Download as docx, pdf, or txt
You might also like
- Hemodialysis Patient's Endorsement FormDocument1 pageHemodialysis Patient's Endorsement FormHacienda Galea Resort and Events Place100% (1)
- Nationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyDocument1 pageNationwide Health Systems Baguio, Inc: Please Fill Up Dotted Boxed Area OnlyNorma Arquillo100% (1)
- Stroke Form: Patient DataDocument6 pagesStroke Form: Patient DataErikaMRSiaNo ratings yet
- Kci Vac Therapy Vtiaf UpdatedDocument2 pagesKci Vac Therapy Vtiaf UpdatedHi BeyoNo ratings yet
- Laboratory and Blood Bank Surveillance (Labs) Form 1: Epidemiology BureauDocument1 pageLaboratory and Blood Bank Surveillance (Labs) Form 1: Epidemiology BureauEvo SingsonNo ratings yet
- A Healthy World Starts Here: Nwdi Requirements For Sars Cov-2 (Covid-19) Antibody Rapid Diagnostic TestDocument2 pagesA Healthy World Starts Here: Nwdi Requirements For Sars Cov-2 (Covid-19) Antibody Rapid Diagnostic TestEric NagumNo ratings yet
- CAUTI RCA FormDocument2 pagesCAUTI RCA Formprincesatish2004No ratings yet
- Medical Disbursement Monitoring FormDocument2 pagesMedical Disbursement Monitoring Formgenalcantara83No ratings yet
- Daily Assessment Chart ICUDocument16 pagesDaily Assessment Chart ICUaiman abushahmaNo ratings yet
- 8.) Health-and-Medical-Profile Template Ver.2Document4 pages8.) Health-and-Medical-Profile Template Ver.2SocialWelfare SilangNo ratings yet
- UTI AssessmentDocument2 pagesUTI Assessmentkhangsiean89No ratings yet
- Medical FormsDocument5 pagesMedical FormsolandiolettyNo ratings yet
- Pages 5 Form FDocument2 pagesPages 5 Form FANIL KUMARNo ratings yet
- PA Tool A UpdatedDocument19 pagesPA Tool A UpdatedSweetyfe GabatanNo ratings yet
- FP Form1 V3.0 2016Document3 pagesFP Form1 V3.0 2016Lorenz Joey Ricarte100% (2)
- FORMF2014Document1 pageFORMF2014debasishkcpNo ratings yet
- Needle Stick Injyry PolicyDocument16 pagesNeedle Stick Injyry PolicyJery JsNo ratings yet
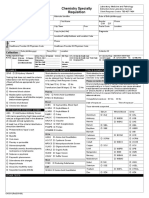
- Ground Floor, Lagman-Garcia BLDG., Molino Road, Molino 3, Bacoor City, Cavite (046) 516 7645 /0970-2186-355 / 0917-6818-948 EmailDocument1 pageGround Floor, Lagman-Garcia BLDG., Molino Road, Molino 3, Bacoor City, Cavite (046) 516 7645 /0970-2186-355 / 0917-6818-948 EmailFrances Marie RiveraNo ratings yet
- VBA-21-0960G-4-ARE Intestinal Surgery PDFDocument3 pagesVBA-21-0960G-4-ARE Intestinal Surgery PDFCombat CraigNo ratings yet
- Hep B Declination - Fillable 2Document1 pageHep B Declination - Fillable 2navneetshekhar.11No ratings yet
- WHO 2019 nCoV Clinical - CRF 2020.3 EngDocument5 pagesWHO 2019 nCoV Clinical - CRF 2020.3 EngPriyanka Alivia AziziNo ratings yet
- Hep B DeclinationDocument1 pageHep B Declinationnavneetshekhar.11No ratings yet
- DR Anup Warrier - How To Identify Hospital Acquired InfectionDocument22 pagesDR Anup Warrier - How To Identify Hospital Acquired InfectionMinusha CNo ratings yet
- Vaccine Beneficiary Status: Past Medical HistoryDocument1 pageVaccine Beneficiary Status: Past Medical HistoryTarannum khatriNo ratings yet
- AbxtimeoutDocument2 pagesAbxtimeoutAkbar Eka PutraNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Night BeforeDocument3 pagesNight BeforeChris MoffettNo ratings yet
- For Print - PADocument4 pagesFor Print - PAJU DYNo ratings yet
- Case LoadDocument3 pagesCase LoadFrancis Raphael PitogoNo ratings yet
- Hepatitis B Documentation Form: PARENT/GUARDIAN SIGNATUREDocument1 pageHepatitis B Documentation Form: PARENT/GUARDIAN SIGNATUREMeera KrishnanNo ratings yet
