
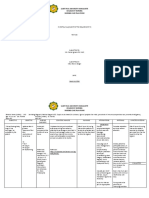
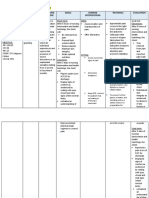
Group 1A - 1 Nursing Care Plan
Group 1A - 1 Nursing Care Plan
You might also like
- Foundation of Special and Inclusive Education Post TestDocument12 pagesFoundation of Special and Inclusive Education Post TestNico John Bauzon Capua100% (10)
- Nursing Care Plan Post Op & Intra OpDocument2 pagesNursing Care Plan Post Op & Intra OpLei Ortega85% (48)
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- Septic Arthritis NCPDocument3 pagesSeptic Arthritis NCPMae Therese B. MAGNO0% (1)
- NCP Pain1Document4 pagesNCP Pain1java_biscocho12290% (1)
- 3011-1 - NCP & Drug Study - AMCDocument5 pages3011-1 - NCP & Drug Study - AMCAngie MandeoyaNo ratings yet
- BL ChartDocument10 pagesBL ChartElizabeth Durkee NeilNo ratings yet
- Or NCPDocument5 pagesOr NCPjelopigar921No ratings yet
- Nursing Care Plan (Patient 1) : Subjective: "Meron Pa RinDocument2 pagesNursing Care Plan (Patient 1) : Subjective: "Meron Pa RinROD MARK DOMINIC ESTABILLONo ratings yet
- UntitledDocument5 pagesUntitledJayelles Dixien JuguilonNo ratings yet
- Nursing Care Plan Age: 60 Years OldDocument4 pagesNursing Care Plan Age: 60 Years OldLouise GudmalinNo ratings yet
- MeningitisDocument17 pagesMeningitisDanielNo ratings yet
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- Rafin NCP and Drug StudyDocument7 pagesRafin NCP and Drug StudyCezanne CruzNo ratings yet
- Tupas, Denzel C. Arrmc Duty-Ncp ActivityDocument13 pagesTupas, Denzel C. Arrmc Duty-Ncp ActivityDen TupasNo ratings yet
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- Pain - Post Partum MotherDocument2 pagesPain - Post Partum Motherulrikov91% (11)
- Cues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale EvaluationDocument11 pagesCues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale Evaluationjoyrena ochondraNo ratings yet
- Saint Paul University Dumaguete College of Nursing Nursing Care Plan FormDocument10 pagesSaint Paul University Dumaguete College of Nursing Nursing Care Plan FormMary Rose Silva GargarNo ratings yet
- NCP FractureDocument7 pagesNCP FractureMacris BondocNo ratings yet
- Graded Pedia NCPDocument4 pagesGraded Pedia NCPsalma.nasr003No ratings yet
- Nursing Process Care Plan Format: Patient Is A Non-SmokerDocument2 pagesNursing Process Care Plan Format: Patient Is A Non-SmokerDavid PerezNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDocument1 pageAssessment Nursing Diagnosis Planning Implementation Rationale EvaluationJames PajarilloNo ratings yet
- Preop Appendectomy NCPDocument3 pagesPreop Appendectomy NCPMyra AtuleNo ratings yet
- Risk For Acute Pain Related To Surgical IncisionDocument4 pagesRisk For Acute Pain Related To Surgical IncisionMia Grace Garcia100% (1)
- Brain Surgery Post Op NCPDocument6 pagesBrain Surgery Post Op NCPunnamed personNo ratings yet
- Case Stduy Med SurgDocument5 pagesCase Stduy Med SurgKevean Kimi LimNo ratings yet
- Nursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NDocument7 pagesNursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NNajla Kaye PerezNo ratings yet
- Medical Management-Nursing Management and NCP For Acute ApendicitisDocument4 pagesMedical Management-Nursing Management and NCP For Acute ApendicitisArki ObusanNo ratings yet
