
Tna Instrument - General
Tna Instrument - General
You might also like
- 5 DVP Assignment CIPD Level 5Document31 pages5 DVP Assignment CIPD Level 5Nomadiclahas Vagabond टीटो89% (54)
- HR Training and Development QuestionnaireDocument5 pagesHR Training and Development QuestionnaireAnis Tajuldin100% (3)
- Training Impact Assessment QuestionnaireDocument6 pagesTraining Impact Assessment QuestionnaireRuby Garcia50% (6)
- The Ultimate Guide To Job Interview Answers1Document92 pagesThe Ultimate Guide To Job Interview Answers1Oana Si Cristi Mocanu86% (7)
- Complete Audio Mastering: Practical TechniquesFrom EverandComplete Audio Mastering: Practical TechniquesRating: 5 out of 5 stars5/5 (5)
- Appendix I Interview Guide For TANESCO Magomeni Zone EmployeesDocument4 pagesAppendix I Interview Guide For TANESCO Magomeni Zone EmployeesSadelick KihongosiNo ratings yet
- Appendix (2) The Close-Ended Questions, Which Are Asked To The TraineesDocument4 pagesAppendix (2) The Close-Ended Questions, Which Are Asked To The TraineesAsadulla KhanNo ratings yet
- May 2018 Unmeb Examination Centre Accreditation ToolDocument26 pagesMay 2018 Unmeb Examination Centre Accreditation Toolopioamos260No ratings yet
- Course Assessment Form Date .. . Course Title: . Facilitator: Location: .. 1Document1 pageCourse Assessment Form Date .. . Course Title: . Facilitator: Location: .. 1Rony LesbtNo ratings yet
- HR Training and Development QuestionnaireDocument4 pagesHR Training and Development QuestionnaireShariful Islam Shaheen100% (3)
- Kingsway-Application Form, Teacher-22Document7 pagesKingsway-Application Form, Teacher-22anon-719393No ratings yet
- Exam Final S 8Document5 pagesExam Final S 8Salma A.No ratings yet
- Summer Internship Feedback DCEA, GLA UnivDocument2 pagesSummer Internship Feedback DCEA, GLA UnivMANSI SINHANo ratings yet
- Nysc National Directorate HeadquartersDocument4 pagesNysc National Directorate HeadquartersABDULRAHMAN YAHAYA (SIR-AB)No ratings yet
- Apr ViDocument4 pagesApr ViITI JammuNo ratings yet
- How Can You Assess The Effectiveness of Training and Development of Your Organization?Document11 pagesHow Can You Assess The Effectiveness of Training and Development of Your Organization?bonyNo ratings yet
- EDI National Master Trainer Success Story Collection Form V2 As of Dec 31, 2024 FinalDocument4 pagesEDI National Master Trainer Success Story Collection Form V2 As of Dec 31, 2024 FinalYonatan BizuworkNo ratings yet
- Ace Credit - Tesol For BusinessDocument176 pagesAce Credit - Tesol For Businessmilo060712No ratings yet
- Industrial Training Fund: Students Industrial Work Experience Scheme End of Year Programreport SheetDocument2 pagesIndustrial Training Fund: Students Industrial Work Experience Scheme End of Year Programreport Sheetjessica Emmanuel100% (1)
- QuestionnaireDocument3 pagesQuestionnaireKASHIF NAWAZNo ratings yet
- Application Form PDFDocument3 pagesApplication Form PDFmthabisi nyathiNo ratings yet
- Questionnaire On Information About HRD in TelecommunicationDocument8 pagesQuestionnaire On Information About HRD in Telecommunicationway2pritiNo ratings yet
- PSC Job Application Form 1J - SRC (1) (1)Document10 pagesPSC Job Application Form 1J - SRC (1) (1)Mercy Chepkorir KilisioNo ratings yet
