Download as pdf or txt
You might also like
- Lorma Colleges Patient Health History Related Learning ExperienceDocument2 pagesLorma Colleges Patient Health History Related Learning Experienceivy annNo ratings yet
- Ect SopDocument6 pagesEct Sopqonita0% (1)
- How To Read A Medical ReportDocument3 pagesHow To Read A Medical ReportpinkuNo ratings yet
- Modern Blue 2Document1 pageModern Blue 2Michaël HenrotteNo ratings yet
- 2019 Article 696 PDFDocument22 pages2019 Article 696 PDFAnonymous 0TOLgQWuHvNo ratings yet
- An Overview of Meningiomas: ReviewDocument18 pagesAn Overview of Meningiomas: ReviewMuhammad Naqvi Al FarisiNo ratings yet
- Jkns 57 315Document8 pagesJkns 57 315arcobaleno589No ratings yet
- Prognostic Factors Affecting Survial and Recurrence in Patientes With Early Cervical Squamous Cell Cancer Following Radical HTDocument13 pagesPrognostic Factors Affecting Survial and Recurrence in Patientes With Early Cervical Squamous Cell Cancer Following Radical HTfernandallmagalhaesNo ratings yet
- Jurnal KedokteranDocument9 pagesJurnal KedokteranannisanoviaNo ratings yet
- 247 2011 Article 2201 PDFDocument13 pages247 2011 Article 2201 PDFArdianNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- Insular GliomaDocument11 pagesInsular GliomaEdin HajdarpasicNo ratings yet
- Biblio 19Document22 pagesBiblio 19JuanchoNo ratings yet
- Internal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionDocument3 pagesInternal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionmarrajoanaNo ratings yet
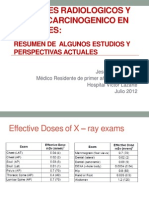
- Examenes Radiologicos y Riesgo de Cancer en PacientesDocument27 pagesExamenes Radiologicos y Riesgo de Cancer en PacientesMaría Isabel Clara Aponte OrtizNo ratings yet
- BJR Brain MetastasisDocument12 pagesBJR Brain MetastasisKarla RiosNo ratings yet
- Review Article: Screening For Lung Cancer With Low-Dose Computed Tomography: A Review of Current StatusDocument16 pagesReview Article: Screening For Lung Cancer With Low-Dose Computed Tomography: A Review of Current StatusAnnizada Intan PratiwiNo ratings yet
- Jgo 27 E1Document10 pagesJgo 27 E1Angga Witra NandaNo ratings yet
- Exploring Vismodegig A Non-Surgical Breakthrough in The Management of Advanced Periocular Basal Cell CarcinomaDocument11 pagesExploring Vismodegig A Non-Surgical Breakthrough in The Management of Advanced Periocular Basal Cell CarcinomaGeorgios LavasidisNo ratings yet
- AsianJNeurosurg10150-2524489 070044 PDFDocument4 pagesAsianJNeurosurg10150-2524489 070044 PDFSucipto HartonoNo ratings yet
- Completion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessDocument7 pagesCompletion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessRadita Dwihaning PutriNo ratings yet
- Minimamenteinvasiva FullDocument7 pagesMinimamenteinvasiva FullLuis OrtizNo ratings yet
- Ann Oncol 2010 Stupp v190 3Document4 pagesAnn Oncol 2010 Stupp v190 3Aryantii AntyNo ratings yet
- Understanding GBMDocument13 pagesUnderstanding GBMayelengiselbochatay@hotmail.comNo ratings yet
- Robotic Surgery in Pediatric Oncology: Lessons Learned From The First 100 Tumors-A Nationwide ExperienceDocument12 pagesRobotic Surgery in Pediatric Oncology: Lessons Learned From The First 100 Tumors-A Nationwide ExperiencePriyank YadavNo ratings yet
- Cancers 14 03161Document10 pagesCancers 14 03161Majd AssaadNo ratings yet
- NIH Public Access: Author ManuscriptDocument22 pagesNIH Public Access: Author ManuscriptHumberto QuimeNo ratings yet
- As Trocito MaDocument10 pagesAs Trocito Majeimy_carolina4163No ratings yet
- RT PediatricDocument9 pagesRT Pediatricfaza mawaddahNo ratings yet
- MeningiomaDocument31 pagesMeningiomaJamie PalmeriNo ratings yet