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationsDocument3 pagesAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationsAjay SupanNo ratings yet
- Assessment Diagnosis Analysis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Analysis Planning Intervention Rationale Evaluationy3nkieNo ratings yet
- NCP DengueDocument3 pagesNCP DengueNecy Tessa C. AcostaNo ratings yet
- Manguiat, Ncma 111 RomeoDocument4 pagesManguiat, Ncma 111 RomeoCiara ManguiatNo ratings yet
- Evidence Summary - Cancer PainDocument12 pagesEvidence Summary - Cancer PainErnesto LlorcaNo ratings yet
- NCP Proper CholecystectomyDocument2 pagesNCP Proper CholecystectomyGail Lian SantosNo ratings yet
- NCP Proper CholecystectomyDocument2 pagesNCP Proper CholecystectomyGail Lian SantosNo ratings yet
- Nursing Science Journal (NSJ) : e-ISSN: 2722-5054Document5 pagesNursing Science Journal (NSJ) : e-ISSN: 2722-5054Iskandar PakayaNo ratings yet
- TB NCPDocument1 pageTB NCPPatricia JuatNo ratings yet
- 17-Article Text-37-2-10-20200615.id - enDocument4 pages17-Article Text-37-2-10-20200615.id - enIskandar PakayaNo ratings yet
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- Emergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Document5 pagesEmergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Wyen CabatbatNo ratings yet
- NAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXDocument2 pagesNAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXTyn TynNo ratings yet
- Drug Study Threatened AbortionDocument4 pagesDrug Study Threatened AbortionKath CastilloNo ratings yet
- NCP For HemorrhoidsDocument3 pagesNCP For HemorrhoidsTADURAN RENE MAE ANGELLI F.No ratings yet
- Kusain - NCP in NCM 112 RleDocument2 pagesKusain - NCP in NCM 112 Rlejay kusainNo ratings yet
- NCP Drug StudyDocument5 pagesNCP Drug StudyAndrea JoyaNo ratings yet
- Reboca, Cristelle Joy M. NCPDocument5 pagesReboca, Cristelle Joy M. NCPCristelle Joy RebocaNo ratings yet
- Acupuncture and Pain: A Review of The Literature: Ladan Eshkevari, CRNA, MS, Dipl. AcDocument10 pagesAcupuncture and Pain: A Review of The Literature: Ladan Eshkevari, CRNA, MS, Dipl. AcRatrika SariNo ratings yet
- Accupressure, Pain 4Document5 pagesAccupressure, Pain 4Akmal ThariqNo ratings yet
- Cues Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation Subjective: Short TermDocument7 pagesCues Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation Subjective: Short TermOUR LADY OF FATIMA UNIVERSITY COLLEGENo ratings yet
- Acute PainDocument3 pagesAcute PainHu DawiNo ratings yet
- Nursing Care Plan PneumoniaDocument4 pagesNursing Care Plan PneumoniaIsaac KipkemoiNo ratings yet
- Alinsangao, Nashwa N. BSN 3B - NCP & DxsDocument3 pagesAlinsangao, Nashwa N. BSN 3B - NCP & DxsNASHWA NASLUN. ALINSANGAONo ratings yet
- BERNARDO - Dash 6 (NCP)Document1 pageBERNARDO - Dash 6 (NCP)Aurea Marie PinedaNo ratings yet
- NCP 3503Document2 pagesNCP 3503Natasha Jean CardonaNo ratings yet
- NCP Pain TeresitoDocument3 pagesNCP Pain TeresitoTheresa Reyes De JesusNo ratings yet
- Ms II NCPDocument2 pagesMs II NCPABIL ABU BAKARNo ratings yet
- "Naga Pan Luya Lang Ang Lawas Ko"as Verbalized by The PatientDocument3 pages"Naga Pan Luya Lang Ang Lawas Ko"as Verbalized by The PatientJamie Grace AbitNo ratings yet
