
Standard Risk B Acute Lymphoblastic Leukemia
Standard Risk B Acute Lymphoblastic Leukemia
You might also like
- Test Bank For Human Diseases 5th Edition by NeighborsDocument4 pagesTest Bank For Human Diseases 5th Edition by NeighborsEmily Mccormick100% (37)
- INV06 Direct Amplification of FTA and Swab Samples Using The Investigator Argus X-12 QS KitDocument7 pagesINV06 Direct Amplification of FTA and Swab Samples Using The Investigator Argus X-12 QS KitWilson Campos RojasNo ratings yet
- Sternal Wound Procedures Require Coding Accuracy OpDocument4 pagesSternal Wound Procedures Require Coding Accuracy OpbushaesNo ratings yet
- T AllDocument10 pagesT Alllasheseye676No ratings yet
- Acute Leukemia ProtocolDocument13 pagesAcute Leukemia ProtocolBol Dhalbeny MalualNo ratings yet
- Protocol For HighDocument11 pagesProtocol For Highlasheseye676No ratings yet
- ALL Protocol-Feb 19, 2016Document26 pagesALL Protocol-Feb 19, 2016Mohammed HaiderNo ratings yet
- BFM 95 ProtocolDocument5 pagesBFM 95 ProtocolGlobal cancerNo ratings yet
- T-All 1Document9 pagesT-All 1Mobin Ur Rehman KhanNo ratings yet
- SMB 1Document7 pagesSMB 1Subhecchha BaidyaNo ratings yet
- HB-1860-009 HB HID Investigator 24plex QS 0221 WWDocument48 pagesHB-1860-009 HB HID Investigator 24plex QS 0221 WWJoshue RosalesNo ratings yet
- Advanced Single or Dual Cell Lithium-Ion/ Lithium-Polymer Charge Management ControllersDocument24 pagesAdvanced Single or Dual Cell Lithium-Ion/ Lithium-Polymer Charge Management Controllers123No ratings yet
- pmTFP1 Cx32Document4 pagespmTFP1 Cx32AlleleBiotechNo ratings yet
- IFU Human JAK2 V617F Mutation Detection Kit (Digital PCR) A1.0 en-USDocument7 pagesIFU Human JAK2 V617F Mutation Detection Kit (Digital PCR) A1.0 en-USMohammed H. KeshtaNo ratings yet
- Protocol Sanger Sequencing SARS-CoV-2 B117 B1351 BrochureDocument10 pagesProtocol Sanger Sequencing SARS-CoV-2 B117 B1351 BrochureCristian VillarNo ratings yet
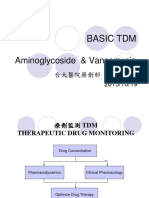
- Aminoglycoside & Vancomycin: Basic TDMDocument57 pagesAminoglycoside & Vancomycin: Basic TDMft84nzzc92No ratings yet
- pmTFP1 VimentinDocument4 pagespmTFP1 VimentinAlleleBiotechNo ratings yet
- pmTFP1 Elp1Document4 pagespmTFP1 Elp1AlleleBiotechNo ratings yet
- Dosage CardDocument2 pagesDosage CardKleibert Maciel100% (1)
- pmTFP1 VSV GDocument4 pagespmTFP1 VSV GAlleleBiotechNo ratings yet
- Realizing Precision Timing With The MSP430Document40 pagesRealizing Precision Timing With The MSP430anon_312676694No ratings yet
- GPM6A Research PaperDocument7 pagesGPM6A Research PaperRida ArifNo ratings yet
- Biokinetic of Tc99m-TetrofosminDocument7 pagesBiokinetic of Tc99m-TetrofosminKhairul AimanNo ratings yet
- 09 The aminoglycoside antibioticsDocument27 pages09 The aminoglycoside antibioticsAYAT NOFALNo ratings yet
- BFM 2002 Supplemental - Tables - JCO.2013.48.6522Document7 pagesBFM 2002 Supplemental - Tables - JCO.2013.48.6522erickmattosNo ratings yet
- Technique Chart Const-JSDocument6 pagesTechnique Chart Const-JSNumdaNo ratings yet
- pmTFP1 Cx26Document4 pagespmTFP1 Cx26AlleleBiotechNo ratings yet