- Minimally Invasive Surgery in Pediatric Oncology Galazka 2019Document11 pagesMinimally Invasive Surgery in Pediatric Oncology Galazka 2019jonays_0106293No ratings yet
- Synopsis Format Brain Tumor JhulelalDocument22 pagesSynopsis Format Brain Tumor Jhulelalraymar2kNo ratings yet
- Fractionated Radiation For MeningiomasDocument2 pagesFractionated Radiation For MeningiomasGil LedermanNo ratings yet
- Articol Pe HartieDocument11 pagesArticol Pe HartieAndrei CUCUNo ratings yet
- Esmo Clinical GuidelinesDocument3 pagesEsmo Clinical GuidelinesAbdi Hakin MohamedNo ratings yet
- BMC CancerDocument9 pagesBMC CancerJohnson JamesNo ratings yet
- Van Der Heijden - Recurrence, Progression and FU of NMIBCDocument7 pagesVan Der Heijden - Recurrence, Progression and FU of NMIBCKeith YuenNo ratings yet
- Angiosarcoma MamaDocument5 pagesAngiosarcoma MamaRaul Matute MartinNo ratings yet
- Bli RenDocument5 pagesBli RenCharles RichardNo ratings yet
- Local Control in Metastatic Neuroblastoma in Children Over 1 Year of AgeDocument8 pagesLocal Control in Metastatic Neuroblastoma in Children Over 1 Year of AgePutri ManurungNo ratings yet
- Case Anemia Thalasemia FixDocument4 pagesCase Anemia Thalasemia FixmasranraisaNo ratings yet
- A Review of Newly Diagnosed GlioblastomaDocument10 pagesA Review of Newly Diagnosed Glioblastomaafdhal.888980No ratings yet
- Nuclear Medicine Imaging in Neuroblastoma: Current Status and New DevelopmentsDocument22 pagesNuclear Medicine Imaging in Neuroblastoma: Current Status and New DevelopmentsAdiNNo ratings yet
- 2019 Article 5894 PDFDocument8 pages2019 Article 5894 PDFGalgalo GarbichaNo ratings yet
- Brain Metastases: Andrew D. Norden, Patrick Y. Wen and Santosh KesariDocument8 pagesBrain Metastases: Andrew D. Norden, Patrick Y. Wen and Santosh KesarideepaneshNo ratings yet
- Neuro-Oncology Advances: Introduction To Radiomics and Radiogenomics in Neuro-Oncology: Implications and ChallengesDocument12 pagesNeuro-Oncology Advances: Introduction To Radiomics and Radiogenomics in Neuro-Oncology: Implications and ChallengesPriyanka VermaNo ratings yet
- IJMECE160531Document7 pagesIJMECE160531Senthil PNo ratings yet
- A Rare Huge Myxofibrosarcoma of Chest WallDocument3 pagesA Rare Huge Myxofibrosarcoma of Chest WallIOSRjournalNo ratings yet
- Jurnal ReadingDocument8 pagesJurnal ReadingHezar SalahudinNo ratings yet
- Tugas Ibu RetinoblastomaDocument7 pagesTugas Ibu RetinoblastomamalaNo ratings yet
- DV2 - 1007 3432 3 EdDocument12 pagesDV2 - 1007 3432 3 EdZannuba NoorNo ratings yet
- 6 Postoperative Radiation Therapy in The Management of Head and Neck Cancer - UpToDateDocument16 pages6 Postoperative Radiation Therapy in The Management of Head and Neck Cancer - UpToDateMarco GornattiNo ratings yet
- 01 Lung Cancer Diagnosis Based On UltrasoundDocument6 pages01 Lung Cancer Diagnosis Based On UltrasoundSaifulhadi BarohNo ratings yet
- A Major Issue in MedicineDocument29 pagesA Major Issue in MedicineSiti NajwaNo ratings yet
- Prognostic Value of Metabolic Tumor Burden On F-FDG PET in Nonsurgical Patients With Non-Small Cell Lung CancerDocument12 pagesPrognostic Value of Metabolic Tumor Burden On F-FDG PET in Nonsurgical Patients With Non-Small Cell Lung CancerAmina GoharyNo ratings yet
- MicroRNA-based Risk Scoring System To Identify EarDocument14 pagesMicroRNA-based Risk Scoring System To Identify EarDavidNo ratings yet
- Ewing's Sarcoma Review ArticleDocument9 pagesEwing's Sarcoma Review ArticleSayan DasNo ratings yet
- Contemporary Thyroid Nodule Evaluation and Management: Endocrinol Metab 105: 1-15, 2020)Document15 pagesContemporary Thyroid Nodule Evaluation and Management: Endocrinol Metab 105: 1-15, 2020)Rosane DiasNo ratings yet