- Annual Health RecordDocument2 pagesAnnual Health RecordCarmela FranciscoNo ratings yet
- Flu Vaccine FormDocument1 pageFlu Vaccine FormEastwest BoundNo ratings yet
- Blood Transfusion Reaction FormDocument2 pagesBlood Transfusion Reaction Formbmci.bongNo ratings yet
- CDC Covid-19 Report FormDocument2 pagesCDC Covid-19 Report FormiggybauNo ratings yet
- Admission LetterDocument17 pagesAdmission LettermarkochikongoyeNo ratings yet
- Health FormsDocument9 pagesHealth Formserika luna romanNo ratings yet
- HEALTH FORM RSCC 1Document4 pagesHEALTH FORM RSCC 1Garlyn TaycoNo ratings yet
- VBA-21-0960G-2-ARE Gallbladder Pancreas PDFDocument4 pagesVBA-21-0960G-2-ARE Gallbladder Pancreas PDFCombat CraigNo ratings yet
- Health Screening and Assessment Form - SampleDocument3 pagesHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Pre Op Antibiotic Audit FormDocument1 pagePre Op Antibiotic Audit FormERWINNo ratings yet
- COVID 19 Revised Monitoring Form 2021Document3 pagesCOVID 19 Revised Monitoring Form 2021Aaron Paul BernasNo ratings yet
- Prenatal Check Up InterviewDocument7 pagesPrenatal Check Up InterviewSHIELOU LOMODNo ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- Medical CertDocument1 pageMedical CertCharan JaganNo ratings yet
- Reimbursement Claim - Hospital Treatment Certificate - FinalDocument3 pagesReimbursement Claim - Hospital Treatment Certificate - Finalsanyogitasawant5No ratings yet
- Initial and Annual Health RecordDocument2 pagesInitial and Annual Health RecordJames DionedaNo ratings yet
- Pre AuthorizationForPertrochantericFractureDocument2 pagesPre AuthorizationForPertrochantericFracturepatrickarilloNo ratings yet
- FRM CH 0311Document1 pageFRM CH 0311elCharlesFNo ratings yet
- Deed of Undertaking Limited F2F InternshipDocument2 pagesDeed of Undertaking Limited F2F InternshipMarie LlanesNo ratings yet
- IIMU MBA 2020 A8 Medical Fitness CertificateDocument1 pageIIMU MBA 2020 A8 Medical Fitness CertificateAayoush GuptaNo ratings yet
- Identifying Healthcare-Associated Infections (HAI) For NHSN SurveillanceDocument26 pagesIdentifying Healthcare-Associated Infections (HAI) For NHSN Surveillancedwi haryatiNo ratings yet
- (Post Test - 5 Points) : Environmental BackgroundDocument2 pages(Post Test - 5 Points) : Environmental BackgroundKristil ChavezNo ratings yet
- Needle Stick Injury FormDocument3 pagesNeedle Stick Injury FormUsma-i- Rasool100% (1)
- 030 - Blood Transfusion Vital Signs SheetDocument3 pages030 - Blood Transfusion Vital Signs Sheetعبدالله الرعويNo ratings yet
- Maternal & Child Health BookletDocument17 pagesMaternal & Child Health BookletAtina LavadiaNo ratings yet
- IIMU MBA 2020 A8 Medical Fitness CertificateDocument1 pageIIMU MBA 2020 A8 Medical Fitness CertificateAayoush GuptaNo ratings yet
- 108820lateral Move Molecular Assay For Horse StranglesDocument3 pages108820lateral Move Molecular Assay For Horse StranglesneriktjpcoNo ratings yet
- Eqas 2019 Form - NewDocument2 pagesEqas 2019 Form - NewAlfreah Jean Tambasen100% (3)
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Portfolio Reflection-2Document3 pagesPortfolio Reflection-2api-507520601No ratings yet
- Table Saw Safety FinalDocument24 pagesTable Saw Safety Finalvolatileyasser100% (1)
- Fluids and ElectrolytesDocument9 pagesFluids and Electrolytespaulzilicous.artNo ratings yet
- 6 SOP of Phosphate Sump PitDocument1 page6 SOP of Phosphate Sump PitAbhishek ChaskarNo ratings yet
- Draft: This Part Is Prepared by Kajal Sapra and Oshadi Puhabhugoda ArachchigedoDocument6 pagesDraft: This Part Is Prepared by Kajal Sapra and Oshadi Puhabhugoda ArachchigedoAmandeep SidhuNo ratings yet
