Download as pdf or txt
You might also like
- 11 Digital Smile DesignDocument10 pages11 Digital Smile DesignSilvia KriNo ratings yet
- Clinical Practicum PaperDocument26 pagesClinical Practicum Paperncory79100% (1)
- Summary Revising Prose PDFDocument19 pagesSummary Revising Prose PDFDavid LópezNo ratings yet
- Miller v. AlabamaDocument62 pagesMiller v. AlabamaDoug MataconisNo ratings yet
- Lawvere F W Functorial Semantics of Algebraic Theories PHD Thesis 1963Document122 pagesLawvere F W Functorial Semantics of Algebraic Theories PHD Thesis 1963LBrouwerNo ratings yet
- Calculator For Stiffness and Compliance of Lamina 90Document3 pagesCalculator For Stiffness and Compliance of Lamina 90panbuuNo ratings yet
- Retrieve (1 4)Document4 pagesRetrieve (1 4)Travis HarveyNo ratings yet
- J Esthet Restor Dent - 2022 - CoachmanDocument7 pagesJ Esthet Restor Dent - 2022 - Coachmanbruno mañonNo ratings yet
- Journal of Prosthodontics - 2022 - PapaspyridakosDocument6 pagesJournal of Prosthodontics - 2022 - Papaspyridakos6mp57dy74sNo ratings yet
- CoachmanDocument10 pagesCoachman881971100% (3)
- Digital Smile Design: A Tool For Treatment Planning and Communication in Esthetic DentistryDocument10 pagesDigital Smile Design: A Tool For Treatment Planning and Communication in Esthetic Dentistrygilberto69No ratings yet
- Digital Wax Up in DentistryDocument14 pagesDigital Wax Up in Dentistrybanea costin100% (1)
- Coachman Calamita DSD Eng 12 PDFDocument10 pagesCoachman Calamita DSD Eng 12 PDFÁngela María GuevaraNo ratings yet
- Which Clinical and Laboratory Procedures Should Be Used To Fabricate Digital Complete Dentures? A Systematic ReviewDocument17 pagesWhich Clinical and Laboratory Procedures Should Be Used To Fabricate Digital Complete Dentures? A Systematic ReviewCaroline AngoneseNo ratings yet
- Digitally Enhanced Esthetic DentistryDocument3 pagesDigitally Enhanced Esthetic DentistrySMART SMARNo ratings yet
- Cad CamDocument18 pagesCad CamTeffy CasteloNo ratings yet
- Poster Strisca StanislavDocument1 pagePoster Strisca StanislavStanislav StrîșcaNo ratings yet
- The Effect of Digital Diagnostic Setups On Orthodontic Treatment PlanningDocument8 pagesThe Effect of Digital Diagnostic Setups On Orthodontic Treatment PlanningAlejandro Aranzábal NavarreteNo ratings yet
- DrChristianCoachman (1 2)Document2 pagesDrChristianCoachman (1 2)Javi ChavezNo ratings yet
- 2016 JOO Camardella PDFDocument11 pages2016 JOO Camardella PDFSelvaNo ratings yet
- Journal of Prosthodontics - 2020 - Park - Digitally Created 3 Piece Additive Manufactured Index For Direct EstheticDocument7 pagesJournal of Prosthodontics - 2020 - Park - Digitally Created 3 Piece Additive Manufactured Index For Direct Estheticfernando vicenteNo ratings yet
- J of Oral Rehabilitation - 2017 - Jokstad - Computer Assisted Technologies Used in Oral Rehabilitation and The ClinicalDocument30 pagesJ of Oral Rehabilitation - 2017 - Jokstad - Computer Assisted Technologies Used in Oral Rehabilitation and The ClinicalJorge AlvaradoNo ratings yet
- Digital Dental Implantology: From Treatment Planning to Guided SurgeryFrom EverandDigital Dental Implantology: From Treatment Planning to Guided SurgeryJorge M. GalanteNo ratings yet
- Marlière Et Al. 2018 ProsthodonticsDocument8 pagesMarlière Et Al. 2018 ProsthodonticsApril FloresNo ratings yet
- Interdisciplinary Treat Planning ChapterDocument56 pagesInterdisciplinary Treat Planning ChapterJulio César Huayllasco de la Cruz0% (1)
- Studiu de CazDocument3 pagesStudiu de CazNico LucaciNo ratings yet
- Alternative Treatment To Orthognatic Surgery by The Application of Digital Smile PlanningDocument12 pagesAlternative Treatment To Orthognatic Surgery by The Application of Digital Smile PlanningCentro Dental IntegralNo ratings yet
- Essay "Is The Surgeon Redundant in The Age of Dental Planning and Workflow"Document24 pagesEssay "Is The Surgeon Redundant in The Age of Dental Planning and Workflow"Gabriel RodriguezNo ratings yet
- CBCT Ch.7 DCNADocument30 pagesCBCT Ch.7 DCNAgibsonNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFDANIELA ALEJANDRA DELGADO FONSECANo ratings yet