- Section A: Respondents BackgroundDocument2 pagesSection A: Respondents BackgroundOoi See ChongNo ratings yet
- Annual Confidential Report of The Work and Conduct of Teachers of Aided/Unaided Recognised SchoolsDocument7 pagesAnnual Confidential Report of The Work and Conduct of Teachers of Aided/Unaided Recognised SchoolsGuru Prasad100% (1)
- Tetfund Conf. Nomination FormDocument1 pageTetfund Conf. Nomination FormValentine AguNo ratings yet
- Tetfund Conference Nomination FormDocument1 pageTetfund Conference Nomination FormOkulaja OLAWALE KEHINDE100% (4)
- Caper Form EmptyDocument9 pagesCaper Form Emptysimeon.badruNo ratings yet
- Assignment Application Letter (Part 1) PDFDocument3 pagesAssignment Application Letter (Part 1) PDFEricIswanNo ratings yet
- Instructor Edition: Do Not DuplicateDocument66 pagesInstructor Edition: Do Not DuplicateSanjay BhattacharyaNo ratings yet
- Confidential: Position Applied For: Salary ExpectedDocument4 pagesConfidential: Position Applied For: Salary ExpectedRichard ZhemiNo ratings yet
- F4 BST PP1 Et3 QNDocument7 pagesF4 BST PP1 Et3 QNrnyaboke90No ratings yet
- CoachingDocument87 pagesCoachingTimsy Dhingra100% (4)
- Form 8Document3 pagesForm 8idahmarvelous58No ratings yet
- Unit 8 Presentation Skills: 8.0 ObjectivesDocument13 pagesUnit 8 Presentation Skills: 8.0 ObjectivesMD shah KhanNo ratings yet
- GEMBA WALK (For Monitoring) CHECKLISTDocument1 pageGEMBA WALK (For Monitoring) CHECKLISTChandu PanditNo ratings yet
- QuestionnaireDocument4 pagesQuestionnaireClifford OwusuNo ratings yet
- 938 Aurora BLVD., Cubao, Quezon City: Technological Institute of The PhilippinesDocument104 pages938 Aurora BLVD., Cubao, Quezon City: Technological Institute of The PhilippinesKingwinston OmbionNo ratings yet
- 2014 S Assessment SheetDocument4 pages2014 S Assessment SheetTijjani BelloNo ratings yet
- 2000-1218 Midterm ExamDocument3 pages2000-1218 Midterm ExamTimoy AlinabonNo ratings yet
- Standards Association of Zimbabwe Iso 9001:2015 Qms Certification QuestionnaireDocument2 pagesStandards Association of Zimbabwe Iso 9001:2015 Qms Certification QuestionnaireTakudzwa Calvin ChibudaNo ratings yet
- Of WLBDocument6 pagesOf WLBPunnya SelvarajNo ratings yet
- Cre QS Midterm 1 ExamsDocument5 pagesCre QS Midterm 1 ExamsmndiwaNo ratings yet
- DEK Training Needs Analysis TemplateDocument2 pagesDEK Training Needs Analysis Templatenogarap767No ratings yet
- Third PageDocument2 pagesThird Pageleirkin33No ratings yet
- Employer EvalFormDocument4 pagesEmployer EvalFormAlma Jean SubongNo ratings yet
- On-The Job Training at Commission On Filipinos OverseasDocument3 pagesOn-The Job Training at Commission On Filipinos OverseasEsmeralda KevinNo ratings yet
- Series 4 BSST pp1-2 CombinedDocument16 pagesSeries 4 BSST pp1-2 CombinedJulius KimaniNo ratings yet
- Sample Format Non Thesis 3Document16 pagesSample Format Non Thesis 3Jamie HaravataNo ratings yet
- LGSC Form7aDocument6 pagesLGSC Form7aVom Samourais0% (1)
- ITF Form8Document2 pagesITF Form8Imrana SirajoNo ratings yet
- Final Report - University of Pittsburgh Academic Study On Gender-Integrated Recruit TrainingDocument738 pagesFinal Report - University of Pittsburgh Academic Study On Gender-Integrated Recruit TrainingZachary RogersNo ratings yet
- JeDocument1 pageJeReyes Je AnNo ratings yet
