Download as pdf or txt
You might also like
- Depathologizing Psychopathology The Neuroscience of Mental Illness and Its TreatmentDocument185 pagesDepathologizing Psychopathology The Neuroscience of Mental Illness and Its TreatmentBreno Costa100% (1)
- Alzheimer's DiseaseDocument22 pagesAlzheimer's DiseaseSagar GavankarNo ratings yet
- Pharmacotherapy of Alzheimers DiseaseDocument69 pagesPharmacotherapy of Alzheimers DiseaseCAROL ANN PATITICONo ratings yet
- c32d9117 1591958900298Document39 pagesc32d9117 1591958900298Marzi MdvNo ratings yet
- Pharmacology Neuromuscular DisordersDocument4 pagesPharmacology Neuromuscular Disorders8dxf5bqv6gNo ratings yet
- 2010 (Chapter19 Final) Epilepsies 2Document20 pages2010 (Chapter19 Final) Epilepsies 2Candilicious10No ratings yet
- Pharmacology SGL 1 Introduction To The Pharmacology of CNS DrugsDocument28 pagesPharmacology SGL 1 Introduction To The Pharmacology of CNS DrugsNwa BradostNo ratings yet
- Cns Pharmacology For Pc-IIDocument135 pagesCns Pharmacology For Pc-IItinsaeworkineh976No ratings yet
- Parkinsonism FinalDocument54 pagesParkinsonism FinalvijayNo ratings yet
- Lecture 2 DepressionDocument26 pagesLecture 2 Depressionammarr44776No ratings yet
- Drugs For Alzheimer's DiseaseDocument12 pagesDrugs For Alzheimer's Diseasemaheen aurangzaibNo ratings yet
- Parkinsons DiseaseDocument3 pagesParkinsons Diseasem3d1kNo ratings yet
- 1-Obat Sistem Saraf Pusat-Parkinson Dan Alzheimer DDocument57 pages1-Obat Sistem Saraf Pusat-Parkinson Dan Alzheimer DFarhan AshsiddiqiNo ratings yet
- Pharmacology of Drugs Used in Movement Disorders: Christian WaeberDocument34 pagesPharmacology of Drugs Used in Movement Disorders: Christian WaeberciaranNo ratings yet
- Anti Epileptic Drug: Guided By: Ms Baiaineh Pyngrope Lecturer SKCN, BANGALOREDocument30 pagesAnti Epileptic Drug: Guided By: Ms Baiaineh Pyngrope Lecturer SKCN, BANGALOREhisse yonjanNo ratings yet
- Kinds of Neurodegenerative DisordersDocument4 pagesKinds of Neurodegenerative DisordersOctavius QuinNo ratings yet
- PharmTest3 StudyGuideDocument9 pagesPharmTest3 StudyGuideTara Bickford ManisNo ratings yet
- AlzheimerDocument5 pagesAlzheimerThe ChannelNo ratings yet
- NPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesDocument83 pagesNPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Drugs For Neurodegenarative DiseaesesDocument14 pagesDrugs For Neurodegenarative Diseaesesالطاهر زروقNo ratings yet
- CNS 2022Document8 pagesCNS 2022Kathleen Kate MonsalveNo ratings yet
- Sistim EkstrapiramidalDocument44 pagesSistim EkstrapiramidaljanaNo ratings yet
- Pharm 9 & 10 Movt Disorders 2022 (Student)Document72 pagesPharm 9 & 10 Movt Disorders 2022 (Student)aaronkinnear713No ratings yet
- CNS UnlockedDocument28 pagesCNS Unlockedabdoelsharkaw211No ratings yet
- Dr. Sobaryati Sepsis Associated Encephalophaty Come On FinalDocument46 pagesDr. Sobaryati Sepsis Associated Encephalophaty Come On FinalAyu WahyuniNo ratings yet
- Pharmacological Treatment: Antipsychotics: Mechanism of ActionDocument7 pagesPharmacological Treatment: Antipsychotics: Mechanism of Actionvarsha thakurNo ratings yet
- Paradoxical ReactionsDocument40 pagesParadoxical ReactionsYasmina BadrNo ratings yet
- Overview CNS Chemical TransmissionDocument75 pagesOverview CNS Chemical TransmissionsaivasyaNo ratings yet
- Lecture 8 Central Nervous System CnsDocument35 pagesLecture 8 Central Nervous System CnsakramuddaulaNo ratings yet