- J Nucl Med-1991-Hung-2162-8 MIBI PreparacionDocument8 pagesJ Nucl Med-1991-Hung-2162-8 MIBI PreparacionJuliana CasalyNo ratings yet
- AN12626Document31 pagesAN12626James Andy CNo ratings yet
- 107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2Document4 pages107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2ft84nzzc92No ratings yet
- 280299-001 LHC0009MDocument3 pages280299-001 LHC0009MSamantha YongNo ratings yet
- pmTFP1 VinculinDocument5 pagespmTFP1 VinculinAlleleBiotechNo ratings yet
- 04QTDocument40 pages04QTSergio MontesNo ratings yet
- pmTFP1 ZyxinDocument5 pagespmTFP1 ZyxinAlleleBiotechNo ratings yet
- LCD MicrochipDocument40 pagesLCD Microchipgorea_grigNo ratings yet
- Noncompartmental Analysis: Deficiencies of Compartmental AnalysisDocument51 pagesNoncompartmental Analysis: Deficiencies of Compartmental Analysisshripathyd1No ratings yet
- Torsades de Pointes: Josh FarkasDocument8 pagesTorsades de Pointes: Josh FarkasnurhidayahNo ratings yet
- Axcent Cetus x12 Brochure en 0120Document6 pagesAxcent Cetus x12 Brochure en 0120Shaif ZahrahNo ratings yet
- 2.postoperative Arrhythmias in Open-Heart SurgeryDocument9 pages2.postoperative Arrhythmias in Open-Heart Surgeryganda gandaNo ratings yet
- Total XVDocument8 pagesTotal XVMohammed HaiderNo ratings yet
- 1995 - NAR - Solid-Phase Revesible Immobilization For The Isolation of PCR ProductsDocument2 pages1995 - NAR - Solid-Phase Revesible Immobilization For The Isolation of PCR ProductsKhoa NguyendangNo ratings yet
- QCLightning ManualDocument19 pagesQCLightning Manualrob burrNo ratings yet
- Protocol 00001947man Hcytomag-60kDocument32 pagesProtocol 00001947man Hcytomag-60kFrancisco SiirNo ratings yet
- American J Hematol - 2023 - JoinerDocument4 pagesAmerican J Hematol - 2023 - Joinersalman mehriNo ratings yet
- Cytokine, Magnetic, Panel - 2013 - Human Cytokine Chemokine Magnetic Bead Panel 96 Well Plate AssayDocument30 pagesCytokine, Magnetic, Panel - 2013 - Human Cytokine Chemokine Magnetic Bead Panel 96 Well Plate AssayEduardo SandovalNo ratings yet
- An4364 PDFDocument34 pagesAn4364 PDFjoseluisblanco69No ratings yet
- V003supp PDFDocument3 pagesV003supp PDFR-win PrawirodiharjoNo ratings yet
- Quikchange Site-Directed Mutagenesis Kit: Instruction ManualDocument20 pagesQuikchange Site-Directed Mutagenesis Kit: Instruction ManualMatthew MancusoNo ratings yet
- Advances in The Diagnosis and Treatment of ThrombocytopeniaDocument50 pagesAdvances in The Diagnosis and Treatment of ThrombocytopeniaLetnanCapungNo ratings yet
- NXP CommunicatorDocument6 pagesNXP Communicator123No ratings yet
- Genotype - Accupower Jak2Document34 pagesGenotype - Accupower Jak2Elvan Dwi WidyadiNo ratings yet
- REFERENCE Kintex 7 Rad Complete ReportDocument39 pagesREFERENCE Kintex 7 Rad Complete Reportfarzian1No ratings yet
- Icd 10 Up-Date 2010Document66 pagesIcd 10 Up-Date 2010adyaNo ratings yet
- 2019 nCoVmanual20200217 enDocument16 pages2019 nCoVmanual20200217 ensekharurlaNo ratings yet
- Dspic PDFDocument530 pagesDspic PDFmester1025No ratings yet
- pmTFP1 ActinDocument4 pagespmTFP1 ActinAlleleBiotechNo ratings yet
