
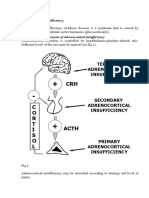
Adrenal Insufficiency.
Adrenal Insufficiency.
You might also like
- Addisons DiseaseDocument12 pagesAddisons DiseaseChinju CyrilNo ratings yet
- Endocrine System IntroductionDocument5 pagesEndocrine System IntroductionAnnapurna DangetiNo ratings yet
- Adrenal InsufficiencyDocument17 pagesAdrenal InsufficiencyHala AhmadNo ratings yet
- Adrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal MedicineDocument24 pagesAdrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal Medicineraed faisalNo ratings yet
- Adrenal Diseases: Types Aetiology Diagnosis Complications TreatmentDocument29 pagesAdrenal Diseases: Types Aetiology Diagnosis Complications Treatmentgani7222No ratings yet
- Adrenal InsufficiencyDocument25 pagesAdrenal InsufficiencyMustafa Salam M.NooriNo ratings yet
- Adrenal InsufficencyDocument48 pagesAdrenal InsufficencyAbood SamoudiNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- Adrenal Insufficiency and Cushing's Disease-1Document34 pagesAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Kuliah AdrenalDocument32 pagesKuliah AdrenalNindhyana Diwaratri R100% (1)
- Endo Lect 10Document22 pagesEndo Lect 10doctorrfarrukhNo ratings yet
- EndokrinDocument27 pagesEndokrinSarah Putri AbellysaNo ratings yet
- ENDO - Adrenal CrisisDocument8 pagesENDO - Adrenal CrisisHajime NakaegawaNo ratings yet
- Pathology of Adrenal Glands.Document41 pagesPathology of Adrenal Glands.Sukma Eka PratiwiNo ratings yet
- 6.28.10 Barnes Adrenal InsufficiencyDocument19 pages6.28.10 Barnes Adrenal InsufficiencySami OmerNo ratings yet
- Pathophysiology 101-823: Unit 5 Common Health ProblemsDocument17 pagesPathophysiology 101-823: Unit 5 Common Health ProblemsHaris NasutionNo ratings yet
- Summary of Medical EmergenciesDocument24 pagesSummary of Medical Emergenciesbasharswork99No ratings yet
- Addison Diseases LecDocument40 pagesAddison Diseases LecSalman RabbaniNo ratings yet
- Autoimmune Polyglandular Syndrome ReviewDocument3 pagesAutoimmune Polyglandular Syndrome ReviewIan AlvaradoNo ratings yet
- AddisonsdiseaseDocument5 pagesAddisonsdiseasenessimmounir1173No ratings yet
- 5) Adrenal GlandDocument74 pages5) Adrenal GlandABUBEKER BESHIRNo ratings yet
- Adrenal Gland DisordersDocument31 pagesAdrenal Gland DisordersThe AbyssinicansNo ratings yet
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- Exam 3 Review PDFDocument38 pagesExam 3 Review PDFunoNo ratings yet
- Adrenal Gland Diseades L 7band 8Document31 pagesAdrenal Gland Diseades L 7band 8lanasalah.mNo ratings yet
- ENDOCRINE DISORDERS (Autosaved)Document81 pagesENDOCRINE DISORDERS (Autosaved)Princewill SeiyefaNo ratings yet
- Adrenal InsufficiencyDocument2 pagesAdrenal InsufficiencyTracy NwanneNo ratings yet
- Adrenal Insufficiency & Adrenal Crisis: Emergency Medicine CH 217Document30 pagesAdrenal Insufficiency & Adrenal Crisis: Emergency Medicine CH 217Saroj Kanta SahuNo ratings yet
- Endocrinology NotesDocument12 pagesEndocrinology Notesrandiey john abelleraNo ratings yet
- Acute Biological CrisisDocument107 pagesAcute Biological CrisisJenes CernaNo ratings yet
