Download as pdf or txt
You might also like
- Commentary: Ophthalmic Increasing Operations ofDocument2 pagesCommentary: Ophthalmic Increasing Operations ofDurval SantosNo ratings yet
- 2005 PROF 018 OphthalmicPrimaryCare2005Document7 pages2005 PROF 018 OphthalmicPrimaryCare2005Annisa KhairunnisaNo ratings yet
- Investigation of The Efficacy of An Online ToolDocument9 pagesInvestigation of The Efficacy of An Online ToolDani DuneNo ratings yet
- 2016 Cataract Surgery Visual Outcomes andDocument11 pages2016 Cataract Surgery Visual Outcomes andnitaNo ratings yet
- Primary Eye Care, Community Ophthalmology and General Ophthalmology Author RCOphth - Welcome To The Royal College of OphthalmologistsDocument17 pagesPrimary Eye Care, Community Ophthalmology and General Ophthalmology Author RCOphth - Welcome To The Royal College of Ophthalmologistsshahil agazNo ratings yet
- Incidence of PostcataractDocument8 pagesIncidence of PostcataractSurendar KesavanNo ratings yet
- Why OptometryDocument30 pagesWhy OptometrysandiNo ratings yet
- Eye 2011154 ADocument7 pagesEye 2011154 AAmba PutraNo ratings yet
- Predictive Factors of Visual Outcome of Malaysian Cataract Patients: A Retrospective StudyDocument8 pagesPredictive Factors of Visual Outcome of Malaysian Cataract Patients: A Retrospective Studyanita adrianiNo ratings yet
- Keratoconus 2Document39 pagesKeratoconus 2YOSEF DERDESAWENo ratings yet
- Cataract BlindnessDocument4 pagesCataract BlindnessNandi DeviNo ratings yet
- Phacoemulsification Versus Small Incision Cataract Surgery For Treatment ofDocument7 pagesPhacoemulsification Versus Small Incision Cataract Surgery For Treatment ofRagni MishraNo ratings yet
- Good Practice in OrthokeratologyDocument12 pagesGood Practice in OrthokeratologyPhilip McNelsonNo ratings yet
- CataratasDocument15 pagesCataratasKaren GuevaraNo ratings yet
- Screening For Eye Disease: Our Role, Responsibility and Opportunity of ResearchDocument2 pagesScreening For Eye Disease: Our Role, Responsibility and Opportunity of ResearchPierre A. RodulfoNo ratings yet
- Posterior Capsular Rent Prevention and ManagementDocument20 pagesPosterior Capsular Rent Prevention and Managementkimie PazNo ratings yet
- An Experimental Training Support Framework For Eye Fundus Examination Skill DevelopmentDocument13 pagesAn Experimental Training Support Framework For Eye Fundus Examination Skill DevelopmentWalisson BarbosaNo ratings yet
- Modified AcceptedDocument28 pagesModified Acceptedaarushi singhNo ratings yet
- Refractive Surgery - The LancetDocument14 pagesRefractive Surgery - The Lancetaann86911No ratings yet
- Eclinicalmedicine: Research PaperDocument8 pagesEclinicalmedicine: Research Paperanita adrianiNo ratings yet
- Cost-Utility Analysis of Extending Public Health Insurance Coverage To Include Diabetic Retinopathy Screening by OptometristsDocument7 pagesCost-Utility Analysis of Extending Public Health Insurance Coverage To Include Diabetic Retinopathy Screening by OptometristsFatiyahSyahidaNo ratings yet
- An Algorithm For Thepreoperative DiagnosisDocument16 pagesAn Algorithm For Thepreoperative DiagnosismedellincolombiaNo ratings yet