- Multiplex Primers Probes PrinterDocument3 pagesMultiplex Primers Probes PrinterFlavio AlvesNo ratings yet
- NXP CommunicatorDocument7 pagesNXP CommunicatorIonut37No ratings yet
- 39900article - Paper - Àlex CalleDocument10 pages39900article - Paper - Àlex Calle河井伸哉No ratings yet
- Gerontologic Nursing 6th EditionDocument61 pagesGerontologic Nursing 6th Editionjulie.navas368100% (52)
- Brochure - Zoonotic Disease Workshop - FinalDocument1 pageBrochure - Zoonotic Disease Workshop - FinalAbhipsa PradhanNo ratings yet
- PALS (Pediatric Advanced Life Support)Document48 pagesPALS (Pediatric Advanced Life Support)Jackson HakimNo ratings yet
- NCP ScoliosisDocument4 pagesNCP ScoliosisCharley DegamoNo ratings yet
- PPI VIP Graha Medika AgustusDocument208 pagesPPI VIP Graha Medika AgustusfirasyauqiNo ratings yet
- The Goal of Water4LifeDocument10 pagesThe Goal of Water4LifeHuiYingNo ratings yet
- A Case of Multiple Cranial Nerves Palsy Post ElectrocutionDocument4 pagesA Case of Multiple Cranial Nerves Palsy Post ElectrocutionEditor IJTSRDNo ratings yet
- Meropenem - Drug Information - UpToDate-2Document8 pagesMeropenem - Drug Information - UpToDate-2Vh TRNo ratings yet
- Study of Clinical, Biochemical Evaluation and Outcome in Hypertrophic Pyloric StenosisDocument4 pagesStudy of Clinical, Biochemical Evaluation and Outcome in Hypertrophic Pyloric StenosiszapomannNo ratings yet
- 10-OBGYN-Glory GroupDocument46 pages10-OBGYN-Glory Groupanmar alkhudhriNo ratings yet
- 1.3.+delusions+ +hallucinationsDocument22 pages1.3.+delusions+ +hallucinationsAna P UCAMNo ratings yet
- WEEK 7-PS M6 CU6 - Care of Clients With Schizophrenia and Related DisordersDocument12 pagesWEEK 7-PS M6 CU6 - Care of Clients With Schizophrenia and Related DisordersMaica LectanaNo ratings yet
- Laboratory - 1 - G4 StatisticsDocument16 pagesLaboratory - 1 - G4 StatisticsJENNEFER LEENo ratings yet
- Homeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Document21 pagesHomeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Yuldash100% (2)
- (Advances in Behavioral Biology 50) Olivier Dulac (Auth.), Isabelle Jambaqué, Maryse Lassonde, Olivier Dulac (Eds.) - Neuropsychology of Childhood Epilepsy (2002, Springer US)Document305 pages(Advances in Behavioral Biology 50) Olivier Dulac (Auth.), Isabelle Jambaqué, Maryse Lassonde, Olivier Dulac (Eds.) - Neuropsychology of Childhood Epilepsy (2002, Springer US)Vanez SusanibarNo ratings yet
- Healing Quantum Codes Códigos de Sanación Cuántica 1 - 5006236209752572132Document47 pagesHealing Quantum Codes Códigos de Sanación Cuántica 1 - 5006236209752572132Húgo PereiraNo ratings yet
- What's The Difference Between A Cold, The Flu, Seasonal Allergies, and CoronavirusDocument1 pageWhat's The Difference Between A Cold, The Flu, Seasonal Allergies, and CoronavirusManan BatraNo ratings yet
- Helmya Trauma ProtocolDocument85 pagesHelmya Trauma ProtocolAhmed ShehataNo ratings yet