- Adrenal PathophysiologyDocument5 pagesAdrenal PathophysiologyditabokNo ratings yet
- Endocrinology Course Content: Semester (5) Clinical Pharmacy CourseDocument91 pagesEndocrinology Course Content: Semester (5) Clinical Pharmacy CourseSadigMukhNo ratings yet
- EN9 - HypoadrenalismDocument8 pagesEN9 - Hypoadrenalismsbobine.imsNo ratings yet
- Endocrine System Pathology 2009Document195 pagesEndocrine System Pathology 2009SofiaemanginteNo ratings yet
- Shaina Dionisia Palacol Candice Guillermo Gelzan RoldanDocument55 pagesShaina Dionisia Palacol Candice Guillermo Gelzan RoldanEdelrose LapitanNo ratings yet
- Addison's DiseaseDocument3 pagesAddison's Diseaseavinash dhameriyaNo ratings yet
- AdrenalsDocument35 pagesAdrenalsMohammed MustafaNo ratings yet
- Adrenal Crisis: Risk FactorsDocument25 pagesAdrenal Crisis: Risk Factorspwinzizitah063No ratings yet
- Adrenal DisordersDocument26 pagesAdrenal DisordersAsif Ali LashariNo ratings yet
- Endocrine Study GuideDocument4 pagesEndocrine Study GuideNursingSchoolNotes100% (1)
- Study Guide For NURS 320 Exam 2Document15 pagesStudy Guide For NURS 320 Exam 2Anthony Del RioNo ratings yet
- Disease of Adrenal GlandDocument47 pagesDisease of Adrenal GlandgibreilNo ratings yet
- Cushing Syndrome and Addison's Disease: Rowena R, Tosoc RN, PHDDocument86 pagesCushing Syndrome and Addison's Disease: Rowena R, Tosoc RN, PHDMARICRIS NEBIARNo ratings yet
- Activity 2 MetabsDocument10 pagesActivity 2 MetabsCalvin Keith YadaoNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARI100% (1)
- Addisonian Crisis: Manish K Medical Officer IgmhDocument47 pagesAddisonian Crisis: Manish K Medical Officer IgmhNaaz Delhiwale100% (1)
- Endocrine Focus PointsDocument10 pagesEndocrine Focus PointsHayden ShulerNo ratings yet
- MRCPass Notes For MRCP 1 - EnDOCRINOLOGYDocument12 pagesMRCPass Notes For MRCP 1 - EnDOCRINOLOGYsabdali100% (1)
- Tertiary Adrenocortical InsufficiencyDocument8 pagesTertiary Adrenocortical InsufficiencysarathNo ratings yet
- Causes of Diffuse Hyperpigmentation EndocrinopathiesDocument9 pagesCauses of Diffuse Hyperpigmentation EndocrinopathiesAbdul QuyyumNo ratings yet
- Endocrinology Part 1Document131 pagesEndocrinology Part 1LucjaNo ratings yet
- Dentals Metabolic MedicineDocument37 pagesDentals Metabolic MedicineDavid McMahonNo ratings yet
- Hyperthyroidism . Management : Indications To Use Antithyroid Drugs IncludeDocument17 pagesHyperthyroidism . Management : Indications To Use Antithyroid Drugs IncludeBba Hab AleneNo ratings yet
- Primary and Secondary HyperparathyroidismDocument13 pagesPrimary and Secondary Hyperparathyroidismaileen agustinNo ratings yet
- Addison's DiseaseDocument57 pagesAddison's DiseaseVie Delvia100% (4)
- Endocrine System: Nila Kurniasari Dept Patologi Anatomi FK UnairDocument82 pagesEndocrine System: Nila Kurniasari Dept Patologi Anatomi FK UnairTidak Ada YangNo ratings yet
- Adrenal Insufficiency and Addison's DiseaseDocument8 pagesAdrenal Insufficiency and Addison's DiseaseFredy RizkiNo ratings yet
- EN8 - HypercortisolismDocument11 pagesEN8 - Hypercortisolismsbobine.imsNo ratings yet
