Download as pdf or txt
You might also like
- GCSE Psych Text BookDocument291 pagesGCSE Psych Text Bookn78% (9)
- 1987 - Marris - The Role and Impact of Mega-Events and Attractions On Regional and National Tourism Development ResolutionsDocument12 pages1987 - Marris - The Role and Impact of Mega-Events and Attractions On Regional and National Tourism Development ResolutionsJulia GCNo ratings yet
- Full BriefDocument52 pagesFull BriefDiana LongrieNo ratings yet
- Biotech Business PlanDocument3 pagesBiotech Business Plansarraz0% (1)
- Correctional Treatment of Violent Offenders.2014-Woessner-862-79Document18 pagesCorrectional Treatment of Violent Offenders.2014-Woessner-862-79Alexandra ParvanNo ratings yet
- Antipsychotic Treatment A Systematic Literature Review and Meta Analysis of Qualitative StudiesDocument12 pagesAntipsychotic Treatment A Systematic Literature Review and Meta Analysis of Qualitative StudiesmafeNo ratings yet
- Long-Term Effects of Psychedeli - Jacob S. AdayDocument11 pagesLong-Term Effects of Psychedeli - Jacob S. AdaysilentrevoNo ratings yet
- Artigo NFD Efficacy of Invasive and Non-Invasive Brain ModulationDocument23 pagesArtigo NFD Efficacy of Invasive and Non-Invasive Brain ModulationMarcelo MenezesNo ratings yet
- CBSP Pratt 2015Document11 pagesCBSP Pratt 2015Abdullah HasanNo ratings yet
- Music Therapy Improves Sleep Quality in Acute and ChronicDocument12 pagesMusic Therapy Improves Sleep Quality in Acute and ChronicLaras Ciingu SyahrezaNo ratings yet
- Prisoners LancetDocument7 pagesPrisoners LancetGodlady Sarah SOUSSIANo ratings yet
- Association of Sleep Duration and Quality With Blood LipidsDocument11 pagesAssociation of Sleep Duration and Quality With Blood Lipidsnajla nailufarNo ratings yet
- Atakan 2012Document13 pagesAtakan 2012DDD TTTNo ratings yet
- Antipsychotic Treatment - A Systematic Literature Review and Meta-Analysis of Qualitative StudiesDocument12 pagesAntipsychotic Treatment - A Systematic Literature Review and Meta-Analysis of Qualitative StudiesPriti BhosleNo ratings yet
- Ashkar - Views From The Inside Young Offenders' Subjective Experiences of IncarcerationDocument14 pagesAshkar - Views From The Inside Young Offenders' Subjective Experiences of IncarcerationZoe PeregrinaNo ratings yet
- Špela PDFDocument11 pagesŠpela PDFŠpela MiroševičNo ratings yet
- Vernoux EffectsCannabisAndPsychosisVulnerability (2003) PDFDocument10 pagesVernoux EffectsCannabisAndPsychosisVulnerability (2003) PDFPau RochaNo ratings yet
- Kall Et Al 2020Document10 pagesKall Et Al 2020365psychNo ratings yet
- Psychedelic MicrodosisDocument13 pagesPsychedelic MicrodosisFabio SantosNo ratings yet
- Cannabis Use in First Episode Psychosis: Meta-Analysis of Prevalence, and The Time Course of Initiation and Continued UseDocument12 pagesCannabis Use in First Episode Psychosis: Meta-Analysis of Prevalence, and The Time Course of Initiation and Continued UseFernandahzrNo ratings yet
- Shantal Mang InasalDocument7 pagesShantal Mang InasalShantal EsperaNo ratings yet
- Long Term Vs Short TermDocument9 pagesLong Term Vs Short TermHerizko KusumaNo ratings yet
- TENS - ArticleDocument10 pagesTENS - ArticleMickael LopesNo ratings yet