- Subjective Cues: Short Term Goal: Short Term GoalDocument4 pagesSubjective Cues: Short Term Goal: Short Term GoalLarr SumalpongNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Doh Do 0223Document19 pagesDoh Do 0223J Velasco PeraltaNo ratings yet
- Jamur FusariumDocument5 pagesJamur FusariumHISANA AFIFANo ratings yet
- CBD DR Saugi IrfanDocument88 pagesCBD DR Saugi IrfanFebri BimayanaNo ratings yet
- Family Nursing Care PlanDocument7 pagesFamily Nursing Care PlanMarilou Jumalon MontefalconNo ratings yet
- Community and Public Health For MLS - LectureDocument49 pagesCommunity and Public Health For MLS - Lecturetorreb8396No ratings yet
- Volume 42, Issue 34 - August 26, 2011Document56 pagesVolume 42, Issue 34 - August 26, 2011BladeNo ratings yet
- Pharmacology IIIDocument2 pagesPharmacology IIITejasNo ratings yet
- Scopus Database Journal 02 NovDocument25 pagesScopus Database Journal 02 Novnaresh kotraNo ratings yet
- THROMBOSISDocument18 pagesTHROMBOSISShruti Verma100% (1)
- Biology - Kertas 1 Pep Pertengahan Tahun MPP2 Terengganu 2020 - SoalanDocument25 pagesBiology - Kertas 1 Pep Pertengahan Tahun MPP2 Terengganu 2020 - SoalanJessheila JoyceNo ratings yet
- 8940Document166 pages8940Basory Ok OkNo ratings yet
- Krissa and Drentlaw Visual Acuity The Critical Measure!Document18 pagesKrissa and Drentlaw Visual Acuity The Critical Measure!Jolien WalravenNo ratings yet
- Physical Assessment ToolDocument21 pagesPhysical Assessment ToolAmal LR100% (1)
- The Impact Of-Covid 19 Pandemic On The Academic Performance of Online Learning Students in Ismael Mathay Sr. High School During The School Year 2020-2021Document12 pagesThe Impact Of-Covid 19 Pandemic On The Academic Performance of Online Learning Students in Ismael Mathay Sr. High School During The School Year 2020-2021Jenalyn Bugaay100% (1)
- Incorporating Mindfulness Meditation Into The Treatment of Provoked VestibulodyniaDocument10 pagesIncorporating Mindfulness Meditation Into The Treatment of Provoked VestibulodyniaPau VRNo ratings yet
- Patanjali 2 (VinodDocument77 pagesPatanjali 2 (VinodgoswamiphotostatNo ratings yet
- (Unit 4) The Great Visionaries (: Questions and Answers)Document2 pages(Unit 4) The Great Visionaries (: Questions and Answers)Wikki Wasif100% (1)
- The Human Machine by RL Bijlani, SK ManchandaDocument176 pagesThe Human Machine by RL Bijlani, SK ManchandaMUSKANNo ratings yet
- Gmail Maxicare EReady Advance PDFDocument7 pagesGmail Maxicare EReady Advance PDFShirelyNo ratings yet
- Mina Drug StudyDocument7 pagesMina Drug StudyChi Chaw Giselle HilarioNo ratings yet
- 7th Symbiosis B Krishna Memorial National Moot Court Competition 2015 MDocument29 pages7th Symbiosis B Krishna Memorial National Moot Court Competition 2015 MChirag AhluwaliaNo ratings yet
- Cureus 0014 00000032158Document8 pagesCureus 0014 00000032158Daniel Martinez HernándezNo ratings yet
- 427 EndoDocument9 pages427 EndoBioq. GallegosNo ratings yet
- Lecture 1 - General Properties and Classification of FungiDocument4 pagesLecture 1 - General Properties and Classification of FungiRemelou Garchitorena AlfelorNo ratings yet
- BloodlettingDocument5 pagesBloodlettingMaria Lana Grace DiazNo ratings yet
- OpenDocument198 pagesOpenlaura fonsecaNo ratings yet
- Bali BellyDocument3 pagesBali BellyAstri KarmilaNo ratings yet