- Appointment of Academic CounsellorsDocument5 pagesAppointment of Academic CounsellorsM.M.NaqshbandiNo ratings yet
- Exit Survey TemplateDocument5 pagesExit Survey TemplateFarhan SaghirNo ratings yet
- Umfolozi Municipality Application For Employment: 1. Personal (Block Letters)Document2 pagesUmfolozi Municipality Application For Employment: 1. Personal (Block Letters)ZandileNo ratings yet
- Annexure 2Document1 pageAnnexure 2LynchXdNo ratings yet
- Questionnaire MDocument4 pagesQuestionnaire MSubhasisChatterjeeNo ratings yet
- Breakthrough Improvement with QI Macros and Excel: Finding the Invisible Low-Hanging Fruit: Finding the Invisible Low-Hanging FruitFrom EverandBreakthrough Improvement with QI Macros and Excel: Finding the Invisible Low-Hanging Fruit: Finding the Invisible Low-Hanging FruitNo ratings yet
- Nailing Jelly to the Wall: Defining and Providing Technical Assistance in Early Childhood EducationFrom EverandNailing Jelly to the Wall: Defining and Providing Technical Assistance in Early Childhood EducationRating: 5 out of 5 stars5/5 (1)
- Instructional PlanningDocument12 pagesInstructional PlanningMissy FelimonNo ratings yet
- SSC Form 2Document3 pagesSSC Form 2Raymart NaagNo ratings yet
- JFUST - Volume 14 - Issue 3 - Pages 1-57Document57 pagesJFUST - Volume 14 - Issue 3 - Pages 1-57noha alsaidNo ratings yet
- Elective - EssayDocument2 pagesElective - EssayRicell Joy RocamoraNo ratings yet
- Weekly Home Learning Plan Science 8 Quarter 4, Week 4, June 28-July 2, 2021Document3 pagesWeekly Home Learning Plan Science 8 Quarter 4, Week 4, June 28-July 2, 2021kaycin Duzon100% (1)
- B.A. (H) Pol. ScienceDocument13 pagesB.A. (H) Pol. ScienceTarun SharmaNo ratings yet
- Uhv-3 (Values, Relationship & Ethical Human Conduct-For A Happy & Harmonious Society)Document1 pageUhv-3 (Values, Relationship & Ethical Human Conduct-For A Happy & Harmonious Society)Vivek guptaNo ratings yet
- English Language A: Pearson Edexcel International GCSEDocument28 pagesEnglish Language A: Pearson Edexcel International GCSEFayez AhmedNo ratings yet
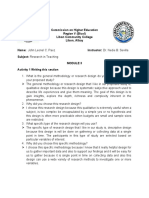
- Research Module 3Document5 pagesResearch Module 3Benilda Pensica SevillaNo ratings yet
- Walk in Interview Ryonan Electric India PVT LimitedDocument2 pagesWalk in Interview Ryonan Electric India PVT Limitedyisakabera123No ratings yet
- Primary Pricelist 1 Oct 2021 RtgsDocument11 pagesPrimary Pricelist 1 Oct 2021 RtgsKundai NyaguraNo ratings yet
- Database For Makeni GraduatesDocument194 pagesDatabase For Makeni GraduatesSelemani DinalaNo ratings yet
- English (Option B), Junior Cycle - Higher Level - PaperDocument37 pagesEnglish (Option B), Junior Cycle - Higher Level - PaperMediaNo ratings yet
- Program Outcomes and Student Learning OutcomesDocument23 pagesProgram Outcomes and Student Learning OutcomesRuby Aiza PascuaNo ratings yet
- Mini - Project - Second - Year Report FormatDocument8 pagesMini - Project - Second - Year Report FormatBrijesh Yadav0% (1)
- Mathematics: Quarter 1 - Module 2: Whole Numbers Up To 100 000Document20 pagesMathematics: Quarter 1 - Module 2: Whole Numbers Up To 100 000Jobelle Canlas100% (1)
- MQ Mop-Up Notification MBBS Course 2021Document3 pagesMQ Mop-Up Notification MBBS Course 2021Feroz FerozNo ratings yet