- Answer Sheet: Maximum of 15 Sentences Only Per Number/question DUE NOVEMBER 10, 2020Document4 pagesAnswer Sheet: Maximum of 15 Sentences Only Per Number/question DUE NOVEMBER 10, 2020Arven FrancoNo ratings yet
- Vitabrid Company Intro ENG 180119Document41 pagesVitabrid Company Intro ENG 180119Kate NguyenNo ratings yet
- 10 1002@aorn 12696Document7 pages10 1002@aorn 12696Salim RumraNo ratings yet
- Amagram in 65Document43 pagesAmagram in 65dgshailNo ratings yet
- ZoonosesDocument1,225 pagesZoonosesSuárez David100% (2)
- Infections:: Jadwal Acara Pelatihan In-Alarm Hari II: Minggu, 28 Februari 2021 Waktu Menit Acara Pembicara AbsensiDocument1 pageInfections:: Jadwal Acara Pelatihan In-Alarm Hari II: Minggu, 28 Februari 2021 Waktu Menit Acara Pembicara AbsensiClarestaNo ratings yet
- Ace Finance - Workplace Health and Safety Policy and ProcedDocument13 pagesAce Finance - Workplace Health and Safety Policy and ProcedIbrahim VolpiNo ratings yet
- Models - of - Stress - Levine & Scotch 1970Document21 pagesModels - of - Stress - Levine & Scotch 1970MadeleineNo ratings yet
- Tourniquet Use at The Boston Marathon Bombing: Lost in TranslationDocument6 pagesTourniquet Use at The Boston Marathon Bombing: Lost in TranslationFabio Ferreira SaNo ratings yet
- 3.indicators and Measurement of Economic DevelopmentDocument17 pages3.indicators and Measurement of Economic Developmentramkumar100% (1)
- Process Flow Chart Template - TemplateLab - Com-1Document1 pageProcess Flow Chart Template - TemplateLab - Com-1Rio Krystal Molate100% (1)
- ROTR Statblock Cards - Skinsaw Murders (For Distribution)Document60 pagesROTR Statblock Cards - Skinsaw Murders (For Distribution)Engin YagmurdereliNo ratings yet
- Brain DumpDocument59 pagesBrain Dumpruchitac28No ratings yet
- EAPP Q3 Wks-1-8 48pp-PSDocument52 pagesEAPP Q3 Wks-1-8 48pp-PSJames CunetaNo ratings yet
- 1-Example 9Document3 pages1-Example 9Rudolf KiraljNo ratings yet
- 9 TH Test 2 9B3Document3 pages9 TH Test 2 9B3Sana MoumniNo ratings yet
- About COR-skills Project: Why Should You Be Interested in Our Courses?Document2 pagesAbout COR-skills Project: Why Should You Be Interested in Our Courses?Taina AvramescuNo ratings yet
- PsychodramaDocument5 pagesPsychodramaAkhila R KrishnaNo ratings yet
- Indoor Plant Technology For Health Environment Sustainability HAL Report 2011 PDFDocument52 pagesIndoor Plant Technology For Health Environment Sustainability HAL Report 2011 PDFSakshi SahuNo ratings yet
- Focus On PAD: Peripheral Artery Disease (PAD)Document2 pagesFocus On PAD: Peripheral Artery Disease (PAD)Durga BasnetNo ratings yet
- The Role of Self-Concept in The Challenges and Coping Mechanisms of Nursing StudentsDocument20 pagesThe Role of Self-Concept in The Challenges and Coping Mechanisms of Nursing StudentsNamoAmitofouNo ratings yet
- Training Module MerkchemDocument110 pagesTraining Module MerkchemArila Roberts100% (1)
- Holy Trinity College of General Santos CityDocument20 pagesHoly Trinity College of General Santos CityMargareth RodaNo ratings yet
- SEC6010 - Planning For Information SecurityDocument9 pagesSEC6010 - Planning For Information SecurityVenkata Pathi JaligamaNo ratings yet
- Effects of A Simulation-Based Education Programme On Delirium Care For Critical Care Nurses: A Randomized Controlled TrialDocument11 pagesEffects of A Simulation-Based Education Programme On Delirium Care For Critical Care Nurses: A Randomized Controlled TrialAz SalNo ratings yet