
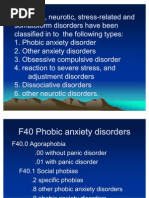
Neurotic, Stress-Related, Somatoform
Neurotic, Stress-Related, Somatoform
You might also like
- PayslipDocument1 pagePayslipAshish Agarwal67% (3)
- Red Light Camera Effectiveness EvaluationDocument33 pagesRed Light Camera Effectiveness EvaluationRochester Democrat and ChronicleNo ratings yet
- Anxiety DisordersDocument21 pagesAnxiety Disorderskarthikkanda100% (1)
- Systematic DesensitizationDocument6 pagesSystematic DesensitizationOniwura Bolarinwa OlapadeNo ratings yet
- List of Government WebsitesDocument1 pageList of Government Websitessumit-7No ratings yet
- Neurotic DisorderDocument180 pagesNeurotic DisordertendolsmithNo ratings yet
- Question 1-What Is Phobia?: Day 7 Assignment Give Brief Answers of Below Given QuestionsDocument3 pagesQuestion 1-What Is Phobia?: Day 7 Assignment Give Brief Answers of Below Given QuestionsashwinNo ratings yet
- Clinical Assessment and Diagnosis of Psychiatric Disorders-1Document118 pagesClinical Assessment and Diagnosis of Psychiatric Disorders-1arathy.smn.04No ratings yet
- Lecture 5 and 6-1Document35 pagesLecture 5 and 6-1هذيل أحمدNo ratings yet
- Anxiety DisordersDocument7 pagesAnxiety Disorderssuresh patilNo ratings yet
- PhobiasDocument22 pagesPhobiasSharizal SaklinNo ratings yet
- Anxiety Disorders FR ClassDocument11 pagesAnxiety Disorders FR ClassPranali M.No ratings yet
- Anxiety Disorders1Document12 pagesAnxiety Disorders1KURBULDKNo ratings yet
- Nature of Anxiety DisordersDocument6 pagesNature of Anxiety Disorderssanyamana935No ratings yet
- Anxiety Disorder ReviewerDocument3 pagesAnxiety Disorder ReviewerRhea Mae TabayagNo ratings yet
- PhobiaDocument19 pagesPhobiaMsRhyxelleNo ratings yet
- 1) Phobic Anxiety DisordersDocument12 pages1) Phobic Anxiety DisordersAzrina KhanNo ratings yet
- Anxiety Disorders - Lecture NotesDocument14 pagesAnxiety Disorders - Lecture NotesPeter Forster67% (3)
- Anxiety DisorderDocument11 pagesAnxiety DisorderBiswas AruNo ratings yet
- AnxietyDocument18 pagesAnxietyRizwana MBTNo ratings yet
- Almost Everyone Has An Irrational Fear or TwoDocument5 pagesAlmost Everyone Has An Irrational Fear or TwoEissej Jean NavarroNo ratings yet
- 02 Anxiety DisordersDocument9 pages02 Anxiety DisorderskayalvizhiNo ratings yet
- Screenshot 2020-01-13 at 2.35.04 PMDocument50 pagesScreenshot 2020-01-13 at 2.35.04 PMSharifah NabaahaNo ratings yet
- Instant Download PDF Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual Full ChapterDocument34 pagesInstant Download PDF Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual Full Chapterperarasut100% (8)
- Full download Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual all chapter 2024 pdfDocument44 pagesFull download Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual all chapter 2024 pdfnifstyra100% (9)
- ANxiety DisorderDocument6 pagesANxiety DisorderSahil AnsariNo ratings yet
- Anxiety DisordersDocument29 pagesAnxiety DisordersJince V JohnNo ratings yet
- Full Abnormal Psychology Plus New Mypsychlab 15Th Edition Butcher Solutions Manual Online PDF All ChapterDocument45 pagesFull Abnormal Psychology Plus New Mypsychlab 15Th Edition Butcher Solutions Manual Online PDF All Chaptercatharfnechfttagonfan100% (6)