- Bryophyllum Pinnatum: (Katakataka)Document7 pagesBryophyllum Pinnatum: (Katakataka)JeemCarloFagelaPulaNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Foundation of Special and Inclusive Education Post TestDocument12 pagesFoundation of Special and Inclusive Education Post TestNico John Bauzon Capua100% (10)
- Nursing Care Plan Post Op & Intra OpDocument2 pagesNursing Care Plan Post Op & Intra OpLei Ortega85% (48)
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- Septic Arthritis NCPDocument3 pagesSeptic Arthritis NCPMae Therese B. MAGNO0% (1)
- NCP Pain1Document4 pagesNCP Pain1java_biscocho12290% (1)
- 3011-1 - NCP & Drug Study - AMCDocument5 pages3011-1 - NCP & Drug Study - AMCAngie MandeoyaNo ratings yet
- BL ChartDocument10 pagesBL ChartElizabeth Durkee NeilNo ratings yet
- Or NCPDocument5 pagesOr NCPjelopigar921No ratings yet
- Nursing Care Plan (Patient 1) : Subjective: "Meron Pa RinDocument2 pagesNursing Care Plan (Patient 1) : Subjective: "Meron Pa RinROD MARK DOMINIC ESTABILLONo ratings yet
- UntitledDocument5 pagesUntitledJayelles Dixien JuguilonNo ratings yet
- Nursing Care Plan Age: 60 Years OldDocument4 pagesNursing Care Plan Age: 60 Years OldLouise GudmalinNo ratings yet
- MeningitisDocument17 pagesMeningitisDanielNo ratings yet
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- Rafin NCP and Drug StudyDocument7 pagesRafin NCP and Drug StudyCezanne CruzNo ratings yet
- Tupas, Denzel C. Arrmc Duty-Ncp ActivityDocument13 pagesTupas, Denzel C. Arrmc Duty-Ncp ActivityDen TupasNo ratings yet
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- Pain - Post Partum MotherDocument2 pagesPain - Post Partum Motherulrikov91% (11)
- Cues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale EvaluationDocument11 pagesCues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale Evaluationjoyrena ochondraNo ratings yet
- Saint Paul University Dumaguete College of Nursing Nursing Care Plan FormDocument10 pagesSaint Paul University Dumaguete College of Nursing Nursing Care Plan FormMary Rose Silva GargarNo ratings yet
- NCP FractureDocument7 pagesNCP FractureMacris BondocNo ratings yet
- Graded Pedia NCPDocument4 pagesGraded Pedia NCPsalma.nasr003No ratings yet
- Nursing Process Care Plan Format: Patient Is A Non-SmokerDocument2 pagesNursing Process Care Plan Format: Patient Is A Non-SmokerDavid PerezNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDocument1 pageAssessment Nursing Diagnosis Planning Implementation Rationale EvaluationJames PajarilloNo ratings yet
- Preop Appendectomy NCPDocument3 pagesPreop Appendectomy NCPMyra AtuleNo ratings yet
- Risk For Acute Pain Related To Surgical IncisionDocument4 pagesRisk For Acute Pain Related To Surgical IncisionMia Grace Garcia100% (1)
- Brain Surgery Post Op NCPDocument6 pagesBrain Surgery Post Op NCPunnamed personNo ratings yet
- Case Stduy Med SurgDocument5 pagesCase Stduy Med SurgKevean Kimi LimNo ratings yet
- Nursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NDocument7 pagesNursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NNajla Kaye PerezNo ratings yet
- Medical Management-Nursing Management and NCP For Acute ApendicitisDocument4 pagesMedical Management-Nursing Management and NCP For Acute ApendicitisArki ObusanNo ratings yet
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationsDocument3 pagesAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationsAjay SupanNo ratings yet