- MCQs Endo FinalDocument6 pagesMCQs Endo Finalhassan qureshiNo ratings yet
- DSL - Thyroid Function TestDocument7 pagesDSL - Thyroid Function TestUmar AzlanNo ratings yet
- Kab ReetDocument254 pagesKab ReetAsia AlhkeemNo ratings yet
- Investigation Biological Reference Interval Observed Value UnitDocument3 pagesInvestigation Biological Reference Interval Observed Value UnitmadhuraNo ratings yet
- CHP 18Document40 pagesCHP 18Sophia YounNo ratings yet
- Male Reproductive SystemDocument27 pagesMale Reproductive System金 Abigail RodriguezNo ratings yet
- Reportpdf1 PDFDocument3 pagesReportpdf1 PDFLifetime AbbeyNo ratings yet
- Quiz 9 Human Reproduction Pregnancy Menstruation GraphsDocument4 pagesQuiz 9 Human Reproduction Pregnancy Menstruation GraphsCamille FrancoNo ratings yet
- ASSESSMENT With No AnswerDocument3 pagesASSESSMENT With No AnswerShielo Marie CabañeroNo ratings yet
- Thyroid & Antithyroid DrugsDocument27 pagesThyroid & Antithyroid DrugsjabirNo ratings yet
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyNo ratings yet
- Normal Ovaries On UltrasoundDocument1 pageNormal Ovaries On UltrasoundDr Pankaj TalwarNo ratings yet
- Biochemistry of HormoneDocument58 pagesBiochemistry of HormoneHaamim Sya'bani0% (1)
- Thyroid Disease in PregnancyDocument53 pagesThyroid Disease in PregnancyTee Wei SianNo ratings yet
- Hyperthyroidism Methimazole Radioactive Iodine 131Document1 pageHyperthyroidism Methimazole Radioactive Iodine 131Steven miles PunzalanNo ratings yet
- Parathyroid Gland: Dr. Mustafa Abdalgadir Khandgawi Ibrahim 2016Document24 pagesParathyroid Gland: Dr. Mustafa Abdalgadir Khandgawi Ibrahim 2016Mustafa KhandgawiNo ratings yet
- Sankha Jee Medical Receipt-18.08.2022Document12 pagesSankha Jee Medical Receipt-18.08.2022saajnaNo ratings yet
- Thyroid Function TestsDocument29 pagesThyroid Function TestsAkwesaNo ratings yet
- Mind Map On Endocrinology of Human For BSC StudentsDocument3 pagesMind Map On Endocrinology of Human For BSC Students2023ebcs499No ratings yet
- Patologi AnatomiDocument3 pagesPatologi Anatomidika anggrainniNo ratings yet
- Anatomy of The Endocrine System IIDocument129 pagesAnatomy of The Endocrine System IIShauie CayabyabNo ratings yet
- Physiology of Male ReproductionDocument19 pagesPhysiology of Male Reproductionalok nayakNo ratings yet
- Diagestive, Urinary and Reproductive SystemDocument39 pagesDiagestive, Urinary and Reproductive SystemCarolina Calle HerreraNo ratings yet
- 2ND Jaecl SMCD SND Pafes EngDocument43 pages2ND Jaecl SMCD SND Pafes EngEdouard AKAFOUNo ratings yet
- Let's Talk About Thyroid PDFDocument92 pagesLet's Talk About Thyroid PDFEidi IdhamNo ratings yet
- Quantum Yoga PDFDocument241 pagesQuantum Yoga PDFMohd AnowarNo ratings yet
- Bullets For CHNDocument4 pagesBullets For CHNWiljohn de la CruzNo ratings yet
- Hyperthyroidism 1Document34 pagesHyperthyroidism 1mussavir100% (2)
- Ch10 Lecture PPT ADocument62 pagesCh10 Lecture PPT AMiky rose De GuzmanNo ratings yet
- Maam Jean OR SCHED 10112022Document2 pagesMaam Jean OR SCHED 10112022Jean Camille Lazo MendozaNo ratings yet























































