- NeurosisDocument11 pagesNeurosisSharika sasiNo ratings yet
- Neurotic DisordersDocument59 pagesNeurotic DisordersCristy-Esther DocdocNo ratings yet
- Download Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual online ebook textbook full chapter pdfDocument23 pagesDownload Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual online ebook textbook full chapter pdftalipesangelicalhyfacNo ratings yet
- Add A Little Bit of Body Text PDFDocument2 pagesAdd A Little Bit of Body Text PDFsofia.loreen567No ratings yet
- Psychology 1 EADocument5 pagesPsychology 1 EAIan RamaNo ratings yet
- Anxiety Disorder-1Document14 pagesAnxiety Disorder-1Naeem Khan AfridiNo ratings yet
- Anxiety DisorderDocument56 pagesAnxiety DisorderDr TNTNo ratings yet
- Anxiety Disorders-Batch 17 Srik-Sept 2012Document57 pagesAnxiety Disorders-Batch 17 Srik-Sept 2012Sangkaran KumarNo ratings yet
- PhobiaDocument41 pagesPhobiaRujuta BaramateNo ratings yet
- Anxiety ReportDocument72 pagesAnxiety Reportcatherine faith gallemitNo ratings yet
- PhobiaDocument27 pagesPhobiasuresh patilNo ratings yet
- Anxiety DisordersDocument44 pagesAnxiety DisordersmanideepreddyNo ratings yet
- Anxiety DisorderDocument17 pagesAnxiety Disordergarimamahaur47No ratings yet
- Phobic DisordersDocument3 pagesPhobic Disorderssomebody_maNo ratings yet
- Anxiety Disorders Lecture NotesDocument9 pagesAnxiety Disorders Lecture NotesHerme BorladoNo ratings yet
- List of Phobias and Simple Cures PDFDocument40 pagesList of Phobias and Simple Cures PDFAnu KumarNo ratings yet
- Specific Phobias: What Is A Specific Phobia?Document6 pagesSpecific Phobias: What Is A Specific Phobia?Waseem QureshiNo ratings yet
- Phobia: IntroductionDocument7 pagesPhobia: IntroductionRachel SepthyNo ratings yet
- Anxiety DisorderDocument53 pagesAnxiety DisorderGene Espino Trajeco0% (1)
- ReviewerDocument5 pagesReviewerEvieNo ratings yet
- Unit-VI Anxiety DisordersDocument198 pagesUnit-VI Anxiety DisordersDemis TekleNo ratings yet
- PMH Panic DisorderDocument19 pagesPMH Panic Disorderycq5s9jdgnNo ratings yet
- PsicologiaDocument24 pagesPsicologiaPablo UlisesNo ratings yet
- Class II Neurotic DisordersDocument37 pagesClass II Neurotic DisordersNarayan K Ghorapde100% (1)
- Crim 201Document50 pagesCrim 201Tabaosares JeffreNo ratings yet
- Clinical PsychologyDocument26 pagesClinical PsychologyGURNOOR KAURNo ratings yet
- Anxiety DisordersDocument10 pagesAnxiety Disorderssrashta gargNo ratings yet
- AnumDocument18 pagesAnummusaweraghani25No ratings yet
- Anxiety-Related Disorders: by Joan SinghDocument41 pagesAnxiety-Related Disorders: by Joan SinghJoan SinghNo ratings yet
- Chapter 5 Anxiety, Trauma and Stressor - Related, Obsessive Compulsive Related DisordersDocument16 pagesChapter 5 Anxiety, Trauma and Stressor - Related, Obsessive Compulsive Related DisordersAnnie SumacotNo ratings yet
- Treatment Options For The Specific Phobias: IjbcpDocument6 pagesTreatment Options For The Specific Phobias: IjbcpMarius MoroianuNo ratings yet
- Social Phobia and Specific PhobiasDocument3 pagesSocial Phobia and Specific PhobiasRoci ArceNo ratings yet