- School Program ScoutsDocument2 pagesSchool Program ScoutsEd LynNo ratings yet
- Nsbi 2019 Template For Validation (Secondary) : District: AYUNGON 1Document34 pagesNsbi 2019 Template For Validation (Secondary) : District: AYUNGON 1Ghlends Alarcio GomezNo ratings yet
- Ead 530 - Field Experience BDocument5 pagesEad 530 - Field Experience Bapi-535950120No ratings yet
- Castillo Carl Louie E. - Midterm Learning GuideDocument2 pagesCastillo Carl Louie E. - Midterm Learning GuideDevon2 CastilloNo ratings yet
- Cheyanne Geiger: Cgeige2@students - Towson.eduDocument2 pagesCheyanne Geiger: Cgeige2@students - Towson.eduapi-512276583No ratings yet
- DLL OutputDocument4 pagesDLL OutputLindsey ArrabisNo ratings yet
- Pat B Inggris Kelas 8Document4 pagesPat B Inggris Kelas 8Putri Nur AzizahNo ratings yet
- #1 Active Research QuestionsDocument6 pages#1 Active Research QuestionsGabriela GNo ratings yet
- Skill Acquisition Worksheet AnswersDocument2 pagesSkill Acquisition Worksheet Answers愛.NiniNo ratings yet
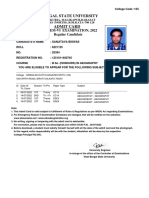
- West Bengal State University: CBCS, Sem-Vi Examination, 2022 Regular CandidateDocument1 pageWest Bengal State University: CBCS, Sem-Vi Examination, 2022 Regular CandidateSANJITAVA BISWASNo ratings yet
- 3.3.2. Sample Certification For Head of TVI With Other Designation (Non-Teaching Staff)Document7 pages3.3.2. Sample Certification For Head of TVI With Other Designation (Non-Teaching Staff)robelyn veranoNo ratings yet
- Facilitation Learning Plan - Sample and TemplateDocument4 pagesFacilitation Learning Plan - Sample and Templatenica gargaritaNo ratings yet
- 2017 FILG8Q1 UnlockedDocument254 pages2017 FILG8Q1 UnlockedJuvilyn ChanNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- 5 DVP Assignment CIPD Level 5Document31 pages5 DVP Assignment CIPD Level 5Nomadiclahas Vagabond टीटो89% (54)
- HR Training and Development QuestionnaireDocument5 pagesHR Training and Development QuestionnaireAnis Tajuldin100% (3)
- Training Impact Assessment QuestionnaireDocument6 pagesTraining Impact Assessment QuestionnaireRuby Garcia50% (6)
- The Ultimate Guide To Job Interview Answers1Document92 pagesThe Ultimate Guide To Job Interview Answers1Oana Si Cristi Mocanu86% (7)
- Complete Audio Mastering: Practical TechniquesFrom EverandComplete Audio Mastering: Practical TechniquesRating: 5 out of 5 stars5/5 (5)
- Appendix I Interview Guide For TANESCO Magomeni Zone EmployeesDocument4 pagesAppendix I Interview Guide For TANESCO Magomeni Zone EmployeesSadelick KihongosiNo ratings yet
- Appendix (2) The Close-Ended Questions, Which Are Asked To The TraineesDocument4 pagesAppendix (2) The Close-Ended Questions, Which Are Asked To The TraineesAsadulla KhanNo ratings yet
- May 2018 Unmeb Examination Centre Accreditation ToolDocument26 pagesMay 2018 Unmeb Examination Centre Accreditation Toolopioamos260No ratings yet
- Course Assessment Form Date .. . Course Title: . Facilitator: Location: .. 1Document1 pageCourse Assessment Form Date .. . Course Title: . Facilitator: Location: .. 1Rony LesbtNo ratings yet
- HR Training and Development QuestionnaireDocument4 pagesHR Training and Development QuestionnaireShariful Islam Shaheen100% (3)
- Kingsway-Application Form, Teacher-22Document7 pagesKingsway-Application Form, Teacher-22anon-719393No ratings yet