- 1 Does Prospective Monitoring Improve Cataract SurgeryDocument5 pages1 Does Prospective Monitoring Improve Cataract SurgeryNizar Arif LazuardiNo ratings yet
- Ref 7Document19 pagesRef 7indah anggarainiNo ratings yet
- 167 FullDocument9 pages167 FullSartajHussainNo ratings yet
- Thesis Martijn VisserDocument146 pagesThesis Martijn Visserbismarkob47No ratings yet
- MataDocument16 pagesMataIslah NadilaNo ratings yet
- Lundstrom Etal JCRS 2018 Risk Factors For Refractive Error After Cataract SurgeryDocument16 pagesLundstrom Etal JCRS 2018 Risk Factors For Refractive Error After Cataract Surgeryhenok birukNo ratings yet
- 2021 Efficacy, Safety and Complications of Autologous Fat Grafting To The Eyelids and Periorbital Area A Systematic Review and Meta-AnalysisDocument18 pages2021 Efficacy, Safety and Complications of Autologous Fat Grafting To The Eyelids and Periorbital Area A Systematic Review and Meta-AnalysisDimitris RodriguezNo ratings yet
- Cataract Surgery Guidelines 2010 - SEPTEMBER 2010Document106 pagesCataract Surgery Guidelines 2010 - SEPTEMBER 2010Ida WilonaNo ratings yet
- Current Advances in Ophthalmic TechnologyFrom EverandCurrent Advances in Ophthalmic TechnologyParul IchhpujaniNo ratings yet
- 2 Can Artificial Intelligence Make Screening Faster, More Accurate, and More AccessibleDocument6 pages2 Can Artificial Intelligence Make Screening Faster, More Accurate, and More Accessible钟华No ratings yet
- Matching The Patient To The Intraocular Lens Preoperative Considerations To Optimize Surgical OutcomesDocument10 pagesMatching The Patient To The Intraocular Lens Preoperative Considerations To Optimize Surgical Outcomesakun kd876No ratings yet
- Real-Time Teleophthalmology Versus Face-To-Face Consultation: A Systematic ReviewDocument10 pagesReal-Time Teleophthalmology Versus Face-To-Face Consultation: A Systematic ReviewJatinderBaliNo ratings yet
- ManDocument6 pagesManNeko NekoNo ratings yet
- Oup Accepted Manuscript 2021Document11 pagesOup Accepted Manuscript 2021Camila Carvajal SilvaNo ratings yet
- J Esthet Restor Dent - 2023 - Pedrinaci - Multifunctional Anatomical Prototypes MAPs Treatment of Excessive GingivalDocument10 pagesJ Esthet Restor Dent - 2023 - Pedrinaci - Multifunctional Anatomical Prototypes MAPs Treatment of Excessive Gingivaljuan.vanegas.a1No ratings yet
- Efficacy of Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in Late Adolescents and Adults A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in Late Adolescents and Adults A Systematic Review and Meta-Analysisaa bbNo ratings yet
- Detecting Keratoconus From Corneal Imaging Data Using Machine LearningDocument9 pagesDetecting Keratoconus From Corneal Imaging Data Using Machine LearningProdeep kumarNo ratings yet
- Advances in Telemedicine in OphthalmologyDocument11 pagesAdvances in Telemedicine in OphthalmologyMoneer Ali tahaNo ratings yet
- 1 s2.0 S030057121830099X MainDocument8 pages1 s2.0 S030057121830099X Mainkiara wardanaNo ratings yet
- DMFR 20130291Document7 pagesDMFR 20130291Dragos CiongaruNo ratings yet
- Futuristic Advances That Might Change The Future of Oral Medicine and RadiologyDocument15 pagesFuturistic Advances That Might Change The Future of Oral Medicine and RadiologyIJAR JOURNALNo ratings yet