- Anxiety Disorders: Moges Ayehu, MD, Psychiatrist Assistant Professor, HUCMHDocument38 pagesAnxiety Disorders: Moges Ayehu, MD, Psychiatrist Assistant Professor, HUCMHsoran muzeyinNo ratings yet
- EDMR Therapy: 2 Manuscripts in 1 - Harnessing Eye Movements for HealingFrom EverandEDMR Therapy: 2 Manuscripts in 1 - Harnessing Eye Movements for HealingNo ratings yet
- Multi-Component FTIR Emission Monitoring System: Abb Measurement & Analytics - Data SheetDocument16 pagesMulti-Component FTIR Emission Monitoring System: Abb Measurement & Analytics - Data SheetRonaldo JuniorNo ratings yet
- Soc TB 25 May 2017Document37 pagesSoc TB 25 May 2017Ipie BsaNo ratings yet
- Christmas Vigil MassDocument106 pagesChristmas Vigil MassMary JosephNo ratings yet
- API BasicsDocument6 pagesAPI BasicsSrinivas BathulaNo ratings yet
- Ultrasonic InterferometerDocument22 pagesUltrasonic InterferometerakshatguptaNo ratings yet
- PR m1Document15 pagesPR m1Jazmyn BulusanNo ratings yet
- In Search of Colonial El Ni No Events and A Brief History of Meteorology in EcuadorDocument7 pagesIn Search of Colonial El Ni No Events and A Brief History of Meteorology in EcuadorDanielNo ratings yet
- Aquamaster 4 Few4 and Fet4: Electromagnetic FlowmeterDocument48 pagesAquamaster 4 Few4 and Fet4: Electromagnetic FlowmeterAmol BorikarNo ratings yet
- FijiTimes - Feb 17 2012 Web PDFDocument48 pagesFijiTimes - Feb 17 2012 Web PDFfijitimescanadaNo ratings yet
- BitBox CarList 2022 10 28Document97 pagesBitBox CarList 2022 10 28marcos hernandezNo ratings yet
- CCC-BMG MOON 3-2 - Within Dwarvenholm v2.0Document30 pagesCCC-BMG MOON 3-2 - Within Dwarvenholm v2.0MarianoNo ratings yet
- KISI USP INGGRIS Kelas 12Document39 pagesKISI USP INGGRIS Kelas 12Deny Cahyo SaputroNo ratings yet
- Rahmania Tbi 6 D Soe...Document9 pagesRahmania Tbi 6 D Soe...Rahmania Aulia PurwagunifaNo ratings yet
- Steffes 5100 Tech Data SheetDocument4 pagesSteffes 5100 Tech Data SheetcringsredNo ratings yet
- Science TE804Document15 pagesScience TE804carolynhart_415No ratings yet
- 8DIO Claire Oboe Virtuoso ManualDocument10 pages8DIO Claire Oboe Virtuoso ManualNiskaNo ratings yet
- ScheduleDocument2 pagesScheduleJen NevalgaNo ratings yet
- Nemo Complete Documentation 2017Document65 pagesNemo Complete Documentation 2017Fredy A. CastañedaNo ratings yet
- How To Improve Battery Life of Your Galaxy Note 10 and Note 10Document18 pagesHow To Improve Battery Life of Your Galaxy Note 10 and Note 10rainpcruzNo ratings yet
- Beginner's Guide To SoloDocument12 pagesBeginner's Guide To SoloTiurNo ratings yet
- B94-6 R1995 E1984Document21 pagesB94-6 R1995 E1984zojoNo ratings yet
- 03 - Literature ReviewDocument9 pages03 - Literature ReviewKhant Wai YanNo ratings yet
- City Center Unifier Deployment PDFDocument35 pagesCity Center Unifier Deployment PDFSachin PatilNo ratings yet
- Find Me Phoenix Book 6 Stacey Kennedy Full ChapterDocument67 pagesFind Me Phoenix Book 6 Stacey Kennedy Full Chaptercatherine.anderegg828100% (21)
- Electrical Circuit Lab ManualDocument38 pagesElectrical Circuit Lab Manualecessec67% (3)
- LC1D32M7: Product Data SheetDocument7 pagesLC1D32M7: Product Data SheetCHAHRHLHOHSNo ratings yet























































