- Exam Final S 8Document5 pagesExam Final S 8Salma A.No ratings yet
- Summer Internship Feedback DCEA, GLA UnivDocument2 pagesSummer Internship Feedback DCEA, GLA UnivMANSI SINHANo ratings yet
- Nysc National Directorate HeadquartersDocument4 pagesNysc National Directorate HeadquartersABDULRAHMAN YAHAYA (SIR-AB)No ratings yet
- Apr ViDocument4 pagesApr ViITI JammuNo ratings yet
- How Can You Assess The Effectiveness of Training and Development of Your Organization?Document11 pagesHow Can You Assess The Effectiveness of Training and Development of Your Organization?bonyNo ratings yet
- EDI National Master Trainer Success Story Collection Form V2 As of Dec 31, 2024 FinalDocument4 pagesEDI National Master Trainer Success Story Collection Form V2 As of Dec 31, 2024 FinalYonatan BizuworkNo ratings yet
- Ace Credit - Tesol For BusinessDocument176 pagesAce Credit - Tesol For Businessmilo060712No ratings yet
- Industrial Training Fund: Students Industrial Work Experience Scheme End of Year Programreport SheetDocument2 pagesIndustrial Training Fund: Students Industrial Work Experience Scheme End of Year Programreport Sheetjessica Emmanuel100% (1)
- QuestionnaireDocument3 pagesQuestionnaireKASHIF NAWAZNo ratings yet
- Application Form PDFDocument3 pagesApplication Form PDFmthabisi nyathiNo ratings yet
- Questionnaire On Information About HRD in TelecommunicationDocument8 pagesQuestionnaire On Information About HRD in Telecommunicationway2pritiNo ratings yet
- PSC Job Application Form 1J - SRC (1) (1)Document10 pagesPSC Job Application Form 1J - SRC (1) (1)Mercy Chepkorir KilisioNo ratings yet
- Section A: Respondents BackgroundDocument2 pagesSection A: Respondents BackgroundOoi See ChongNo ratings yet
- Annual Confidential Report of The Work and Conduct of Teachers of Aided/Unaided Recognised SchoolsDocument7 pagesAnnual Confidential Report of The Work and Conduct of Teachers of Aided/Unaided Recognised SchoolsGuru Prasad100% (1)
- Tetfund Conf. Nomination FormDocument1 pageTetfund Conf. Nomination FormValentine AguNo ratings yet
- Tetfund Conference Nomination FormDocument1 pageTetfund Conference Nomination FormOkulaja OLAWALE KEHINDE100% (4)
- Caper Form EmptyDocument9 pagesCaper Form Emptysimeon.badruNo ratings yet
- Assignment Application Letter (Part 1) PDFDocument3 pagesAssignment Application Letter (Part 1) PDFEricIswanNo ratings yet
- Instructor Edition: Do Not DuplicateDocument66 pagesInstructor Edition: Do Not DuplicateSanjay BhattacharyaNo ratings yet
- Confidential: Position Applied For: Salary ExpectedDocument4 pagesConfidential: Position Applied For: Salary ExpectedRichard ZhemiNo ratings yet
- F4 BST PP1 Et3 QNDocument7 pagesF4 BST PP1 Et3 QNrnyaboke90No ratings yet
- CoachingDocument87 pagesCoachingTimsy Dhingra100% (4)
- Form 8Document3 pagesForm 8idahmarvelous58No ratings yet
- Unit 8 Presentation Skills: 8.0 ObjectivesDocument13 pagesUnit 8 Presentation Skills: 8.0 ObjectivesMD shah KhanNo ratings yet
- GEMBA WALK (For Monitoring) CHECKLISTDocument1 pageGEMBA WALK (For Monitoring) CHECKLISTChandu PanditNo ratings yet
- QuestionnaireDocument4 pagesQuestionnaireClifford OwusuNo ratings yet