Download as pdf or txt
You might also like
- Addisons DiseaseDocument12 pagesAddisons DiseaseChinju CyrilNo ratings yet
- Endocrine System IntroductionDocument5 pagesEndocrine System IntroductionAnnapurna DangetiNo ratings yet
- Adrenal InsufficiencyDocument17 pagesAdrenal InsufficiencyHala AhmadNo ratings yet
- Adrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal MedicineDocument24 pagesAdrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal Medicineraed faisalNo ratings yet
- Adrenal Diseases: Types Aetiology Diagnosis Complications TreatmentDocument29 pagesAdrenal Diseases: Types Aetiology Diagnosis Complications Treatmentgani7222No ratings yet
- Adrenal InsufficiencyDocument25 pagesAdrenal InsufficiencyMustafa Salam M.NooriNo ratings yet
- Adrenal InsufficencyDocument48 pagesAdrenal InsufficencyAbood SamoudiNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- Adrenal Insufficiency and Cushing's Disease-1Document34 pagesAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Kuliah AdrenalDocument32 pagesKuliah AdrenalNindhyana Diwaratri R100% (1)
- Endo Lect 10Document22 pagesEndo Lect 10doctorrfarrukhNo ratings yet
- EndokrinDocument27 pagesEndokrinSarah Putri AbellysaNo ratings yet
- ENDO - Adrenal CrisisDocument8 pagesENDO - Adrenal CrisisHajime NakaegawaNo ratings yet
- Pathology of Adrenal Glands.Document41 pagesPathology of Adrenal Glands.Sukma Eka PratiwiNo ratings yet
- 6.28.10 Barnes Adrenal InsufficiencyDocument19 pages6.28.10 Barnes Adrenal InsufficiencySami OmerNo ratings yet
- Pathophysiology 101-823: Unit 5 Common Health ProblemsDocument17 pagesPathophysiology 101-823: Unit 5 Common Health ProblemsHaris NasutionNo ratings yet
- Summary of Medical EmergenciesDocument24 pagesSummary of Medical Emergenciesbasharswork99No ratings yet
- Addison Diseases LecDocument40 pagesAddison Diseases LecSalman RabbaniNo ratings yet
- Autoimmune Polyglandular Syndrome ReviewDocument3 pagesAutoimmune Polyglandular Syndrome ReviewIan AlvaradoNo ratings yet
- AddisonsdiseaseDocument5 pagesAddisonsdiseasenessimmounir1173No ratings yet
- 5) Adrenal GlandDocument74 pages5) Adrenal GlandABUBEKER BESHIRNo ratings yet
- Adrenal Gland DisordersDocument31 pagesAdrenal Gland DisordersThe AbyssinicansNo ratings yet
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- Exam 3 Review PDFDocument38 pagesExam 3 Review PDFunoNo ratings yet
- Adrenal Gland Diseades L 7band 8Document31 pagesAdrenal Gland Diseades L 7band 8lanasalah.mNo ratings yet
- ENDOCRINE DISORDERS (Autosaved)Document81 pagesENDOCRINE DISORDERS (Autosaved)Princewill SeiyefaNo ratings yet
- Adrenal InsufficiencyDocument2 pagesAdrenal InsufficiencyTracy NwanneNo ratings yet
- Adrenal Insufficiency & Adrenal Crisis: Emergency Medicine CH 217Document30 pagesAdrenal Insufficiency & Adrenal Crisis: Emergency Medicine CH 217Saroj Kanta SahuNo ratings yet
- Endocrinology NotesDocument12 pagesEndocrinology Notesrandiey john abelleraNo ratings yet
- Acute Biological CrisisDocument107 pagesAcute Biological CrisisJenes CernaNo ratings yet