Download as docx, pdf, or txt
You might also like
- PayslipDocument1 pagePayslipAshish Agarwal67% (3)
- Red Light Camera Effectiveness EvaluationDocument33 pagesRed Light Camera Effectiveness EvaluationRochester Democrat and ChronicleNo ratings yet
- Anxiety DisordersDocument21 pagesAnxiety Disorderskarthikkanda100% (1)
- Systematic DesensitizationDocument6 pagesSystematic DesensitizationOniwura Bolarinwa OlapadeNo ratings yet
- List of Government WebsitesDocument1 pageList of Government Websitessumit-7No ratings yet
- Neurotic DisorderDocument180 pagesNeurotic DisordertendolsmithNo ratings yet
- Question 1-What Is Phobia?: Day 7 Assignment Give Brief Answers of Below Given QuestionsDocument3 pagesQuestion 1-What Is Phobia?: Day 7 Assignment Give Brief Answers of Below Given QuestionsashwinNo ratings yet
- Clinical Assessment and Diagnosis of Psychiatric Disorders-1Document118 pagesClinical Assessment and Diagnosis of Psychiatric Disorders-1arathy.smn.04No ratings yet
- Lecture 5 and 6-1Document35 pagesLecture 5 and 6-1هذيل أحمدNo ratings yet
- Anxiety DisordersDocument7 pagesAnxiety Disorderssuresh patilNo ratings yet
- PhobiasDocument22 pagesPhobiasSharizal SaklinNo ratings yet
- Anxiety Disorders FR ClassDocument11 pagesAnxiety Disorders FR ClassPranali M.No ratings yet
- Anxiety Disorders1Document12 pagesAnxiety Disorders1KURBULDKNo ratings yet
- Nature of Anxiety DisordersDocument6 pagesNature of Anxiety Disorderssanyamana935No ratings yet
- Anxiety Disorder ReviewerDocument3 pagesAnxiety Disorder ReviewerRhea Mae TabayagNo ratings yet
- PhobiaDocument19 pagesPhobiaMsRhyxelleNo ratings yet
- 1) Phobic Anxiety DisordersDocument12 pages1) Phobic Anxiety DisordersAzrina KhanNo ratings yet
- Anxiety Disorders - Lecture NotesDocument14 pagesAnxiety Disorders - Lecture NotesPeter Forster67% (3)
- Anxiety DisorderDocument11 pagesAnxiety DisorderBiswas AruNo ratings yet
- AnxietyDocument18 pagesAnxietyRizwana MBTNo ratings yet
- Almost Everyone Has An Irrational Fear or TwoDocument5 pagesAlmost Everyone Has An Irrational Fear or TwoEissej Jean NavarroNo ratings yet
- 02 Anxiety DisordersDocument9 pages02 Anxiety DisorderskayalvizhiNo ratings yet
- Screenshot 2020-01-13 at 2.35.04 PMDocument50 pagesScreenshot 2020-01-13 at 2.35.04 PMSharifah NabaahaNo ratings yet
- Instant Download PDF Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual Full ChapterDocument34 pagesInstant Download PDF Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual Full Chapterperarasut100% (8)
- Full download Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual all chapter 2024 pdfDocument44 pagesFull download Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual all chapter 2024 pdfnifstyra100% (9)
- ANxiety DisorderDocument6 pagesANxiety DisorderSahil AnsariNo ratings yet
- Anxiety DisordersDocument29 pagesAnxiety DisordersJince V JohnNo ratings yet
- Full Abnormal Psychology Plus New Mypsychlab 15Th Edition Butcher Solutions Manual Online PDF All ChapterDocument45 pagesFull Abnormal Psychology Plus New Mypsychlab 15Th Edition Butcher Solutions Manual Online PDF All Chaptercatharfnechfttagonfan100% (6)