- Hilton Et Al 2019 Assessment of Risk For Seclusion Among Forensic Inpatients Validation and Modification of The Risk ofDocument22 pagesHilton Et Al 2019 Assessment of Risk For Seclusion Among Forensic Inpatients Validation and Modification of The Risk ofGurmeet chahalNo ratings yet
- Long-Term Effects of Cannabis On Brain StructureDocument8 pagesLong-Term Effects of Cannabis On Brain StructureRebecca DiasNo ratings yet
- Eclinicalmedicine: Research PaperDocument10 pagesEclinicalmedicine: Research PaperEvelynNo ratings yet
- Iseger and Bossong 2015 Schizophrenia ResearchDocument10 pagesIseger and Bossong 2015 Schizophrenia ResearchIgnacia PaezNo ratings yet
- Metaanalisis Psicoterapia Resultados PPLDocument20 pagesMetaanalisis Psicoterapia Resultados PPLXavierBilbaoNo ratings yet
- Benzodiazepinicos e Demencias 2012Document12 pagesBenzodiazepinicos e Demencias 2012Fábio VinholyNo ratings yet
- 1 s2.0 S0022395624002371 MainDocument8 pages1 s2.0 S0022395624002371 MainUmmu Hanik ThasaNo ratings yet
- A Longitudinal Outcome Evaluation of A Prison-Based Sex Offender Treatment ProgramDocument28 pagesA Longitudinal Outcome Evaluation of A Prison-Based Sex Offender Treatment ProgramCamila SorianoNo ratings yet
- Fazel Danesh 16feb2002Document9 pagesFazel Danesh 16feb2002Fajar YanuarNo ratings yet
- Nicotine Enhances Auditory Processing in Healthy and Normal-Hearing Young Adult NonsmokersDocument8 pagesNicotine Enhances Auditory Processing in Healthy and Normal-Hearing Young Adult NonsmokersSantiago MirandaNo ratings yet
- 1 s2.0 S0197455617300424 MainDocument9 pages1 s2.0 S0197455617300424 MainJulia LinzenboldNo ratings yet
- 10.1007@s11065 020 09443 7Document14 pages10.1007@s11065 020 09443 7José NettoNo ratings yet
- Health-Related Quality of Life in Narcolepsy: A Systematic Review and Meta - AnalysisDocument13 pagesHealth-Related Quality of Life in Narcolepsy: A Systematic Review and Meta - AnalysisHernán MarínNo ratings yet
- Nasim 2017Document1 pageNasim 2017Diego SantanaNo ratings yet
- Ecstasy Research PaperDocument8 pagesEcstasy Research Paperlyn0l1gamop2100% (1)
- Medication For Attention Deficit - Hyperactivity Disorder and CriminalityDocument9 pagesMedication For Attention Deficit - Hyperactivity Disorder and Criminalityd10140rezaNo ratings yet
- Mal de DebarquementDocument10 pagesMal de DebarquementFelipeAsenjoÁlvarezNo ratings yet
- Long Term Effects of Psychedelic Drugs A Systematic Review Jacob S Aday Full ChapterDocument33 pagesLong Term Effects of Psychedelic Drugs A Systematic Review Jacob S Aday Full Chapterjohnny.stevenson857100% (5)
- Prinsloo (2017)Document16 pagesPrinsloo (2017)Anonymous ovTI4eNo ratings yet
- Synthesis PaperDocument17 pagesSynthesis Paperapi-321753881No ratings yet
- Prof. Baldacchino - PonenciaDocument65 pagesProf. Baldacchino - Ponenciaverito3tresNo ratings yet
- Kroencke Et Al 2020 How Does Substance Use Affect Personality Development Disentangling Between and Within PersonDocument11 pagesKroencke Et Al 2020 How Does Substance Use Affect Personality Development Disentangling Between and Within Personcarllaurenceaquino53No ratings yet
- Jurnal POTDocument11 pagesJurnal POTSiti Arum WidiyantiNo ratings yet