- A Comprehensive Classification To Full ADocument14 pagesA Comprehensive Classification To Full ACristina EneNo ratings yet
- Cataract Surgery in Patients With Corneal Opacities: Researcharticle Open AccessDocument10 pagesCataract Surgery in Patients With Corneal Opacities: Researcharticle Open AccesszulmiyettyNo ratings yet
- 67 1427640213 PDFDocument5 pages67 1427640213 PDFIene Dhiitta PramudNo ratings yet
- Wco Global Competency Model 2015-1Document73 pagesWco Global Competency Model 2015-1CHIMA ONWUKA MONGNo ratings yet
- Artificial Intelligence and Deep Learning in OphthalmologyDocument9 pagesArtificial Intelligence and Deep Learning in OphthalmologySilvia Rossa MuisNo ratings yet
- Lapsus Neuro FixDocument8 pagesLapsus Neuro FixEcyeNo ratings yet
- Comparison of Postoperative Refractive Outcome in Eyes UndergoingDocument9 pagesComparison of Postoperative Refractive Outcome in Eyes UndergoingAndi Ayu LestariNo ratings yet
- Go Gate 2010Document4 pagesGo Gate 2010Okta Eka SuryaniNo ratings yet
- Presentation 1Document24 pagesPresentation 1-Yohanes Firmansyah-No ratings yet
- Process Evaluation of A National Primary Eye Care Programme in RwandaDocument12 pagesProcess Evaluation of A National Primary Eye Care Programme in RwandaEvan McCartneyNo ratings yet
- Rapid Palatal ExpansionDocument24 pagesRapid Palatal Expansiondaniela2201No ratings yet
- Effective Cataract Surgical Coverage: An Indicator For Measuring Quality-Of-Care in The Context of Universal Health CoverageDocument13 pagesEffective Cataract Surgical Coverage: An Indicator For Measuring Quality-Of-Care in The Context of Universal Health CoverageriskhapangestikaNo ratings yet
- Femtosecond Laser-Assisted Versus PhacoemulsificationDocument13 pagesFemtosecond Laser-Assisted Versus Phacoemulsificationdhimas satriaNo ratings yet
- 1 s2.0 S0039625720300709 MainDocument23 pages1 s2.0 S0039625720300709 Mainneha midhaNo ratings yet
- An Ontology-Driven, Case-Based Clinical Decision Support Model For Removable Partial Denture DesignDocument8 pagesAn Ontology-Driven, Case-Based Clinical Decision Support Model For Removable Partial Denture Designteodor888No ratings yet
- Monitoring Progression of Retinitis Pigmentosa: Current Recommendations and Recent AdvancesDocument25 pagesMonitoring Progression of Retinitis Pigmentosa: Current Recommendations and Recent AdvancesArief RianraharjoNo ratings yet
- Use of Dental Radiography Among Lithuanian General Dentists: Scientific ArticlesDocument6 pagesUse of Dental Radiography Among Lithuanian General Dentists: Scientific ArticlesfghdhmdkhNo ratings yet
- Gea Neo Puff-2Document2 pagesGea Neo Puff-2Anisa AnisaNo ratings yet
- English TestDocument4 pagesEnglish TestYagesh GuptaNo ratings yet
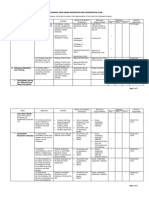
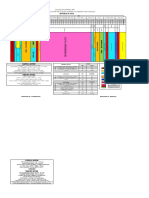
- For Companies - Sample - Three - Year Plan Matrix Revised 11.30.19Document5 pagesFor Companies - Sample - Three - Year Plan Matrix Revised 11.30.19Arnold RadaNo ratings yet
- Jurnal LukaDocument16 pagesJurnal Lukaqanitah olanNo ratings yet
- Leads Demo 20-Jan-24 14 44 09Document1 pageLeads Demo 20-Jan-24 14 44 09Raj TiwariNo ratings yet
- Feb - Deals For Agci ClientsDocument5 pagesFeb - Deals For Agci ClientsJancel James LimNo ratings yet