- NeurosisDocument11 pagesNeurosisSharika sasiNo ratings yet
- Neurotic DisordersDocument59 pagesNeurotic DisordersCristy-Esther DocdocNo ratings yet
- Download Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual online ebook textbook full chapter pdfDocument23 pagesDownload Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual online ebook textbook full chapter pdftalipesangelicalhyfacNo ratings yet
- Add A Little Bit of Body Text PDFDocument2 pagesAdd A Little Bit of Body Text PDFsofia.loreen567No ratings yet
- Psychology 1 EADocument5 pagesPsychology 1 EAIan RamaNo ratings yet
- Anxiety Disorder-1Document14 pagesAnxiety Disorder-1Naeem Khan AfridiNo ratings yet
- Anxiety DisorderDocument56 pagesAnxiety DisorderDr TNTNo ratings yet
- Anxiety Disorders-Batch 17 Srik-Sept 2012Document57 pagesAnxiety Disorders-Batch 17 Srik-Sept 2012Sangkaran KumarNo ratings yet
- PhobiaDocument41 pagesPhobiaRujuta BaramateNo ratings yet
- Anxiety ReportDocument72 pagesAnxiety Reportcatherine faith gallemitNo ratings yet
- PhobiaDocument27 pagesPhobiasuresh patilNo ratings yet
- Anxiety DisordersDocument44 pagesAnxiety DisordersmanideepreddyNo ratings yet
- Anxiety DisorderDocument17 pagesAnxiety Disordergarimamahaur47No ratings yet
- Phobic DisordersDocument3 pagesPhobic Disorderssomebody_maNo ratings yet
- Anxiety Disorders Lecture NotesDocument9 pagesAnxiety Disorders Lecture NotesHerme BorladoNo ratings yet
- List of Phobias and Simple Cures PDFDocument40 pagesList of Phobias and Simple Cures PDFAnu KumarNo ratings yet
- Specific Phobias: What Is A Specific Phobia?Document6 pagesSpecific Phobias: What Is A Specific Phobia?Waseem QureshiNo ratings yet
- Phobia: IntroductionDocument7 pagesPhobia: IntroductionRachel SepthyNo ratings yet
- Anxiety DisorderDocument53 pagesAnxiety DisorderGene Espino Trajeco0% (1)
- ReviewerDocument5 pagesReviewerEvieNo ratings yet
- Unit-VI Anxiety DisordersDocument198 pagesUnit-VI Anxiety DisordersDemis TekleNo ratings yet
- PMH Panic DisorderDocument19 pagesPMH Panic Disorderycq5s9jdgnNo ratings yet
- PsicologiaDocument24 pagesPsicologiaPablo UlisesNo ratings yet
- Class II Neurotic DisordersDocument37 pagesClass II Neurotic DisordersNarayan K Ghorapde100% (1)
- Crim 201Document50 pagesCrim 201Tabaosares JeffreNo ratings yet
- Clinical PsychologyDocument26 pagesClinical PsychologyGURNOOR KAURNo ratings yet
- Anxiety DisordersDocument10 pagesAnxiety Disorderssrashta gargNo ratings yet
- AnumDocument18 pagesAnummusaweraghani25No ratings yet
- Anxiety-Related Disorders: by Joan SinghDocument41 pagesAnxiety-Related Disorders: by Joan SinghJoan SinghNo ratings yet
- Chapter 5 Anxiety, Trauma and Stressor - Related, Obsessive Compulsive Related DisordersDocument16 pagesChapter 5 Anxiety, Trauma and Stressor - Related, Obsessive Compulsive Related DisordersAnnie SumacotNo ratings yet
- Treatment Options For The Specific Phobias: IjbcpDocument6 pagesTreatment Options For The Specific Phobias: IjbcpMarius MoroianuNo ratings yet
- Social Phobia and Specific PhobiasDocument3 pagesSocial Phobia and Specific PhobiasRoci ArceNo ratings yet