- 938 Aurora BLVD., Cubao, Quezon City: Technological Institute of The PhilippinesDocument104 pages938 Aurora BLVD., Cubao, Quezon City: Technological Institute of The PhilippinesKingwinston OmbionNo ratings yet
- 2014 S Assessment SheetDocument4 pages2014 S Assessment SheetTijjani BelloNo ratings yet
- 2000-1218 Midterm ExamDocument3 pages2000-1218 Midterm ExamTimoy AlinabonNo ratings yet
- Standards Association of Zimbabwe Iso 9001:2015 Qms Certification QuestionnaireDocument2 pagesStandards Association of Zimbabwe Iso 9001:2015 Qms Certification QuestionnaireTakudzwa Calvin ChibudaNo ratings yet
- Of WLBDocument6 pagesOf WLBPunnya SelvarajNo ratings yet
- Cre QS Midterm 1 ExamsDocument5 pagesCre QS Midterm 1 ExamsmndiwaNo ratings yet
- DEK Training Needs Analysis TemplateDocument2 pagesDEK Training Needs Analysis Templatenogarap767No ratings yet
- Third PageDocument2 pagesThird Pageleirkin33No ratings yet
- Employer EvalFormDocument4 pagesEmployer EvalFormAlma Jean SubongNo ratings yet
- On-The Job Training at Commission On Filipinos OverseasDocument3 pagesOn-The Job Training at Commission On Filipinos OverseasEsmeralda KevinNo ratings yet
- Series 4 BSST pp1-2 CombinedDocument16 pagesSeries 4 BSST pp1-2 CombinedJulius KimaniNo ratings yet
- Sample Format Non Thesis 3Document16 pagesSample Format Non Thesis 3Jamie HaravataNo ratings yet
- LGSC Form7aDocument6 pagesLGSC Form7aVom Samourais0% (1)
- ITF Form8Document2 pagesITF Form8Imrana SirajoNo ratings yet
- Final Report - University of Pittsburgh Academic Study On Gender-Integrated Recruit TrainingDocument738 pagesFinal Report - University of Pittsburgh Academic Study On Gender-Integrated Recruit TrainingZachary RogersNo ratings yet
- JeDocument1 pageJeReyes Je AnNo ratings yet
- Appointment of Academic CounsellorsDocument5 pagesAppointment of Academic CounsellorsM.M.NaqshbandiNo ratings yet
- Exit Survey TemplateDocument5 pagesExit Survey TemplateFarhan SaghirNo ratings yet
- Umfolozi Municipality Application For Employment: 1. Personal (Block Letters)Document2 pagesUmfolozi Municipality Application For Employment: 1. Personal (Block Letters)ZandileNo ratings yet
- Annexure 2Document1 pageAnnexure 2LynchXdNo ratings yet
- Questionnaire MDocument4 pagesQuestionnaire MSubhasisChatterjeeNo ratings yet
- Breakthrough Improvement with QI Macros and Excel: Finding the Invisible Low-Hanging Fruit: Finding the Invisible Low-Hanging FruitFrom EverandBreakthrough Improvement with QI Macros and Excel: Finding the Invisible Low-Hanging Fruit: Finding the Invisible Low-Hanging FruitNo ratings yet
- Nailing Jelly to the Wall: Defining and Providing Technical Assistance in Early Childhood EducationFrom EverandNailing Jelly to the Wall: Defining and Providing Technical Assistance in Early Childhood EducationRating: 5 out of 5 stars5/5 (1)
- Instructional PlanningDocument12 pagesInstructional PlanningMissy FelimonNo ratings yet
- SSC Form 2Document3 pagesSSC Form 2Raymart NaagNo ratings yet
- JFUST - Volume 14 - Issue 3 - Pages 1-57Document57 pagesJFUST - Volume 14 - Issue 3 - Pages 1-57noha alsaidNo ratings yet
- Elective - EssayDocument2 pagesElective - EssayRicell Joy RocamoraNo ratings yet
- Weekly Home Learning Plan Science 8 Quarter 4, Week 4, June 28-July 2, 2021Document3 pagesWeekly Home Learning Plan Science 8 Quarter 4, Week 4, June 28-July 2, 2021kaycin Duzon100% (1)