- The Diagnostic Accuracy of Kernig's Sign, Brudzinski's Sign, and Nuchal Rigidity in Adults With Suspected MeningitisDocument7 pagesThe Diagnostic Accuracy of Kernig's Sign, Brudzinski's Sign, and Nuchal Rigidity in Adults With Suspected MeningitisNeymarNo ratings yet
- 3.0HEPATIT Lecture 5Document48 pages3.0HEPATIT Lecture 5Jiya MuhammadNo ratings yet
- Cog PsychDocument22 pagesCog PsychJoy Ann Corpuz GanadosNo ratings yet
- Australian Dental Journal - 2020 - Beaumont - Temporomandibular Disorder A Practical Guide For Dental Practitioners inDocument9 pagesAustralian Dental Journal - 2020 - Beaumont - Temporomandibular Disorder A Practical Guide For Dental Practitioners ingermanNo ratings yet
- NCM 117J (Maladaptive Pattern of Behavior) : Overview of Psychiatric Mental Health Nursing Module 1/7Document41 pagesNCM 117J (Maladaptive Pattern of Behavior) : Overview of Psychiatric Mental Health Nursing Module 1/7Abdelmar Susulan100% (1)
- Free Apo Psych Final Coaching Nov 2023 PDF PresentationDocument124 pagesFree Apo Psych Final Coaching Nov 2023 PDF PresentationsheynmalubayNo ratings yet
- Catch-22 by Joseph Heller Joseph Heller Biography: His Life and TimesDocument56 pagesCatch-22 by Joseph Heller Joseph Heller Biography: His Life and TimesAll DocumentsNo ratings yet
- CHN & NCDDocument92 pagesCHN & NCDlorelie asisNo ratings yet
- De La Salle Medical and Health Sciences InstituteDocument108 pagesDe La Salle Medical and Health Sciences InstituteJericho Daniel IgdanesNo ratings yet
- Feil & Filippi. EnglishDocument6 pagesFeil & Filippi. EnglishRia Utami Yuliani RiyutNo ratings yet
- CC1 Trans ProteinsDocument7 pagesCC1 Trans Proteinschayiezen0301No ratings yet
























































































Download as pdf or txt
You might also like
- Test Bank For Human Diseases 5th Edition by NeighborsDocument4 pagesTest Bank For Human Diseases 5th Edition by NeighborsEmily Mccormick100% (37)
- INV06 Direct Amplification of FTA and Swab Samples Using The Investigator Argus X-12 QS KitDocument7 pagesINV06 Direct Amplification of FTA and Swab Samples Using The Investigator Argus X-12 QS KitWilson Campos RojasNo ratings yet
- Sternal Wound Procedures Require Coding Accuracy OpDocument4 pagesSternal Wound Procedures Require Coding Accuracy OpbushaesNo ratings yet
- T AllDocument10 pagesT Alllasheseye676No ratings yet
- Acute Leukemia ProtocolDocument13 pagesAcute Leukemia ProtocolBol Dhalbeny MalualNo ratings yet
- Protocol For HighDocument11 pagesProtocol For Highlasheseye676No ratings yet
- ALL Protocol-Feb 19, 2016Document26 pagesALL Protocol-Feb 19, 2016Mohammed HaiderNo ratings yet
- BFM 95 ProtocolDocument5 pagesBFM 95 ProtocolGlobal cancerNo ratings yet
- T-All 1Document9 pagesT-All 1Mobin Ur Rehman KhanNo ratings yet
- SMB 1Document7 pagesSMB 1Subhecchha BaidyaNo ratings yet
- HB-1860-009 HB HID Investigator 24plex QS 0221 WWDocument48 pagesHB-1860-009 HB HID Investigator 24plex QS 0221 WWJoshue RosalesNo ratings yet
- Advanced Single or Dual Cell Lithium-Ion/ Lithium-Polymer Charge Management ControllersDocument24 pagesAdvanced Single or Dual Cell Lithium-Ion/ Lithium-Polymer Charge Management Controllers123No ratings yet