- Contemporary Thyroid Nodule Evaluation and ManagemenDocument34 pagesContemporary Thyroid Nodule Evaluation and ManagemensamuelNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleGrace Juniaty GozaliNo ratings yet
- Pi Is 1879850016300947Document7 pagesPi Is 1879850016300947Daniela GordeaNo ratings yet
- International Seminars in Surgical OncologyDocument8 pagesInternational Seminars in Surgical OncologyAhmad ShafiqNo ratings yet
- Glioma Imaging: Physiologic, Metabolic, and Molecular ApproachesFrom EverandGlioma Imaging: Physiologic, Metabolic, and Molecular ApproachesWhitney B. PopeNo ratings yet
- Session 3.1-Vaccine Administration (Urdu)Document2 pagesSession 3.1-Vaccine Administration (Urdu)Mudassar PatelNo ratings yet
- Oropharyngeal and Nasopharyngeal SuctioningDocument2 pagesOropharyngeal and Nasopharyngeal SuctioningAlana Caballero100% (1)
- Rinhs Science 8 4th Catch Up Activity 2 Digestive System Crossword PuzzleDocument2 pagesRinhs Science 8 4th Catch Up Activity 2 Digestive System Crossword PuzzleRyan BersaminNo ratings yet
- X-Rays: Click To Add TextDocument43 pagesX-Rays: Click To Add TextAhmedNo ratings yet
- Stem CellsDocument58 pagesStem CellsRakesh Kumar100% (2)
- Bab 7Document27 pagesBab 7bangarudaugtherNo ratings yet
- GONORRHOEADocument23 pagesGONORRHOEADwi Fikha AprilyantiNo ratings yet
- What Is BacteriaDocument33 pagesWhat Is Bacteriaapi-19862227100% (1)
- Radiology of MSKDocument54 pagesRadiology of MSKgabriellafelisaNo ratings yet
- Trifluridine and TipiracilDocument3 pagesTrifluridine and TipiracilKristine AcasioNo ratings yet
- Biofilms and Quorum SensingDocument71 pagesBiofilms and Quorum Sensingzawar mughalNo ratings yet
- (From The Department of Bacteriology, School of Medicine, American University of Beirut, Beirut, Syria) Plates 64 A CD 65Document18 pages(From The Department of Bacteriology, School of Medicine, American University of Beirut, Beirut, Syria) Plates 64 A CD 65diantinurwindaNo ratings yet
- 2.nutrition Guide For Physicians PDFDocument444 pages2.nutrition Guide For Physicians PDFMauro Lopez100% (2)
- Physiology of The Cerebrospinal FluidDocument6 pagesPhysiology of The Cerebrospinal FluidShereen Al-ObinayNo ratings yet
- Drug Study - SulindacDocument3 pagesDrug Study - SulindacThalia UyNo ratings yet
- Abnormal Liver Function Test LGHDocument35 pagesAbnormal Liver Function Test LGHElaineNo ratings yet
- Group 3 QUIZDocument4 pagesGroup 3 QUIZJessa Mae OhaoNo ratings yet
- 1 Administering OxygenDocument6 pages1 Administering OxygentlokingNo ratings yet
- Pharmacology NotesDocument30 pagesPharmacology NotesJessica WalkerNo ratings yet
- Prostate Ca Flow ChartDocument5 pagesProstate Ca Flow ChartDanekka Tan100% (1)
- OPHTHA Case Report Diabetic RetinopathyDocument51 pagesOPHTHA Case Report Diabetic RetinopathyJessa MeaNo ratings yet
- Katara KDocument4 pagesKatara KAmirah Jihan AfryNo ratings yet
- Obs & GynDocument121 pagesObs & GynSaya K. AkremNo ratings yet
- Kantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Document6 pagesKantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Ic-tika Siee ChuabbieNo ratings yet
- Hepatitis B (HepB Vaccine)Document6 pagesHepatitis B (HepB Vaccine)Desiree EscobidoNo ratings yet
- The Measurement of Serum Osmolality and Its Application To Clinical Practice and Laboratory: Literature ReviewDocument8 pagesThe Measurement of Serum Osmolality and Its Application To Clinical Practice and Laboratory: Literature ReviewAkbar TaufikNo ratings yet
- Orthognathic SurgeryDocument26 pagesOrthognathic Surgerym.n.n .q.c.fNo ratings yet