- B.A. (H) Pol. ScienceDocument13 pagesB.A. (H) Pol. ScienceTarun SharmaNo ratings yet
- Uhv-3 (Values, Relationship & Ethical Human Conduct-For A Happy & Harmonious Society)Document1 pageUhv-3 (Values, Relationship & Ethical Human Conduct-For A Happy & Harmonious Society)Vivek guptaNo ratings yet
- English Language A: Pearson Edexcel International GCSEDocument28 pagesEnglish Language A: Pearson Edexcel International GCSEFayez AhmedNo ratings yet
- Research Module 3Document5 pagesResearch Module 3Benilda Pensica SevillaNo ratings yet
- Walk in Interview Ryonan Electric India PVT LimitedDocument2 pagesWalk in Interview Ryonan Electric India PVT Limitedyisakabera123No ratings yet
- Primary Pricelist 1 Oct 2021 RtgsDocument11 pagesPrimary Pricelist 1 Oct 2021 RtgsKundai NyaguraNo ratings yet
- Database For Makeni GraduatesDocument194 pagesDatabase For Makeni GraduatesSelemani DinalaNo ratings yet
- English (Option B), Junior Cycle - Higher Level - PaperDocument37 pagesEnglish (Option B), Junior Cycle - Higher Level - PaperMediaNo ratings yet
- Program Outcomes and Student Learning OutcomesDocument23 pagesProgram Outcomes and Student Learning OutcomesRuby Aiza PascuaNo ratings yet
- Mini - Project - Second - Year Report FormatDocument8 pagesMini - Project - Second - Year Report FormatBrijesh Yadav0% (1)
- Mathematics: Quarter 1 - Module 2: Whole Numbers Up To 100 000Document20 pagesMathematics: Quarter 1 - Module 2: Whole Numbers Up To 100 000Jobelle Canlas100% (1)
- MQ Mop-Up Notification MBBS Course 2021Document3 pagesMQ Mop-Up Notification MBBS Course 2021Feroz FerozNo ratings yet
- School Program ScoutsDocument2 pagesSchool Program ScoutsEd LynNo ratings yet
- Nsbi 2019 Template For Validation (Secondary) : District: AYUNGON 1Document34 pagesNsbi 2019 Template For Validation (Secondary) : District: AYUNGON 1Ghlends Alarcio GomezNo ratings yet
- Ead 530 - Field Experience BDocument5 pagesEad 530 - Field Experience Bapi-535950120No ratings yet
- Castillo Carl Louie E. - Midterm Learning GuideDocument2 pagesCastillo Carl Louie E. - Midterm Learning GuideDevon2 CastilloNo ratings yet
- Cheyanne Geiger: Cgeige2@students - Towson.eduDocument2 pagesCheyanne Geiger: Cgeige2@students - Towson.eduapi-512276583No ratings yet
- DLL OutputDocument4 pagesDLL OutputLindsey ArrabisNo ratings yet
- Pat B Inggris Kelas 8Document4 pagesPat B Inggris Kelas 8Putri Nur AzizahNo ratings yet
- #1 Active Research QuestionsDocument6 pages#1 Active Research QuestionsGabriela GNo ratings yet
- Skill Acquisition Worksheet AnswersDocument2 pagesSkill Acquisition Worksheet Answers愛.NiniNo ratings yet
- West Bengal State University: CBCS, Sem-Vi Examination, 2022 Regular CandidateDocument1 pageWest Bengal State University: CBCS, Sem-Vi Examination, 2022 Regular CandidateSANJITAVA BISWASNo ratings yet
- 3.3.2. Sample Certification For Head of TVI With Other Designation (Non-Teaching Staff)Document7 pages3.3.2. Sample Certification For Head of TVI With Other Designation (Non-Teaching Staff)robelyn veranoNo ratings yet
- Facilitation Learning Plan - Sample and TemplateDocument4 pagesFacilitation Learning Plan - Sample and Templatenica gargaritaNo ratings yet
- 2017 FILG8Q1 UnlockedDocument254 pages2017 FILG8Q1 UnlockedJuvilyn ChanNo ratings yet