Download as pdf or txt
You might also like
- Anesthesia Crash CourseDocument32 pagesAnesthesia Crash Coursechris husonNo ratings yet
- Claim Form Regency For Expats PDFDocument2 pagesClaim Form Regency For Expats PDFChris DarkNo ratings yet
- MembershipContract PDFDocument2 pagesMembershipContract PDFbobgreen19870% (1)
- Administering Intradermal InjectionDocument2 pagesAdministering Intradermal InjectionMoiraMaeBeridoBalite100% (1)
- Personal Philosophy of NursingDocument4 pagesPersonal Philosophy of Nursingapi-390528288No ratings yet
- Your Extras and Medical Claim Form: SECTION A: Your DetailsDocument3 pagesYour Extras and Medical Claim Form: SECTION A: Your DetailsTGNo ratings yet
- Ci Benefits Rights InformationDocument15 pagesCi Benefits Rights InformationBladimir LoraNo ratings yet
- Health Claim Form: Part A (To Be Filled by Insured)Document3 pagesHealth Claim Form: Part A (To Be Filled by Insured)Harshad DhodiNo ratings yet
- Claim FormDocument3 pagesClaim FormInvestor ProtegeNo ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- 5Document10 pages5John C. LewisNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Insurance Claim FormDocument9 pagesInsurance Claim FormRahmaNo ratings yet
- All Medicare C73ac3dea5Document12 pagesAll Medicare C73ac3dea5Pradeep SahuNo ratings yet
- NDIS Check Refund FormDocument3 pagesNDIS Check Refund FormNika GarciaNo ratings yet
- Reliancegeneral - Co.in 1800 3009 4890 3009: Health Claim FormDocument4 pagesReliancegeneral - Co.in 1800 3009 4890 3009: Health Claim FormSumit BhallaNo ratings yet
- Reliance Health Claim FormDocument4 pagesReliance Health Claim FormarijitnirmalNo ratings yet
- Cigna Global Claim FormDocument3 pagesCigna Global Claim Formrsiabs marketingNo ratings yet
- All Medicare C73ac3dea5Document12 pagesAll Medicare C73ac3dea5shivamvijaymishra1703No ratings yet
- Absa Consultants and Actuaries Afrimat Pension Fund (Withdrawal) - 101456903 PDFDocument3 pagesAbsa Consultants and Actuaries Afrimat Pension Fund (Withdrawal) - 101456903 PDFAlvin JantjiesNo ratings yet
- CIBenefitsRightsInformation HollyMartinez-727202103144858Document15 pagesCIBenefitsRightsInformation HollyMartinez-727202103144858Faith Nevaeh MartinezNo ratings yet
- Please Update Mentioned Mobile Number As Primary Contact Details Against My Policy. I Also Hereby Confirm To Be Contacted On The Number Provided Below For Claim Status /policy RenewalDocument4 pagesPlease Update Mentioned Mobile Number As Primary Contact Details Against My Policy. I Also Hereby Confirm To Be Contacted On The Number Provided Below For Claim Status /policy RenewalSumit BhallaNo ratings yet
- Forms Payout Others Web 23 AprilDocument2 pagesForms Payout Others Web 23 AprilYo PaisaNo ratings yet
- SW Claim FormDocument5 pagesSW Claim FormNovaPNo ratings yet
- Change of OwnershipDocument3 pagesChange of Ownerships2gfxzkw2wNo ratings yet
- Group Hospital and Surgical Claim FormDocument4 pagesGroup Hospital and Surgical Claim FormYiki TanNo ratings yet
- Bupa Claim FormDocument1 pageBupa Claim FormcrazydeveloperNo ratings yet
- Walters Shameka 46370 MedicaidrecertappDocument4 pagesWalters Shameka 46370 Medicaidrecertappdoenyka.lewisNo ratings yet
- Getting Started Pack - IEA Only Oct 2020Document9 pagesGetting Started Pack - IEA Only Oct 2020Akitha SiyaginaNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Wageworks Pay Me Back Claim Form Instructions: Please Read This Before Submitting Your Claim FormDocument2 pagesWageworks Pay Me Back Claim Form Instructions: Please Read This Before Submitting Your Claim FormbmxengineerNo ratings yet