- Healthcare 11 00679 v2Document15 pagesHealthcare 11 00679 v2KEY 1111No ratings yet
- Yang 2018Document6 pagesYang 2018Krushil BhadaniNo ratings yet
- Digital Diagnostics and Orthodontic PracticeDocument6 pagesDigital Diagnostics and Orthodontic PracticeXimena De LeonNo ratings yet
- Digital Dentistry and Its Impact On Oral Health-Related QualDocument10 pagesDigital Dentistry and Its Impact On Oral Health-Related Qualbelen.rodasNo ratings yet
- Video Cephalometric Diagnosis (VCD) : A New Concept in Treatment Planning?Document17 pagesVideo Cephalometric Diagnosis (VCD) : A New Concept in Treatment Planning?Ismail BenameurNo ratings yet
- Guided Surgery in Dental ImplantologyDocument5 pagesGuided Surgery in Dental Implantologynarendra singhNo ratings yet
- Digital vs. Conventional ImplantDocument6 pagesDigital vs. Conventional ImplantCaroline AngoneseNo ratings yet
- DSD From 2d To 3dDocument14 pagesDSD From 2d To 3dHugoRoCkstar100% (1)
- Digital WorkflowsDocument14 pagesDigital Workflowsmoji_puiNo ratings yet
- Using A Clinical Protocol For Orthognathic Surgery and Assessing A 3-Dimensional Virtual ApproachDocument15 pagesUsing A Clinical Protocol For Orthognathic Surgery and Assessing A 3-Dimensional Virtual ApproachKorkmaz SayınsuNo ratings yet
- Alejandro Lanis Full Mouth Oral Rehabilitation of ADocument13 pagesAlejandro Lanis Full Mouth Oral Rehabilitation of AAARON DIAZ RONQUILLONo ratings yet
- Digitalized ProsthodonticsDocument3 pagesDigitalized ProsthodonticsSg100% (1)
- An Ontology-Driven, Case-Based Clinical Decision Support Model For Removable Partial Denture DesignDocument8 pagesAn Ontology-Driven, Case-Based Clinical Decision Support Model For Removable Partial Denture Designteodor888No ratings yet
- Jurnal PutriDocument20 pagesJurnal Putriputriind-ahps0% (1)
- Comparison of The Accuracy of Optical Impression Systems in Three Different Clinical SituationsDocument8 pagesComparison of The Accuracy of Optical Impression Systems in Three Different Clinical SituationsMathias SchottNo ratings yet
- MDA APR2012 Fasbinder Article R 031212Document9 pagesMDA APR2012 Fasbinder Article R 031212labakoum badr-eddineNo ratings yet
- Polymers: Dental 3D-Printing: Transferring Art From The Laboratories To The ClinicsDocument25 pagesPolymers: Dental 3D-Printing: Transferring Art From The Laboratories To The ClinicssmilesindiaNo ratings yet
- Evaluation of Patient Experience and Satisfaction With CAD CAM Fabricated Complete Dentures A Retrospective Survey StudyDocument5 pagesEvaluation of Patient Experience and Satisfaction With CAD CAM Fabricated Complete Dentures A Retrospective Survey StudygermanpuigNo ratings yet
- The Digital Smile Design Concept: Documenting, Designing, and Communicating in Interdisciplinary DentistryDocument35 pagesThe Digital Smile Design Concept: Documenting, Designing, and Communicating in Interdisciplinary DentistryHải Việt CaoNo ratings yet
- Digital Orthodontics - A Contemporary View of Futuristic PracticeDocument10 pagesDigital Orthodontics - A Contemporary View of Futuristic PracticeIJAR JOURNALNo ratings yet
- Comparison of Different Impression Techniques ForDocument8 pagesComparison of Different Impression Techniques ForQabas MustafaNo ratings yet
- The Aesthetic Smile Designing in The Digital Dentistry EraDocument3 pagesThe Aesthetic Smile Designing in The Digital Dentistry EraLucia PopescuNo ratings yet
- Clinical Efficiency and Patient Preference of Digital and Conventional Workflow For Single Implant Crowns Using Immediate and Regular Digital Impression A Meta-AnalysisDocument18 pagesClinical Efficiency and Patient Preference of Digital and Conventional Workflow For Single Implant Crowns Using Immediate and Regular Digital Impression A Meta-AnalysisCaroline AngoneseNo ratings yet
- Digital White Paper r1Document11 pagesDigital White Paper r1Syed AbeerNo ratings yet
- Joda 2016Document6 pagesJoda 2016Juan MusanNo ratings yet