- Adrenal PathophysiologyDocument5 pagesAdrenal PathophysiologyditabokNo ratings yet
- Endocrinology Course Content: Semester (5) Clinical Pharmacy CourseDocument91 pagesEndocrinology Course Content: Semester (5) Clinical Pharmacy CourseSadigMukhNo ratings yet
- EN9 - HypoadrenalismDocument8 pagesEN9 - Hypoadrenalismsbobine.imsNo ratings yet
- Endocrine System Pathology 2009Document195 pagesEndocrine System Pathology 2009SofiaemanginteNo ratings yet
- Shaina Dionisia Palacol Candice Guillermo Gelzan RoldanDocument55 pagesShaina Dionisia Palacol Candice Guillermo Gelzan RoldanEdelrose LapitanNo ratings yet
- Addison's DiseaseDocument3 pagesAddison's Diseaseavinash dhameriyaNo ratings yet
- AdrenalsDocument35 pagesAdrenalsMohammed MustafaNo ratings yet
- Adrenal Crisis: Risk FactorsDocument25 pagesAdrenal Crisis: Risk Factorspwinzizitah063No ratings yet
- Adrenal DisordersDocument26 pagesAdrenal DisordersAsif Ali LashariNo ratings yet
- Endocrine Study GuideDocument4 pagesEndocrine Study GuideNursingSchoolNotes100% (1)
- Study Guide For NURS 320 Exam 2Document15 pagesStudy Guide For NURS 320 Exam 2Anthony Del RioNo ratings yet
- Disease of Adrenal GlandDocument47 pagesDisease of Adrenal GlandgibreilNo ratings yet
- Cushing Syndrome and Addison's Disease: Rowena R, Tosoc RN, PHDDocument86 pagesCushing Syndrome and Addison's Disease: Rowena R, Tosoc RN, PHDMARICRIS NEBIARNo ratings yet
- Activity 2 MetabsDocument10 pagesActivity 2 MetabsCalvin Keith YadaoNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARI100% (1)
- Addisonian Crisis: Manish K Medical Officer IgmhDocument47 pagesAddisonian Crisis: Manish K Medical Officer IgmhNaaz Delhiwale100% (1)
- Endocrine Focus PointsDocument10 pagesEndocrine Focus PointsHayden ShulerNo ratings yet
- MRCPass Notes For MRCP 1 - EnDOCRINOLOGYDocument12 pagesMRCPass Notes For MRCP 1 - EnDOCRINOLOGYsabdali100% (1)
- Tertiary Adrenocortical InsufficiencyDocument8 pagesTertiary Adrenocortical InsufficiencysarathNo ratings yet
- Causes of Diffuse Hyperpigmentation EndocrinopathiesDocument9 pagesCauses of Diffuse Hyperpigmentation EndocrinopathiesAbdul QuyyumNo ratings yet
- Endocrinology Part 1Document131 pagesEndocrinology Part 1LucjaNo ratings yet
- Dentals Metabolic MedicineDocument37 pagesDentals Metabolic MedicineDavid McMahonNo ratings yet
- Hyperthyroidism . Management : Indications To Use Antithyroid Drugs IncludeDocument17 pagesHyperthyroidism . Management : Indications To Use Antithyroid Drugs IncludeBba Hab AleneNo ratings yet
- Primary and Secondary HyperparathyroidismDocument13 pagesPrimary and Secondary Hyperparathyroidismaileen agustinNo ratings yet
- Addison's DiseaseDocument57 pagesAddison's DiseaseVie Delvia100% (4)
- Endocrine System: Nila Kurniasari Dept Patologi Anatomi FK UnairDocument82 pagesEndocrine System: Nila Kurniasari Dept Patologi Anatomi FK UnairTidak Ada YangNo ratings yet
- Adrenal Insufficiency and Addison's DiseaseDocument8 pagesAdrenal Insufficiency and Addison's DiseaseFredy RizkiNo ratings yet
- EN8 - HypercortisolismDocument11 pagesEN8 - Hypercortisolismsbobine.imsNo ratings yet