- pmTFP1 Cx32Document4 pagespmTFP1 Cx32AlleleBiotechNo ratings yet
- IFU Human JAK2 V617F Mutation Detection Kit (Digital PCR) A1.0 en-USDocument7 pagesIFU Human JAK2 V617F Mutation Detection Kit (Digital PCR) A1.0 en-USMohammed H. KeshtaNo ratings yet
- Protocol Sanger Sequencing SARS-CoV-2 B117 B1351 BrochureDocument10 pagesProtocol Sanger Sequencing SARS-CoV-2 B117 B1351 BrochureCristian VillarNo ratings yet
- Aminoglycoside & Vancomycin: Basic TDMDocument57 pagesAminoglycoside & Vancomycin: Basic TDMft84nzzc92No ratings yet
- pmTFP1 VimentinDocument4 pagespmTFP1 VimentinAlleleBiotechNo ratings yet
- pmTFP1 Elp1Document4 pagespmTFP1 Elp1AlleleBiotechNo ratings yet
- Dosage CardDocument2 pagesDosage CardKleibert Maciel100% (1)
- pmTFP1 VSV GDocument4 pagespmTFP1 VSV GAlleleBiotechNo ratings yet
- Realizing Precision Timing With The MSP430Document40 pagesRealizing Precision Timing With The MSP430anon_312676694No ratings yet
- GPM6A Research PaperDocument7 pagesGPM6A Research PaperRida ArifNo ratings yet
- Biokinetic of Tc99m-TetrofosminDocument7 pagesBiokinetic of Tc99m-TetrofosminKhairul AimanNo ratings yet
- 09 The aminoglycoside antibioticsDocument27 pages09 The aminoglycoside antibioticsAYAT NOFALNo ratings yet
- BFM 2002 Supplemental - Tables - JCO.2013.48.6522Document7 pagesBFM 2002 Supplemental - Tables - JCO.2013.48.6522erickmattosNo ratings yet
- Technique Chart Const-JSDocument6 pagesTechnique Chart Const-JSNumdaNo ratings yet
- pmTFP1 Cx26Document4 pagespmTFP1 Cx26AlleleBiotechNo ratings yet
- J Nucl Med-1991-Hung-2162-8 MIBI PreparacionDocument8 pagesJ Nucl Med-1991-Hung-2162-8 MIBI PreparacionJuliana CasalyNo ratings yet
- AN12626Document31 pagesAN12626James Andy CNo ratings yet
- 107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2Document4 pages107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2ft84nzzc92No ratings yet
- 280299-001 LHC0009MDocument3 pages280299-001 LHC0009MSamantha YongNo ratings yet
- pmTFP1 VinculinDocument5 pagespmTFP1 VinculinAlleleBiotechNo ratings yet
- 04QTDocument40 pages04QTSergio MontesNo ratings yet
- pmTFP1 ZyxinDocument5 pagespmTFP1 ZyxinAlleleBiotechNo ratings yet
- LCD MicrochipDocument40 pagesLCD Microchipgorea_grigNo ratings yet
- Noncompartmental Analysis: Deficiencies of Compartmental AnalysisDocument51 pagesNoncompartmental Analysis: Deficiencies of Compartmental Analysisshripathyd1No ratings yet
- Torsades de Pointes: Josh FarkasDocument8 pagesTorsades de Pointes: Josh FarkasnurhidayahNo ratings yet
- Axcent Cetus x12 Brochure en 0120Document6 pagesAxcent Cetus x12 Brochure en 0120Shaif ZahrahNo ratings yet
- 2.postoperative Arrhythmias in Open-Heart SurgeryDocument9 pages2.postoperative Arrhythmias in Open-Heart Surgeryganda gandaNo ratings yet
- Total XVDocument8 pagesTotal XVMohammed HaiderNo ratings yet
- 1995 - NAR - Solid-Phase Revesible Immobilization For The Isolation of PCR ProductsDocument2 pages1995 - NAR - Solid-Phase Revesible Immobilization For The Isolation of PCR ProductsKhoa NguyendangNo ratings yet
- QCLightning ManualDocument19 pagesQCLightning Manualrob burrNo ratings yet