- Commercial Work Injury Compensation Claim FormDocument3 pagesCommercial Work Injury Compensation Claim FormHihiNo ratings yet
- CIBenefitsRightsInformation BILLIECASEBIER-727202007224240Document15 pagesCIBenefitsRightsInformation BILLIECASEBIER-727202007224240BILLIE CASEBIERNo ratings yet
- Reimbursement Claim FormDocument1 pageReimbursement Claim FormmoinuNo ratings yet
- Claim Form: DD MM YY DD MM YYDocument3 pagesClaim Form: DD MM YY DD MM YYAnonymous SM6kY6tB1sNo ratings yet
- Extended Health Benefits Claim FormDocument2 pagesExtended Health Benefits Claim FormHolystreamNo ratings yet
- OPD Form IHealthcare-2Document2 pagesOPD Form IHealthcare-2Masoom Kazmi100% (1)
- Reimbursement Claim Form PDFDocument3 pagesReimbursement Claim Form PDFMuhammak SKNo ratings yet
- Jawad Claim FormDocument2 pagesJawad Claim FormJawad KarimNo ratings yet
- IRDAI Registration No. 103. Reliance General Insurance Company LimitedDocument4 pagesIRDAI Registration No. 103. Reliance General Insurance Company LimitedSumit BhallaNo ratings yet
- ICICI Lombard Health Care Claim Form - Outpatient DepartmentDocument2 pagesICICI Lombard Health Care Claim Form - Outpatient Departmentanon_103901460No ratings yet
- Redirection of Benefit PaymentDocument4 pagesRedirection of Benefit PaymentStephanie PrangnellNo ratings yet
- ApointeeDocument8 pagesApointeeaymanNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- AETNADocument5 pagesAETNATRTNo ratings yet
- Niramaya FaqDocument4 pagesNiramaya FaqAnonymous TD99UqSLNo ratings yet
- Medical Claim Reimbursement Form EnglishDocument2 pagesMedical Claim Reimbursement Form EnglishHananAhmedNo ratings yet
- DFSA Form PDFDocument2 pagesDFSA Form PDFvalerieNo ratings yet
- Form 1. Application For Travel and Accommodation Assistance - April 2019Document4 pagesForm 1. Application For Travel and Accommodation Assistance - April 2019chris tNo ratings yet
- Chubb14-345-1122 Uber Personal Injury Claim Form-INTDocument7 pagesChubb14-345-1122 Uber Personal Injury Claim Form-INTEidrian RicardoNo ratings yet
- MOF Suspension Letter TCF - J307415625Document2 pagesMOF Suspension Letter TCF - J307415625Thomas BarnettNo ratings yet
- ICICI - Claim FormDocument5 pagesICICI - Claim FormRaja RamanNo ratings yet
- Ci Benefits Rights InformationDocument15 pagesCi Benefits Rights Informationchris johnNo ratings yet
- Claim Form AustraliaDocument8 pagesClaim Form AustraliarosemcdoNo ratings yet
- Sukshma Hospi CashDocument4 pagesSukshma Hospi CashAdemuyiwa OlaniyiNo ratings yet
- Firstshore - Payment Reversal FormDocument4 pagesFirstshore - Payment Reversal Formkelex32No ratings yet
- Financial Assistance Scheme For Uncontracted Assessors: Application Form - IndividualsDocument4 pagesFinancial Assistance Scheme For Uncontracted Assessors: Application Form - Individualsn_san5No ratings yet
- Disability Critical Illness Medical Reimbursement or Hospitalization Claim FormDocument5 pagesDisability Critical Illness Medical Reimbursement or Hospitalization Claim FormAkoSiAudreyNo ratings yet
- Claim Form NewDocument4 pagesClaim Form Newparvazahmed03191No ratings yet
- Alico Indemnity Medical Claim FormDocument2 pagesAlico Indemnity Medical Claim FormJalal Al-QutobNo ratings yet
- SAE Claim FormDocument5 pagesSAE Claim FormNovaPNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (2)
- Engine - Commissioning Check SheetDocument1 pageEngine - Commissioning Check SheetKarthii AjuNo ratings yet
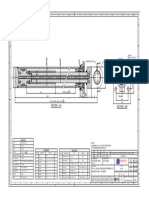
- Line-40 - Ga-Rh-240128-Cyl-418 - Feed Tilt Cylinder - (125-50-290) - (MMPL) - R1Document1 pageLine-40 - Ga-Rh-240128-Cyl-418 - Feed Tilt Cylinder - (125-50-290) - (MMPL) - R1Karthii AjuNo ratings yet