- MCQs Endo FinalDocument6 pagesMCQs Endo Finalhassan qureshiNo ratings yet
- DSL - Thyroid Function TestDocument7 pagesDSL - Thyroid Function TestUmar AzlanNo ratings yet
- Kab ReetDocument254 pagesKab ReetAsia AlhkeemNo ratings yet
- Investigation Biological Reference Interval Observed Value UnitDocument3 pagesInvestigation Biological Reference Interval Observed Value UnitmadhuraNo ratings yet
- CHP 18Document40 pagesCHP 18Sophia YounNo ratings yet
- Male Reproductive SystemDocument27 pagesMale Reproductive System金 Abigail RodriguezNo ratings yet
- Reportpdf1 PDFDocument3 pagesReportpdf1 PDFLifetime AbbeyNo ratings yet
- Quiz 9 Human Reproduction Pregnancy Menstruation GraphsDocument4 pagesQuiz 9 Human Reproduction Pregnancy Menstruation GraphsCamille FrancoNo ratings yet
- ASSESSMENT With No AnswerDocument3 pagesASSESSMENT With No AnswerShielo Marie CabañeroNo ratings yet
- Thyroid & Antithyroid DrugsDocument27 pagesThyroid & Antithyroid DrugsjabirNo ratings yet
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyNo ratings yet
- Normal Ovaries On UltrasoundDocument1 pageNormal Ovaries On UltrasoundDr Pankaj TalwarNo ratings yet
- Biochemistry of HormoneDocument58 pagesBiochemistry of HormoneHaamim Sya'bani0% (1)
- Thyroid Disease in PregnancyDocument53 pagesThyroid Disease in PregnancyTee Wei SianNo ratings yet
- Hyperthyroidism Methimazole Radioactive Iodine 131Document1 pageHyperthyroidism Methimazole Radioactive Iodine 131Steven miles PunzalanNo ratings yet
- Parathyroid Gland: Dr. Mustafa Abdalgadir Khandgawi Ibrahim 2016Document24 pagesParathyroid Gland: Dr. Mustafa Abdalgadir Khandgawi Ibrahim 2016Mustafa KhandgawiNo ratings yet
- Sankha Jee Medical Receipt-18.08.2022Document12 pagesSankha Jee Medical Receipt-18.08.2022saajnaNo ratings yet
- Thyroid Function TestsDocument29 pagesThyroid Function TestsAkwesaNo ratings yet
- Mind Map On Endocrinology of Human For BSC StudentsDocument3 pagesMind Map On Endocrinology of Human For BSC Students2023ebcs499No ratings yet
- Patologi AnatomiDocument3 pagesPatologi Anatomidika anggrainniNo ratings yet
- Anatomy of The Endocrine System IIDocument129 pagesAnatomy of The Endocrine System IIShauie CayabyabNo ratings yet
- Physiology of Male ReproductionDocument19 pagesPhysiology of Male Reproductionalok nayakNo ratings yet
- Diagestive, Urinary and Reproductive SystemDocument39 pagesDiagestive, Urinary and Reproductive SystemCarolina Calle HerreraNo ratings yet
- 2ND Jaecl SMCD SND Pafes EngDocument43 pages2ND Jaecl SMCD SND Pafes EngEdouard AKAFOUNo ratings yet
- Let's Talk About Thyroid PDFDocument92 pagesLet's Talk About Thyroid PDFEidi IdhamNo ratings yet
- Quantum Yoga PDFDocument241 pagesQuantum Yoga PDFMohd AnowarNo ratings yet
- Bullets For CHNDocument4 pagesBullets For CHNWiljohn de la CruzNo ratings yet
- Hyperthyroidism 1Document34 pagesHyperthyroidism 1mussavir100% (2)
- Ch10 Lecture PPT ADocument62 pagesCh10 Lecture PPT AMiky rose De GuzmanNo ratings yet
- Maam Jean OR SCHED 10112022Document2 pagesMaam Jean OR SCHED 10112022Jean Camille Lazo MendozaNo ratings yet