- Anxiety Disorders: Moges Ayehu, MD, Psychiatrist Assistant Professor, HUCMHDocument38 pagesAnxiety Disorders: Moges Ayehu, MD, Psychiatrist Assistant Professor, HUCMHsoran muzeyinNo ratings yet
- EDMR Therapy: 2 Manuscripts in 1 - Harnessing Eye Movements for HealingFrom EverandEDMR Therapy: 2 Manuscripts in 1 - Harnessing Eye Movements for HealingNo ratings yet
- Multi-Component FTIR Emission Monitoring System: Abb Measurement & Analytics - Data SheetDocument16 pagesMulti-Component FTIR Emission Monitoring System: Abb Measurement & Analytics - Data SheetRonaldo JuniorNo ratings yet
- Soc TB 25 May 2017Document37 pagesSoc TB 25 May 2017Ipie BsaNo ratings yet
- Christmas Vigil MassDocument106 pagesChristmas Vigil MassMary JosephNo ratings yet
- API BasicsDocument6 pagesAPI BasicsSrinivas BathulaNo ratings yet
- Ultrasonic InterferometerDocument22 pagesUltrasonic InterferometerakshatguptaNo ratings yet
- PR m1Document15 pagesPR m1Jazmyn BulusanNo ratings yet
- In Search of Colonial El Ni No Events and A Brief History of Meteorology in EcuadorDocument7 pagesIn Search of Colonial El Ni No Events and A Brief History of Meteorology in EcuadorDanielNo ratings yet
- Aquamaster 4 Few4 and Fet4: Electromagnetic FlowmeterDocument48 pagesAquamaster 4 Few4 and Fet4: Electromagnetic FlowmeterAmol BorikarNo ratings yet
- FijiTimes - Feb 17 2012 Web PDFDocument48 pagesFijiTimes - Feb 17 2012 Web PDFfijitimescanadaNo ratings yet
- BitBox CarList 2022 10 28Document97 pagesBitBox CarList 2022 10 28marcos hernandezNo ratings yet
- CCC-BMG MOON 3-2 - Within Dwarvenholm v2.0Document30 pagesCCC-BMG MOON 3-2 - Within Dwarvenholm v2.0MarianoNo ratings yet
- KISI USP INGGRIS Kelas 12Document39 pagesKISI USP INGGRIS Kelas 12Deny Cahyo SaputroNo ratings yet
- Rahmania Tbi 6 D Soe...Document9 pagesRahmania Tbi 6 D Soe...Rahmania Aulia PurwagunifaNo ratings yet
- Steffes 5100 Tech Data SheetDocument4 pagesSteffes 5100 Tech Data SheetcringsredNo ratings yet
- Science TE804Document15 pagesScience TE804carolynhart_415No ratings yet
- 8DIO Claire Oboe Virtuoso ManualDocument10 pages8DIO Claire Oboe Virtuoso ManualNiskaNo ratings yet
- ScheduleDocument2 pagesScheduleJen NevalgaNo ratings yet
- Nemo Complete Documentation 2017Document65 pagesNemo Complete Documentation 2017Fredy A. CastañedaNo ratings yet
- How To Improve Battery Life of Your Galaxy Note 10 and Note 10Document18 pagesHow To Improve Battery Life of Your Galaxy Note 10 and Note 10rainpcruzNo ratings yet
- Beginner's Guide To SoloDocument12 pagesBeginner's Guide To SoloTiurNo ratings yet
- B94-6 R1995 E1984Document21 pagesB94-6 R1995 E1984zojoNo ratings yet
- 03 - Literature ReviewDocument9 pages03 - Literature ReviewKhant Wai YanNo ratings yet
- City Center Unifier Deployment PDFDocument35 pagesCity Center Unifier Deployment PDFSachin PatilNo ratings yet
- Find Me Phoenix Book 6 Stacey Kennedy Full ChapterDocument67 pagesFind Me Phoenix Book 6 Stacey Kennedy Full Chaptercatherine.anderegg828100% (21)
- Electrical Circuit Lab ManualDocument38 pagesElectrical Circuit Lab Manualecessec67% (3)
- LC1D32M7: Product Data SheetDocument7 pagesLC1D32M7: Product Data SheetCHAHRHLHOHSNo ratings yet