- Osodi Mental Health AdolescentesDocument16 pagesOsodi Mental Health Adolescentespaulacastell1No ratings yet
- Drug and Alcohol DependenceDocument8 pagesDrug and Alcohol DependenceGilson Mariano NeryNo ratings yet
- Pesticida e DepressaoDocument5 pagesPesticida e DepressaoEduardo cardosoNo ratings yet
- Jsaa 086Document11 pagesJsaa 086Elías Coreas SotoNo ratings yet
- A Systematic Review of The Evidence of Clozapine's Anti-Aggressive EffectsDocument21 pagesA Systematic Review of The Evidence of Clozapine's Anti-Aggressive EffectsDivaNo ratings yet
- Sanna-Et-Al.-2019-1 TMSDocument10 pagesSanna-Et-Al.-2019-1 TMSgiovanna cannarellaNo ratings yet
- Clinical Effectiveness and Acceptability of StructDocument10 pagesClinical Effectiveness and Acceptability of StructArthur AlvesNo ratings yet
- Brachytherapy For The Palliation of Dysphagia Owing To Esop - 2017 - RadiotherapDocument8 pagesBrachytherapy For The Palliation of Dysphagia Owing To Esop - 2017 - RadiotherapFlorin AchimNo ratings yet
- Asian J. Med. Pharm. Res. 2 (3) 47-52, 2012Document6 pagesAsian J. Med. Pharm. Res. 2 (3) 47-52, 2012juandellibroNo ratings yet
- The Impact of Time Factors On Overall Survival in Patients With Nasopharyngeal Carcinoma: A Population-Based StudyDocument7 pagesThe Impact of Time Factors On Overall Survival in Patients With Nasopharyngeal Carcinoma: A Population-Based Studytami widiatul azahraNo ratings yet
- Lewczuk 2017Document12 pagesLewczuk 2017BarbaraNo ratings yet
- Guided Discontinuation Versus Maintenance Treatment in Remitted Firstepisode Psychosis Relapse Rates and Functional OutcomeDocument2 pagesGuided Discontinuation Versus Maintenance Treatment in Remitted Firstepisode Psychosis Relapse Rates and Functional Outcomewen zhangNo ratings yet
- Paroxetine, Cognitive Therapy or Their Combination in The Treatment of Social Anxiety Disorder With and Without Avoidant Personality Disorder: A Randomized Clinical TrialDocument11 pagesParoxetine, Cognitive Therapy or Their Combination in The Treatment of Social Anxiety Disorder With and Without Avoidant Personality Disorder: A Randomized Clinical TrialAdm Foto MahniteseNo ratings yet
- Aphasia Recovery: When, How and Who To Treat?Document7 pagesAphasia Recovery: When, How and Who To Treat?Mohammed Dr.adjedNo ratings yet
- Effect of Mortality Salience On Health Compromising BehaviorDocument6 pagesEffect of Mortality Salience On Health Compromising BehaviorIJAR JOURNALNo ratings yet
- Study of Cannabis Use Among Moroccan Medical Student and Anxio-Depressive ComorbidityDocument6 pagesStudy of Cannabis Use Among Moroccan Medical Student and Anxio-Depressive ComorbidityIJAR JOURNALNo ratings yet
- Jurnal DepresiDocument15 pagesJurnal DepresiDesi PratiwiNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- A Project Work On Study On Awareness of Health Insurance: Divaba Institute of Business AdministrationDocument58 pagesA Project Work On Study On Awareness of Health Insurance: Divaba Institute of Business Administration13 Mehul MandanakaNo ratings yet
- Critical Review of LiteratureDocument3 pagesCritical Review of LiteratureTomvie CephasNo ratings yet
- MB0040-Statistics For Management-Answer KeysDocument33 pagesMB0040-Statistics For Management-Answer KeysSanyo Gita50% (2)