- Basal GangliaDocument76 pagesBasal GangliaHussain ANo ratings yet
- Toxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiDocument18 pagesToxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiVivi DeviyanaNo ratings yet
- Naidoo Lecture NoteDocument10 pagesNaidoo Lecture NoteDanny LeeNo ratings yet
- Antipsychotic Drugs - Pharmacology - An Illustrated ReviewDocument5 pagesAntipsychotic Drugs - Pharmacology - An Illustrated ReviewDragutin PetrićNo ratings yet
- 26brain Neurotransmitters-18Document39 pages26brain Neurotransmitters-18Ilobun Faithful IziengbeNo ratings yet
- Management Management: Clinical Features Clinical FeaturesDocument1 pageManagement Management: Clinical Features Clinical FeaturesKSP PatnaikNo ratings yet
- Alzheimer's DiseaseDocument9 pagesAlzheimer's Diseasejanemwanza003No ratings yet
- Fritschy Neuropharmacology FS2012Document57 pagesFritschy Neuropharmacology FS2012gugspotNo ratings yet
- Paradoxical ReactionsDocument8 pagesParadoxical ReactionsYasmina BadrNo ratings yet
- Novement Disorder EmergenciesDocument40 pagesNovement Disorder EmergenciesGamer MadaNo ratings yet
- Pharmacotherapy Handbook, 9th Ed-522-554Document33 pagesPharmacotherapy Handbook, 9th Ed-522-554kikiNo ratings yet
- Typical AntipsychoticsDocument13 pagesTypical AntipsychoticsAKASH DEEPNo ratings yet
- DementiaDocument40 pagesDementiacvmqx7yppdNo ratings yet
- PDF Wk4 Neuro 2Document10 pagesPDF Wk4 Neuro 2IssacNo ratings yet
- Mark Tuttle Neurology Clerkship Study Guide PDFDocument84 pagesMark Tuttle Neurology Clerkship Study Guide PDFDavid ChangNo ratings yet
- CNS NeurotransmitterDocument67 pagesCNS NeurotransmitterGreenNo ratings yet
- Drug StudyDocument10 pagesDrug StudyRubie Ann TillorNo ratings yet
- Neurology Clerkship Study GuideDocument84 pagesNeurology Clerkship Study GuidetaherNo ratings yet
- Epilepsy With Antiepileptic DrugsDocument58 pagesEpilepsy With Antiepileptic DrugsAyesha ZahidNo ratings yet
- DementiaDocument53 pagesDementiaDcp MbbsNo ratings yet
- 11-1-2021 Case DiscussionDocument26 pages11-1-2021 Case Discussionsrija vijjapuNo ratings yet
- MaladaptiveDocument16 pagesMaladaptiveJanely EstreraNo ratings yet
- Dementia and Neurodegenerative Disorders: Clinical ManifestationsDocument5 pagesDementia and Neurodegenerative Disorders: Clinical Manifestationsmay_74846422No ratings yet
- Antiparkinsons DrugsDocument19 pagesAntiparkinsons Drugs39 Nayan BhagatNo ratings yet
- Obat-Obat Psychiatry - 1 2018Document104 pagesObat-Obat Psychiatry - 1 2018Christo LimbongNo ratings yet
- Anti Psychotic DrugDocument25 pagesAnti Psychotic DrugANI SAMNo ratings yet
- Joana Marie E. Gantuangco: Harrison's 20th EditionDocument27 pagesJoana Marie E. Gantuangco: Harrison's 20th EditionJoana Marie Gantuangco-MaglinteNo ratings yet
- Antiparkinsonismdrugsbydr 181226084221Document70 pagesAntiparkinsonismdrugsbydr 181226084221Analiza Kitongan LantayanNo ratings yet
- HaloperidolDocument4 pagesHaloperidolKyla Barrera TabungarNo ratings yet
- Haloperidol PDFDocument4 pagesHaloperidol PDFfatimahNo ratings yet
- Autoimmune EncephalitisDocument43 pagesAutoimmune EncephalitisPrateek Kumar PandaNo ratings yet
- A170566 Study Report BodyDocument79 pagesA170566 Study Report BodyAnonymous yqRB5cVMeNo ratings yet
- Benefits of Hypnosis Author Mental Health America of Northern KentuckyDocument4 pagesBenefits of Hypnosis Author Mental Health America of Northern KentuckyJakarta SelamatNo ratings yet
- WEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestDocument6 pagesWEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestHàNhậtNguyễnNo ratings yet
- Hyperworks Technology Conference (HTC) 2011: Optimization of PMH StructuresDocument25 pagesHyperworks Technology Conference (HTC) 2011: Optimization of PMH StructuresgiakovidNo ratings yet
- National Program For Rehabilitation of Polluted Site - A Case StudyDocument4 pagesNational Program For Rehabilitation of Polluted Site - A Case StudyijeteeditorNo ratings yet
- Nurses' Knowledge Towards Severe Acute Malnutrition Management Protocol and Its Associated FactorsDocument10 pagesNurses' Knowledge Towards Severe Acute Malnutrition Management Protocol and Its Associated FactorsIJPHSNo ratings yet
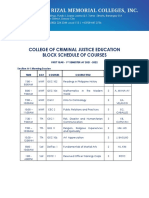
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- BERSHAM AND ADWY GIRLS SCHOOL LOGS. Book 2 August 1889 - JANUARY 1915Document80 pagesBERSHAM AND ADWY GIRLS SCHOOL LOGS. Book 2 August 1889 - JANUARY 1915Annette EdwardsNo ratings yet
- ICO-Ophthalmology Surgical Competency Assessment Rubric-SICS (ICO-OSCAR: SICS)Document3 pagesICO-Ophthalmology Surgical Competency Assessment Rubric-SICS (ICO-OSCAR: SICS)Andi Akhmad FaisalNo ratings yet
- For DissertationDocument13 pagesFor DissertationRegi viniciyaNo ratings yet
- Managing Our Waste: Powerpoint Slides Prepared by Stephen TurnbullDocument59 pagesManaging Our Waste: Powerpoint Slides Prepared by Stephen TurnbullJulia HartNo ratings yet
- Ultrarunning MagDocument60 pagesUltrarunning MagLynseyNo ratings yet
- Local Exhaust Ventilation LEV Guidance PDFDocument72 pagesLocal Exhaust Ventilation LEV Guidance PDFJoaquim Reis100% (2)
- Thorax and Lungs Physical Assessment Includes InspectionDocument9 pagesThorax and Lungs Physical Assessment Includes InspectionwiwinNo ratings yet
- Post Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MDocument3 pagesPost Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MLyca Mae AurelioNo ratings yet
- Hospital PharmacyDocument14 pagesHospital PharmacyAbigael PescasioNo ratings yet
- Your AnswersDocument5 pagesYour AnswersHa TranNo ratings yet
- The Results of MasturbationDocument1 pageThe Results of MasturbationAkash DeepNo ratings yet
- 21 2023 ICTP QA ProgrammeDocument54 pages21 2023 ICTP QA ProgrammeBui Duy LinhNo ratings yet
- Punctate: NumberDocument6 pagesPunctate: NumberMuhamad Chairul SyahNo ratings yet
- Helping Children With Learning DisabilitiesDocument10 pagesHelping Children With Learning DisabilitiesUni KartikasariNo ratings yet
- Green Light Surgical GuideDocument88 pagesGreen Light Surgical GuidekbrinaldiNo ratings yet
- Prevention & Management of Sports Injuries: Quimcy Dsouza Fybms-Sm (B) 75Document26 pagesPrevention & Management of Sports Injuries: Quimcy Dsouza Fybms-Sm (B) 75Quimcy100% (1)
- The Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateDocument5 pagesThe Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateManuel Guerrero GómezNo ratings yet
- Cowan 1999Document20 pagesCowan 1999ggggggggggg32No ratings yet
- Health ServicesDocument3 pagesHealth ServicesReizza Mae NecesitoNo ratings yet
- 5X5 Intermediate - Bill StarrDocument7 pages5X5 Intermediate - Bill StarrAfrican MastiffNo ratings yet
- Admission: Athia Fidian, M.PDDocument6 pagesAdmission: Athia Fidian, M.PDAthiaNo ratings yet
- IELTS Writing Task 2 Samples (WWW - Luckyielts.com) PDFDocument648 pagesIELTS Writing Task 2 Samples (WWW - Luckyielts.com) PDFMinh NgọcNo ratings yet