- Assessment Diagnosis Analysis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Analysis Planning Intervention Rationale Evaluationy3nkieNo ratings yet
- NCP DengueDocument3 pagesNCP DengueNecy Tessa C. AcostaNo ratings yet
- Manguiat, Ncma 111 RomeoDocument4 pagesManguiat, Ncma 111 RomeoCiara ManguiatNo ratings yet
- Evidence Summary - Cancer PainDocument12 pagesEvidence Summary - Cancer PainErnesto LlorcaNo ratings yet
- NCP Proper CholecystectomyDocument2 pagesNCP Proper CholecystectomyGail Lian SantosNo ratings yet
- NCP Proper CholecystectomyDocument2 pagesNCP Proper CholecystectomyGail Lian SantosNo ratings yet
- Nursing Science Journal (NSJ) : e-ISSN: 2722-5054Document5 pagesNursing Science Journal (NSJ) : e-ISSN: 2722-5054Iskandar PakayaNo ratings yet
- TB NCPDocument1 pageTB NCPPatricia JuatNo ratings yet
- 17-Article Text-37-2-10-20200615.id - enDocument4 pages17-Article Text-37-2-10-20200615.id - enIskandar PakayaNo ratings yet
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- Emergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Document5 pagesEmergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Wyen CabatbatNo ratings yet
- NAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXDocument2 pagesNAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXTyn TynNo ratings yet
- Drug Study Threatened AbortionDocument4 pagesDrug Study Threatened AbortionKath CastilloNo ratings yet
- NCP For HemorrhoidsDocument3 pagesNCP For HemorrhoidsTADURAN RENE MAE ANGELLI F.No ratings yet
- Kusain - NCP in NCM 112 RleDocument2 pagesKusain - NCP in NCM 112 Rlejay kusainNo ratings yet
- NCP Drug StudyDocument5 pagesNCP Drug StudyAndrea JoyaNo ratings yet
- Reboca, Cristelle Joy M. NCPDocument5 pagesReboca, Cristelle Joy M. NCPCristelle Joy RebocaNo ratings yet
- Acupuncture and Pain: A Review of The Literature: Ladan Eshkevari, CRNA, MS, Dipl. AcDocument10 pagesAcupuncture and Pain: A Review of The Literature: Ladan Eshkevari, CRNA, MS, Dipl. AcRatrika SariNo ratings yet
- Accupressure, Pain 4Document5 pagesAccupressure, Pain 4Akmal ThariqNo ratings yet
- Cues Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation Subjective: Short TermDocument7 pagesCues Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation Subjective: Short TermOUR LADY OF FATIMA UNIVERSITY COLLEGENo ratings yet
- Acute PainDocument3 pagesAcute PainHu DawiNo ratings yet
- Nursing Care Plan PneumoniaDocument4 pagesNursing Care Plan PneumoniaIsaac KipkemoiNo ratings yet
- Alinsangao, Nashwa N. BSN 3B - NCP & DxsDocument3 pagesAlinsangao, Nashwa N. BSN 3B - NCP & DxsNASHWA NASLUN. ALINSANGAONo ratings yet
- BERNARDO - Dash 6 (NCP)Document1 pageBERNARDO - Dash 6 (NCP)Aurea Marie PinedaNo ratings yet
- NCP 3503Document2 pagesNCP 3503Natasha Jean CardonaNo ratings yet
- NCP Pain TeresitoDocument3 pagesNCP Pain TeresitoTheresa Reyes De JesusNo ratings yet
- Ms II NCPDocument2 pagesMs II NCPABIL ABU BAKARNo ratings yet
- "Naga Pan Luya Lang Ang Lawas Ko"as Verbalized by The PatientDocument3 pages"Naga Pan Luya Lang Ang Lawas Ko"as Verbalized by The PatientJamie Grace AbitNo ratings yet