- Digital Versus Conventional Impression Method in Children: Comfort, Preference and TimeDocument8 pagesDigital Versus Conventional Impression Method in Children: Comfort, Preference and Timemadhu kakanurNo ratings yet
- Digital Versus Conventional Impression Method in Children: Comfort, Preference and TimeDocument8 pagesDigital Versus Conventional Impression Method in Children: Comfort, Preference and Timemadhu kakanurNo ratings yet
- Machine Learning in DentistryFrom EverandMachine Learning in DentistryChing-Chang KoNo ratings yet
- Suresh2022 PDFDocument8 pagesSuresh2022 PDFFilipe do Carmo Barreto DiasNo ratings yet
- 10 1016@j Prosdent 2018 10 012Document5 pages10 1016@j Prosdent 2018 10 012a.alnajei96No ratings yet
- Digital Versus Conventional Impression Method in Children: Comfort, Preference and TimeDocument18 pagesDigital Versus Conventional Impression Method in Children: Comfort, Preference and TimeSome TimeNo ratings yet
- Available CAD-CAM System Concepts For The Fabrication of Digital DenturesDocument9 pagesAvailable CAD-CAM System Concepts For The Fabrication of Digital DenturesSMART SMARNo ratings yet
- Paper14 PDFDocument5 pagesPaper14 PDFCarlos Alfredo Finquin PejerreyNo ratings yet
- Buap 6Document11 pagesBuap 6WawawaNo ratings yet
- Project For LMSDocument7 pagesProject For LMSTHUY PHAM NGOCNo ratings yet
- Istorijat DresstaDocument4 pagesIstorijat DresstaAmdMsiNo ratings yet
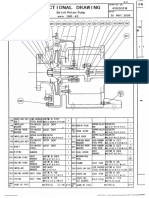
- Dring Water Pump Model BHR-40 M C 08Document2 pagesDring Water Pump Model BHR-40 M C 08Nam Nguyen HuuNo ratings yet
- Final Report SubmisionDocument53 pagesFinal Report SubmisionGaurav TrivediNo ratings yet
- Q2 Tle Reviewer PDFDocument6 pagesQ2 Tle Reviewer PDFFire RobloxNo ratings yet
- Regulatory Notice For Wireless Lan Modules Consumer NB V5Document114 pagesRegulatory Notice For Wireless Lan Modules Consumer NB V5djmorphyNo ratings yet
- Breunig Karl LiebknechtDocument12 pagesBreunig Karl Liebknechtluis enrique mendezNo ratings yet
- Tezuka Animation Vol 1 PDFDocument84 pagesTezuka Animation Vol 1 PDFMauricio Matus100% (4)
- Sweet Oddity Art: Angus The Highland Cow Crochet Pattern Extension OnlyDocument8 pagesSweet Oddity Art: Angus The Highland Cow Crochet Pattern Extension OnlyIilia Buenrostro100% (4)
- Sabine Pass Approval Order, DOEDocument50 pagesSabine Pass Approval Order, DOEcprofitaNo ratings yet
- Government Polytechnic, Uttawar: (D.Pharma)Document2 pagesGovernment Polytechnic, Uttawar: (D.Pharma)Mujahid SehrawatNo ratings yet
- Lecture-12 Practice-3Document5 pagesLecture-12 Practice-3Muhammad ZainNo ratings yet
- CILADocument8 pagesCILA23985811No ratings yet
- 2019 CLC 211Document6 pages2019 CLC 211Asif NawazNo ratings yet
- (En) The Ultimative Guide by FishyDocument72 pages(En) The Ultimative Guide by FishytoplvlNo ratings yet
- Anito Elementary SchoolDocument4 pagesAnito Elementary SchoolKristina CalvoNo ratings yet
- TCRA Communications Statistics For Q3 2023-2024 - 1713708695Document50 pagesTCRA Communications Statistics For Q3 2023-2024 - 1713708695Amir Aboul FotouhNo ratings yet
- Shiva AyyaduraiDocument60 pagesShiva AyyaduraiJoy Velu100% (2)
- Personal Development: Quarter 1-Module 3 Week 3&4Document12 pagesPersonal Development: Quarter 1-Module 3 Week 3&4Nikka Irah CamaristaNo ratings yet
- 03 Industrial RevolutionDocument103 pages03 Industrial Revolutioninfo12060% (1)
- CRM Assignment 2Document11 pagesCRM Assignment 2Arneet SarnaNo ratings yet
- Star Wars: Building A Galaxy With Code: Lesson OverviewDocument4 pagesStar Wars: Building A Galaxy With Code: Lesson Overviewmaslinovik5003No ratings yet
- Course Modules - IT Systems Management 1 HISM100-1Document8 pagesCourse Modules - IT Systems Management 1 HISM100-1Bonginkosi0% (1)
- Slokas and Mantras: Bhaja Govindam Was Written by Jagadguru Adi ShankaracharyaDocument12 pagesSlokas and Mantras: Bhaja Govindam Was Written by Jagadguru Adi Shankaracharyan.devanathanNo ratings yet
- Abonesh Tesfaye Agri. Economics - Jan. 2007Document246 pagesAbonesh Tesfaye Agri. Economics - Jan. 2007Rafez JoneNo ratings yet
- Turbo Generator PDFDocument5 pagesTurbo Generator PDFAlfeusShalonda100% (1)