- What Is Clinical PharmacyDocument4 pagesWhat Is Clinical PharmacySethiSheikhNo ratings yet
- Guidelines For The Evaluation of The Efficacy of Cosmetic Products - 2008Document18 pagesGuidelines For The Evaluation of The Efficacy of Cosmetic Products - 2008binal100% (1)
- ReadingDocument14 pagesReadingDeepikaNo ratings yet
- Friedman Habitus Clive 2016Document44 pagesFriedman Habitus Clive 2016JOHNATIELNo ratings yet
- 570 Assignment1-NguyenHuuThang-GBD1004Document30 pages570 Assignment1-NguyenHuuThang-GBD1004Ha Van Anh (FGW DN)No ratings yet
- FDA 21 CFR Part 11 PDFDocument2 pagesFDA 21 CFR Part 11 PDFRobert0% (1)
- Effect of Teamwork Employee Empowerment PDFDocument15 pagesEffect of Teamwork Employee Empowerment PDFAbdul HadiNo ratings yet
- Summary Changes ISO 9001 (2015)Document9 pagesSummary Changes ISO 9001 (2015)RomaidaNo ratings yet
- Pre-Operating Period: Part I: Management Aspect ADocument5 pagesPre-Operating Period: Part I: Management Aspect APaul George DomingoNo ratings yet
- Using Machine Learning Models To Predict S&P500 Price Level and Spread DirectionDocument6 pagesUsing Machine Learning Models To Predict S&P500 Price Level and Spread DirectionjajabinksNo ratings yet
- Civilandenvironmentalengineering PDFDocument11 pagesCivilandenvironmentalengineering PDFWanderley K. Shukaku Vallhonrat CnIcNo ratings yet
- Regression Discontinuity Models: Pavel CoronadoDocument63 pagesRegression Discontinuity Models: Pavel CoronadoDIEGO ALONSO GOMEZNo ratings yet
- Pengaruh Iklan Versi "Nyalakan Harapan" Terhadap Brand: Awareness Ramayana Di JakartaDocument4 pagesPengaruh Iklan Versi "Nyalakan Harapan" Terhadap Brand: Awareness Ramayana Di JakartaRenaldy BaptistaNo ratings yet
- Soria (2001) - WP19 (2) IlokanoDocument34 pagesSoria (2001) - WP19 (2) IlokanoCarol GalleonNo ratings yet
- Isaac Opoku-Mensah Resume PDFDocument1 pageIsaac Opoku-Mensah Resume PDFIsaac Opoku-MensahNo ratings yet
- Aveyard and Sharp Literature ReviewDocument4 pagesAveyard and Sharp Literature Reviewaflsqfsaw100% (1)
- 01.pengantar IMK Dan Konsep GUI - Web UIDocument18 pages01.pengantar IMK Dan Konsep GUI - Web UIluffy luffylandNo ratings yet
- GBV Needs Assessment Report - 2023-2024Document63 pagesGBV Needs Assessment Report - 2023-2024MaxNo ratings yet
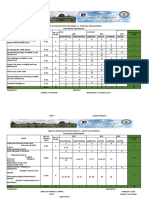
- Table of Specification For Grade 12 - Personal Development First Quarter ExaminationDocument17 pagesTable of Specification For Grade 12 - Personal Development First Quarter ExaminationArgie Joy Marie AmpolNo ratings yet
- T Statistic and Z Statics DifferenceDocument4 pagesT Statistic and Z Statics DifferenceMadison HartfieldNo ratings yet
- Variables: Sherine ShawkyDocument37 pagesVariables: Sherine ShawkyAbigail Basco100% (1)
- IGCW Attendees' List - EditableDocument7 pagesIGCW Attendees' List - EditableTaherNo ratings yet
- "This Is A Sponsored Blog Post, But All Opinions Are My Own" The Effects of Sponsorship Disclosure On Responses To Sponsored Blog PostsDocument8 pages"This Is A Sponsored Blog Post, But All Opinions Are My Own" The Effects of Sponsorship Disclosure On Responses To Sponsored Blog PostsqueengraciousNo ratings yet