SatpathyNo ratings yet
- CraniectomyDocument5 pagesCraniectomytabanaoNo ratings yet
- Toxikon Final GLP Report: 08-2140-G1Document21 pagesToxikon Final GLP Report: 08-2140-G1Tarun MishraNo ratings yet
- NCPDocument5 pagesNCPf_jm06_gNo ratings yet