- Line-30 - Ga-Rh-240128-Cyl-417 - Boom Extension Cylinder - (80-50-1038) - (MMPL) - R1Document1 pageLine-30 - Ga-Rh-240128-Cyl-417 - Boom Extension Cylinder - (80-50-1038) - (MMPL) - R1Karthii AjuNo ratings yet
- MCN Resume Updated 22nd SepDocument3 pagesMCN Resume Updated 22nd SepKarthii AjuNo ratings yet
- R02 Offer For Eddy Current Dyamometer With Controller - 12.06.2023Document9 pagesR02 Offer For Eddy Current Dyamometer With Controller - 12.06.2023Karthii AjuNo ratings yet
- Oil Analysis Offer - MMPL2Document2 pagesOil Analysis Offer - MMPL2Karthii AjuNo ratings yet
- Quotation For Oil TestingDocument1 pageQuotation For Oil TestingKarthii AjuNo ratings yet
- Sos GainwellDocument4 pagesSos GainwellKarthii AjuNo ratings yet
- Asn To KolDocument1 pageAsn To KolKarthii AjuNo ratings yet
- Travel Request Form 2022Document1 pageTravel Request Form 2022Karthii AjuNo ratings yet
- Holiday List 2023 - APPROVEDDocument1 pageHoliday List 2023 - APPROVEDKarthii AjuNo ratings yet
- TNSTCDocument1 pageTNSTCKarthii AjuNo ratings yet
- Invoice HEGFD20220210335Document1 pageInvoice HEGFD20220210335Karthii AjuNo ratings yet
- Air Compressor Attachment PartsDocument5 pagesAir Compressor Attachment PartsKarthii AjuNo ratings yet
- lh410 48 Technical Specifications EnglishDocument18 pageslh410 48 Technical Specifications EnglishKarthii AjuNo ratings yet
- EX110 Observation ReportDocument7 pagesEX110 Observation ReportKarthii AjuNo ratings yet
- Distribution Business Unit Cummins Field Service Report Deccan Sales and Services Private Limited (Indore)Document2 pagesDistribution Business Unit Cummins Field Service Report Deccan Sales and Services Private Limited (Indore)Karthii AjuNo ratings yet
- Attachment Parts For Starting Motor & AlternatorDocument6 pagesAttachment Parts For Starting Motor & AlternatorKarthii AjuNo ratings yet
- Distribution Business Unit Cummins Field Service Report Deccan Sales and Services Private Limited (Indore)Document2 pagesDistribution Business Unit Cummins Field Service Report Deccan Sales and Services Private Limited (Indore)Karthii AjuNo ratings yet
- AssessmentDocument19 pagesAssessmentKarthii AjuNo ratings yet
- Alternator (Bus) Mercedes OM 904 LA: (Europa) (Engine)Document21 pagesAlternator (Bus) Mercedes OM 904 LA: (Europa) (Engine)Karthii AjuNo ratings yet
- Air Compressor (Bus) Mercedes OM 904 LA: (Europa) (Engine)Document11 pagesAir Compressor (Bus) Mercedes OM 904 LA: (Europa) (Engine)Karthii AjuNo ratings yet
- Camshaft and Timing Parts (Bus) Mercedes OM 904 LA: (Europa) (Engine)Document4 pagesCamshaft and Timing Parts (Bus) Mercedes OM 904 LA: (Europa) (Engine)Karthii AjuNo ratings yet
- Hydraulic Room Drawing PDF 3 ColourDocument1 pageHydraulic Room Drawing PDF 3 ColourKarthii AjuNo ratings yet
- Torque Specifications - Fasteners: Nut and Bolt Size, MM 280M or Better Torque, N M 280M or Better Torque, LB FTDocument1 pageTorque Specifications - Fasteners: Nut and Bolt Size, MM 280M or Better Torque, N M 280M or Better Torque, LB FTKarthii AjuNo ratings yet
- Application Systems: Powder DynamometersDocument6 pagesApplication Systems: Powder DynamometersKarthii AjuNo ratings yet
- Tandem DynamometersDocument5 pagesTandem DynamometersKarthii AjuNo ratings yet
- Gear Box Test SetupDocument20 pagesGear Box Test SetupKarthii AjuNo ratings yet
- List of Customers: ISO 9001:2015 Certified CertifiedDocument5 pagesList of Customers: ISO 9001:2015 Certified CertifiedKarthii AjuNo ratings yet
- Electronic Parts Catalog - Option DetailDocument2 pagesElectronic Parts Catalog - Option DetailKarthii AjuNo ratings yet
- Senior Citizen Discount and Benefits ChecklistDocument7 pagesSenior Citizen Discount and Benefits ChecklistKROS EffectsNo ratings yet