- Subjective Cues: Short Term Goal: Short Term GoalDocument4 pagesSubjective Cues: Short Term Goal: Short Term GoalLarr SumalpongNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Doh Do 0223Document19 pagesDoh Do 0223J Velasco PeraltaNo ratings yet
- Jamur FusariumDocument5 pagesJamur FusariumHISANA AFIFANo ratings yet
- CBD DR Saugi IrfanDocument88 pagesCBD DR Saugi IrfanFebri BimayanaNo ratings yet
- Family Nursing Care PlanDocument7 pagesFamily Nursing Care PlanMarilou Jumalon MontefalconNo ratings yet
- Community and Public Health For MLS - LectureDocument49 pagesCommunity and Public Health For MLS - Lecturetorreb8396No ratings yet
- Volume 42, Issue 34 - August 26, 2011Document56 pagesVolume 42, Issue 34 - August 26, 2011BladeNo ratings yet
- Pharmacology IIIDocument2 pagesPharmacology IIITejasNo ratings yet
- Scopus Database Journal 02 NovDocument25 pagesScopus Database Journal 02 Novnaresh kotraNo ratings yet
- THROMBOSISDocument18 pagesTHROMBOSISShruti Verma100% (1)
- Biology - Kertas 1 Pep Pertengahan Tahun MPP2 Terengganu 2020 - SoalanDocument25 pagesBiology - Kertas 1 Pep Pertengahan Tahun MPP2 Terengganu 2020 - SoalanJessheila JoyceNo ratings yet
- 8940Document166 pages8940Basory Ok OkNo ratings yet
- Krissa and Drentlaw Visual Acuity The Critical Measure!Document18 pagesKrissa and Drentlaw Visual Acuity The Critical Measure!Jolien WalravenNo ratings yet
- Physical Assessment ToolDocument21 pagesPhysical Assessment ToolAmal LR100% (1)
- The Impact Of-Covid 19 Pandemic On The Academic Performance of Online Learning Students in Ismael Mathay Sr. High School During The School Year 2020-2021Document12 pagesThe Impact Of-Covid 19 Pandemic On The Academic Performance of Online Learning Students in Ismael Mathay Sr. High School During The School Year 2020-2021Jenalyn Bugaay100% (1)
- Incorporating Mindfulness Meditation Into The Treatment of Provoked VestibulodyniaDocument10 pagesIncorporating Mindfulness Meditation Into The Treatment of Provoked VestibulodyniaPau VRNo ratings yet
- Patanjali 2 (VinodDocument77 pagesPatanjali 2 (VinodgoswamiphotostatNo ratings yet
- (Unit 4) The Great Visionaries (: Questions and Answers)Document2 pages(Unit 4) The Great Visionaries (: Questions and Answers)Wikki Wasif100% (1)
- The Human Machine by RL Bijlani, SK ManchandaDocument176 pagesThe Human Machine by RL Bijlani, SK ManchandaMUSKANNo ratings yet
- Gmail Maxicare EReady Advance PDFDocument7 pagesGmail Maxicare EReady Advance PDFShirelyNo ratings yet
- Mina Drug StudyDocument7 pagesMina Drug StudyChi Chaw Giselle HilarioNo ratings yet
- 7th Symbiosis B Krishna Memorial National Moot Court Competition 2015 MDocument29 pages7th Symbiosis B Krishna Memorial National Moot Court Competition 2015 MChirag AhluwaliaNo ratings yet
- Cureus 0014 00000032158Document8 pagesCureus 0014 00000032158Daniel Martinez HernándezNo ratings yet
- 427 EndoDocument9 pages427 EndoBioq. GallegosNo ratings yet
- Lecture 1 - General Properties and Classification of FungiDocument4 pagesLecture 1 - General Properties and Classification of FungiRemelou Garchitorena AlfelorNo ratings yet
- BloodlettingDocument5 pagesBloodlettingMaria Lana Grace DiazNo ratings yet
- OpenDocument198 pagesOpenlaura fonsecaNo ratings yet
- Bali BellyDocument3 pagesBali BellyAstri KarmilaNo ratings yet
- Bryophyllum Pinnatum: (Katakataka)Document7 pagesBryophyllum Pinnatum: (Katakataka)JeemCarloFagelaPulaNo ratings yet