- Protocol 00001947man Hcytomag-60kDocument32 pagesProtocol 00001947man Hcytomag-60kFrancisco SiirNo ratings yet
- American J Hematol - 2023 - JoinerDocument4 pagesAmerican J Hematol - 2023 - Joinersalman mehriNo ratings yet
- Cytokine, Magnetic, Panel - 2013 - Human Cytokine Chemokine Magnetic Bead Panel 96 Well Plate AssayDocument30 pagesCytokine, Magnetic, Panel - 2013 - Human Cytokine Chemokine Magnetic Bead Panel 96 Well Plate AssayEduardo SandovalNo ratings yet
- An4364 PDFDocument34 pagesAn4364 PDFjoseluisblanco69No ratings yet
- V003supp PDFDocument3 pagesV003supp PDFR-win PrawirodiharjoNo ratings yet
- Quikchange Site-Directed Mutagenesis Kit: Instruction ManualDocument20 pagesQuikchange Site-Directed Mutagenesis Kit: Instruction ManualMatthew MancusoNo ratings yet
- Advances in The Diagnosis and Treatment of ThrombocytopeniaDocument50 pagesAdvances in The Diagnosis and Treatment of ThrombocytopeniaLetnanCapungNo ratings yet
- NXP CommunicatorDocument6 pagesNXP Communicator123No ratings yet
- Genotype - Accupower Jak2Document34 pagesGenotype - Accupower Jak2Elvan Dwi WidyadiNo ratings yet
- REFERENCE Kintex 7 Rad Complete ReportDocument39 pagesREFERENCE Kintex 7 Rad Complete Reportfarzian1No ratings yet
- Icd 10 Up-Date 2010Document66 pagesIcd 10 Up-Date 2010adyaNo ratings yet
- 2019 nCoVmanual20200217 enDocument16 pages2019 nCoVmanual20200217 ensekharurlaNo ratings yet
- Dspic PDFDocument530 pagesDspic PDFmester1025No ratings yet
- pmTFP1 ActinDocument4 pagespmTFP1 ActinAlleleBiotechNo ratings yet
- Multiplex Primers Probes PrinterDocument3 pagesMultiplex Primers Probes PrinterFlavio AlvesNo ratings yet
- NXP CommunicatorDocument7 pagesNXP CommunicatorIonut37No ratings yet
- 39900article - Paper - Àlex CalleDocument10 pages39900article - Paper - Àlex Calle河井伸哉No ratings yet
- Gerontologic Nursing 6th EditionDocument61 pagesGerontologic Nursing 6th Editionjulie.navas368100% (52)
- Brochure - Zoonotic Disease Workshop - FinalDocument1 pageBrochure - Zoonotic Disease Workshop - FinalAbhipsa PradhanNo ratings yet
- PALS (Pediatric Advanced Life Support)Document48 pagesPALS (Pediatric Advanced Life Support)Jackson HakimNo ratings yet
- NCP ScoliosisDocument4 pagesNCP ScoliosisCharley DegamoNo ratings yet
- PPI VIP Graha Medika AgustusDocument208 pagesPPI VIP Graha Medika AgustusfirasyauqiNo ratings yet
- The Goal of Water4LifeDocument10 pagesThe Goal of Water4LifeHuiYingNo ratings yet
- A Case of Multiple Cranial Nerves Palsy Post ElectrocutionDocument4 pagesA Case of Multiple Cranial Nerves Palsy Post ElectrocutionEditor IJTSRDNo ratings yet
- Meropenem - Drug Information - UpToDate-2Document8 pagesMeropenem - Drug Information - UpToDate-2Vh TRNo ratings yet
- Study of Clinical, Biochemical Evaluation and Outcome in Hypertrophic Pyloric StenosisDocument4 pagesStudy of Clinical, Biochemical Evaluation and Outcome in Hypertrophic Pyloric StenosiszapomannNo ratings yet
- 10-OBGYN-Glory GroupDocument46 pages10-OBGYN-Glory Groupanmar alkhudhriNo ratings yet