- Latihan Soal Tentang Public PlacesDocument3 pagesLatihan Soal Tentang Public PlacesSMPN 4 BANDARNo ratings yet
- Grey's Anatomy QuotesDocument11 pagesGrey's Anatomy QuoteslalikoNo ratings yet
- 298830Document34 pages298830Mohamed belhasan100% (1)
- EDITED Tle10 - He - Beautynailcareservices - q1 - Mod5 - Applyhandtreatment5 - v3-7-21Document22 pagesEDITED Tle10 - He - Beautynailcareservices - q1 - Mod5 - Applyhandtreatment5 - v3-7-21karl elordeNo ratings yet
- SPS Outdoor Cleaning Services: Hse Plan/ProgramDocument4 pagesSPS Outdoor Cleaning Services: Hse Plan/Programdhimas aditNo ratings yet
- V100 目錄含規格spec (標案)Document6 pagesV100 目錄含規格spec (標案)許善智No ratings yet
- MASTER ROTATION PLAN FOR 4TH YEAR B.SC NURSING 2020-2021Document4 pagesMASTER ROTATION PLAN FOR 4TH YEAR B.SC NURSING 2020-2021Bisakha DeyNo ratings yet
- All Vaccinees Are Requested To Bring Certificate of Dose-II From COWIN Portal Alongwith Registered Mobile Number Before Proceeding For VaccinationDocument2 pagesAll Vaccinees Are Requested To Bring Certificate of Dose-II From COWIN Portal Alongwith Registered Mobile Number Before Proceeding For VaccinationRakesh KumarNo ratings yet
- Heat Load Gupta Consultants & Associates: Lower BasementDocument2 pagesHeat Load Gupta Consultants & Associates: Lower BasementSameer UddinNo ratings yet
- Varieties of Medicinal Plants Found in Poblacion, Boljoon, CebuDocument5 pagesVarieties of Medicinal Plants Found in Poblacion, Boljoon, CebuCharles Dave AvenidoNo ratings yet
- 3shape Implant Studio Drilling ProtocolDocument2 pages3shape Implant Studio Drilling Protocolnha khoa NHƯ NGỌCNo ratings yet
- Dear MR Shamsi Vuai NahodhaDocument2 pagesDear MR Shamsi Vuai NahodhaShamsi NahodhaNo ratings yet
- Energearadionics RatesDocument163 pagesEnergearadionics RatesRoberta & Thomas NormanNo ratings yet
- Sherlyn Pablo-Pablo - 2023 Senior Project Proposal FormDocument4 pagesSherlyn Pablo-Pablo - 2023 Senior Project Proposal Formapi-663260468No ratings yet
- Oral-Motor Skills - Assessment and Treatment FormDocument2 pagesOral-Motor Skills - Assessment and Treatment FormBagus Satrio hadiNo ratings yet
- FINAL Announcement 22nd CNE 2023Document25 pagesFINAL Announcement 22nd CNE 2023hajjahnurainahNo ratings yet
- Brgy. Nabulao - Drug Cleared Cert.Document3 pagesBrgy. Nabulao - Drug Cleared Cert.Emily BondadNo ratings yet
- Advertisement GAMCDocument2 pagesAdvertisement GAMCParul SharmaNo ratings yet
- How To Become A Mercy General Hospital VolunteerDocument6 pagesHow To Become A Mercy General Hospital VolunteerShabnam AlizadaNo ratings yet
- NO Nama Alkes KegunaanDocument10 pagesNO Nama Alkes KegunaanIntan AisyahNo ratings yet
- KF - 07 - Blood Grouping 2019 - 03 - enDocument4 pagesKF - 07 - Blood Grouping 2019 - 03 - enSurta DevianaNo ratings yet
- Pricelist Harga ObatDocument22 pagesPricelist Harga ObatNIRMALANo ratings yet
- HIRA - Installation of Shot Blast BoothDocument9 pagesHIRA - Installation of Shot Blast BoothAniket autiNo ratings yet
- Dexametasone: No Nama Obat Sediaan Jumlah Satua N Harga Beli Harga JualDocument1 pageDexametasone: No Nama Obat Sediaan Jumlah Satua N Harga Beli Harga Jualfebri12No ratings yet