- Routes of Drug AdministrationDocument37 pagesRoutes of Drug AdministrationAhmed YTNo ratings yet
- Assessment of Attitude of Nursing Mothers Towards Childhood Immunization in Some Selected Communities in Bali, LGA of Taraba StateDocument56 pagesAssessment of Attitude of Nursing Mothers Towards Childhood Immunization in Some Selected Communities in Bali, LGA of Taraba StateJoshua Bature SamboNo ratings yet
- AssessmentDocument3 pagesAssessmentLOUISE JOSEL TACLAYNo ratings yet
- Sample Formal Invitation Letter For Chief GuestDocument2 pagesSample Formal Invitation Letter For Chief Guestanshul guptaNo ratings yet
- Palliative CareDocument160 pagesPalliative CareReni PurwoNo ratings yet
- Registration BrochureDocument21 pagesRegistration BrochurePratamaAnandaNo ratings yet
- Naditarangini BrochureDocument12 pagesNaditarangini BrochureHarikrishnan MeenakshisundaramNo ratings yet
- Child and Adolescent Psychiatry - Blackwell's Neurology and Psychiatry Access SeriesDocument416 pagesChild and Adolescent Psychiatry - Blackwell's Neurology and Psychiatry Access SeriesErickson Arthur Siahaan0% (1)
- 2020 Dental History Form PacketDocument6 pages2020 Dental History Form PacketLandon AllenNo ratings yet
- Bulletin 125Document39 pagesBulletin 125Rasangi Sumudu Clare SuraweeraNo ratings yet
- Clinical Rotation Plan of 4th Year B.SC Nursing 2018-19-1Document1 pageClinical Rotation Plan of 4th Year B.SC Nursing 2018-19-1Patel Amee100% (4)
- Interview Questions Asked in PPSC 2015 in Diff Sectors: RawalpindiDocument4 pagesInterview Questions Asked in PPSC 2015 in Diff Sectors: RawalpindiAli ArshadNo ratings yet
- HEALTH - Book 4 Module 16 - Planning For Health CareerDocument26 pagesHEALTH - Book 4 Module 16 - Planning For Health CareerHECTOR ARANTE TANNo ratings yet
- Aseptic Technique ProcedureDocument10 pagesAseptic Technique ProcedureaksinuNo ratings yet
- Person-Centered: Caring For Older AdultsDocument1 pagePerson-Centered: Caring For Older AdultsAprillia AlmaasNo ratings yet
- Migraine - Symptoms, Causes, Treatment, Triggers, and MoreDocument35 pagesMigraine - Symptoms, Causes, Treatment, Triggers, and MoreKarlla SuarezNo ratings yet
- Annex 18 Experiences On Registration of Medical Tourism Ecozones in The PhilippinesDocument5 pagesAnnex 18 Experiences On Registration of Medical Tourism Ecozones in The PhilippineswhiosharnaNo ratings yet
- Trainng Programpdf166990215462Document3 pagesTrainng Programpdf166990215462Raghav SolankiNo ratings yet
- Evidence Based MedicineDocument55 pagesEvidence Based MedicineHelen SusantoNo ratings yet
- Acute Liver Failure: by - Ahmed Osama - Habiba Yehia - Ahmed Tarek - Ahmed Adham - Ahmed AbdelkaderDocument19 pagesAcute Liver Failure: by - Ahmed Osama - Habiba Yehia - Ahmed Tarek - Ahmed Adham - Ahmed AbdelkaderAhmed AbdelkaderNo ratings yet
- Exam Questions AHM-250: Healthcare Management: An IntroductionDocument24 pagesExam Questions AHM-250: Healthcare Management: An IntroductionSivaNo ratings yet
- CounsellingDocument52 pagesCounsellingAnnapurna Dangeti100% (1)
- Fluconazole Final Dossier - Enrollemt Number 2Document139 pagesFluconazole Final Dossier - Enrollemt Number 2lathasunil1976No ratings yet
- The Journey of Reforms by Integrating ICT: Case of KNH - Connected Kenya - Richard LesiyampeDocument22 pagesThe Journey of Reforms by Integrating ICT: Case of KNH - Connected Kenya - Richard LesiyampeICT AUTHORITYNo ratings yet
- Reference ThesisDocument13 pagesReference ThesisGhina SalsabilaNo ratings yet
- Food, Nutrition and HygieneDocument2 pagesFood, Nutrition and HygieneAmit TiwariNo ratings yet