- 1.3.+delusions+ +hallucinationsDocument22 pages1.3.+delusions+ +hallucinationsAna P UCAMNo ratings yet
- WEEK 7-PS M6 CU6 - Care of Clients With Schizophrenia and Related DisordersDocument12 pagesWEEK 7-PS M6 CU6 - Care of Clients With Schizophrenia and Related DisordersMaica LectanaNo ratings yet
- Laboratory - 1 - G4 StatisticsDocument16 pagesLaboratory - 1 - G4 StatisticsJENNEFER LEENo ratings yet
- Homeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Document21 pagesHomeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Yuldash100% (2)
- (Advances in Behavioral Biology 50) Olivier Dulac (Auth.), Isabelle Jambaqué, Maryse Lassonde, Olivier Dulac (Eds.) - Neuropsychology of Childhood Epilepsy (2002, Springer US)Document305 pages(Advances in Behavioral Biology 50) Olivier Dulac (Auth.), Isabelle Jambaqué, Maryse Lassonde, Olivier Dulac (Eds.) - Neuropsychology of Childhood Epilepsy (2002, Springer US)Vanez SusanibarNo ratings yet
- Healing Quantum Codes Códigos de Sanación Cuántica 1 - 5006236209752572132Document47 pagesHealing Quantum Codes Códigos de Sanación Cuántica 1 - 5006236209752572132Húgo PereiraNo ratings yet
- What's The Difference Between A Cold, The Flu, Seasonal Allergies, and CoronavirusDocument1 pageWhat's The Difference Between A Cold, The Flu, Seasonal Allergies, and CoronavirusManan BatraNo ratings yet
- Helmya Trauma ProtocolDocument85 pagesHelmya Trauma ProtocolAhmed ShehataNo ratings yet
- The Diagnostic Accuracy of Kernig's Sign, Brudzinski's Sign, and Nuchal Rigidity in Adults With Suspected MeningitisDocument7 pagesThe Diagnostic Accuracy of Kernig's Sign, Brudzinski's Sign, and Nuchal Rigidity in Adults With Suspected MeningitisNeymarNo ratings yet
- 3.0HEPATIT Lecture 5Document48 pages3.0HEPATIT Lecture 5Jiya MuhammadNo ratings yet
- Cog PsychDocument22 pagesCog PsychJoy Ann Corpuz GanadosNo ratings yet
- Australian Dental Journal - 2020 - Beaumont - Temporomandibular Disorder A Practical Guide For Dental Practitioners inDocument9 pagesAustralian Dental Journal - 2020 - Beaumont - Temporomandibular Disorder A Practical Guide For Dental Practitioners ingermanNo ratings yet
- NCM 117J (Maladaptive Pattern of Behavior) : Overview of Psychiatric Mental Health Nursing Module 1/7Document41 pagesNCM 117J (Maladaptive Pattern of Behavior) : Overview of Psychiatric Mental Health Nursing Module 1/7Abdelmar Susulan100% (1)
- Free Apo Psych Final Coaching Nov 2023 PDF PresentationDocument124 pagesFree Apo Psych Final Coaching Nov 2023 PDF PresentationsheynmalubayNo ratings yet
- Catch-22 by Joseph Heller Joseph Heller Biography: His Life and TimesDocument56 pagesCatch-22 by Joseph Heller Joseph Heller Biography: His Life and TimesAll DocumentsNo ratings yet
- CHN & NCDDocument92 pagesCHN & NCDlorelie asisNo ratings yet
- De La Salle Medical and Health Sciences InstituteDocument108 pagesDe La Salle Medical and Health Sciences InstituteJericho Daniel IgdanesNo ratings yet
- Feil & Filippi. EnglishDocument6 pagesFeil & Filippi. EnglishRia Utami Yuliani RiyutNo ratings yet
- CC1 Trans ProteinsDocument7 pagesCC1 Trans Proteinschayiezen0301No ratings yet