
Arc Als Guides
Arc Als Guides
You might also like
- AHA ACLS Megacode Scenarios PDFDocument6 pagesAHA ACLS Megacode Scenarios PDFNavin ShawnNo ratings yet
- TLS 3 Day Workout RoutineDocument14 pagesTLS 3 Day Workout RoutineamberNo ratings yet
- Nursing Care Plan For Palliative Care Nursing NotesDocument2 pagesNursing Care Plan For Palliative Care Nursing NotesblaireNo ratings yet
- Types of Assisted VentilationDocument1 pageTypes of Assisted VentilationJerry G100% (3)
- ACLS Megacode Testing ScenariosDocument12 pagesACLS Megacode Testing Scenariosealm10100% (2)
- Advanced Cardiac ArrestDocument1 pageAdvanced Cardiac ArrestDebbie MeyerNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Pamet and PasmethDocument4 pagesPamet and PasmethBash De Guzman50% (2)
- v723 6986675 SM 4-10 (Full Permission) - UnprotectedDocument913 pagesv723 6986675 SM 4-10 (Full Permission) - UnprotectedAaron VanceNo ratings yet
- All India 20 Crore Database SampleDocument304 pagesAll India 20 Crore Database SampleVikram100% (1)
- Procedure TextDocument4 pagesProcedure TextIrfanuddin MudzakiNo ratings yet
- Effect of PH and Temperature On Enzyma Activity Formal ReportDocument5 pagesEffect of PH and Temperature On Enzyma Activity Formal ReportAshNo ratings yet
- ALS Code Card - Adult Systematic AssessmentDocument1 pageALS Code Card - Adult Systematic AssessmentphoxxyNo ratings yet
- BLS Code Card - Basic Life Support Adults and AdolescentsDocument2 pagesBLS Code Card - Basic Life Support Adults and AdolescentsphuongNo ratings yet
- BLS Code Card - Basic Life Support Children and InfantsDocument2 pagesBLS Code Card - Basic Life Support Children and InfantsphuongNo ratings yet
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDocument7 pagesIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaNo ratings yet
- Course Task Week 7 Fluid ImbalancesDocument6 pagesCourse Task Week 7 Fluid ImbalancesNathan MielNo ratings yet
- Intravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid StatusDocument13 pagesIntravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid Statusfernin96No ratings yet
- Acls Algorithms Acls Algorithms: (Cardiac Arrest) (Bradycardia) Assessment ActionDocument5 pagesAcls Algorithms Acls Algorithms: (Cardiac Arrest) (Bradycardia) Assessment ActionCabales EmmanNo ratings yet
- Card ACLSDocument2 pagesCard ACLSSaman FirdousNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- Website Tachycardia Algorithm DiagramDocument1 pageWebsite Tachycardia Algorithm Diagramcolette zgheibNo ratings yet
- AlgorithmsDocument16 pagesAlgorithmsirish laglevaNo ratings yet
- Pediatric Tachycardia With A Pulse Algorithm: Yes NoDocument1 pagePediatric Tachycardia With A Pulse Algorithm: Yes NoRatna TambaNo ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- SepsisDocument10 pagesSepsisJessa MaeNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Adenosine 8-28-22Document1 pageAdenosine 8-28-22ladawskiNo ratings yet
- CBR Midterms: Assessment of Vital Signs Key TermsDocument4 pagesCBR Midterms: Assessment of Vital Signs Key TermsFlint RockNo ratings yet
- 11 Care of The CV Surgery Patient EmilDocument2 pages11 Care of The CV Surgery Patient EmilameliajamirusNo ratings yet
- PALS Practice 1 Hypovolemic ShockDocument64 pagesPALS Practice 1 Hypovolemic ShockGlen LazarusNo ratings yet
- Caro NCPDocument17 pagesCaro NCPAbegail PolicarpioNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612must dietNo ratings yet
- Haemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareDocument7 pagesHaemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareClaudia IsabelNo ratings yet
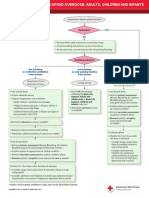
- CC Opioid OverdoseDocument1 pageCC Opioid Overdosestarskyhutch0000No ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- L8 9 Cardiac Fluids Disorders in ChildrenDocument17 pagesL8 9 Cardiac Fluids Disorders in ChildrenRose Anne AbivaNo ratings yet
- 2492 AAP RCUK Algorithms-26 1 - AIHCADocument1 page2492 AAP RCUK Algorithms-26 1 - AIHCAGayani UdayangaNo ratings yet
- Atrial Fibrillation: Key TreatmentsDocument2 pagesAtrial Fibrillation: Key TreatmentschoobiNo ratings yet
- Critical Care - Hemodynamic Monitoring TableDocument7 pagesCritical Care - Hemodynamic Monitoring TableVictoria Romero100% (2)
- Nursing Care Plan Related To Pospartum HemmorhageDocument5 pagesNursing Care Plan Related To Pospartum HemmorhageAsmin BalahNo ratings yet
- Norepinephrine FinalDocument2 pagesNorepinephrine FinalNelly CruzNo ratings yet
- Algorithms of AHA 2020Document23 pagesAlgorithms of AHA 2020Emirhan llkhanNo ratings yet
- Decreased Cardiac Output RT HypertensionDocument3 pagesDecreased Cardiac Output RT Hypertensionjessa maeNo ratings yet
- Веб-страница 2Document1 pageВеб-страница 2Zalina IvanovaNo ratings yet
- Post Arrest CareDocument23 pagesPost Arrest CareMohamed RasoolNo ratings yet
- Wa0080.Document2 pagesWa0080.eee83353No ratings yet
- 8-Suspected Stroke AlgrthmDocument1 page8-Suspected Stroke AlgrthmterminallllNo ratings yet
- 2020 Acls Megacode Testing Scenarios - 2Document13 pages2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNo ratings yet
- BEC Module 1 Part 1Document26 pagesBEC Module 1 Part 1colorred818No ratings yet
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdNo ratings yet
- S T A R T: Imple Riage ND Apid ReatmentDocument17 pagesS T A R T: Imple Riage ND Apid ReatmentNavine NavNo ratings yet
- ILS 2014 Final Year Revision LectureDocument54 pagesILS 2014 Final Year Revision Lectureunstoppable jionNo ratings yet
- Day 3Document31 pagesDay 3Sara AlramdhanNo ratings yet
- Pulmonary EmbolismDocument2 pagesPulmonary EmbolismAnjana BasilNo ratings yet
- Microsoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1Document23 pagesMicrosoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1api-19824701100% (1)
- C19 SPACE ToolKit ChecklistsDocument8 pagesC19 SPACE ToolKit ChecklistsAdrian BălanNo ratings yet
- Marcos Er NCPDocument1 pageMarcos Er NCPAssasination ClassroomNo ratings yet
- Central Venous Pressure Monitoring: Assisting With CVP PlacementDocument3 pagesCentral Venous Pressure Monitoring: Assisting With CVP PlacementGlare RhayneNo ratings yet
- Damage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and CorpsmenDocument1 pageDamage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and Corpsmenchou youNo ratings yet
- طوارئDocument9 pagesطوارئbestmsaasNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- NCP HyperthermiaDocument2 pagesNCP HyperthermiaKirby ContaoiNo ratings yet
- Aha Acls GuideDocument11 pagesAha Acls GuideIrene PimentelNo ratings yet
- Guide To Caring For Acutely Ill Patients For Non Critical Care Staff in An Emergency SituationDocument29 pagesGuide To Caring For Acutely Ill Patients For Non Critical Care Staff in An Emergency Situationmy dreamNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Final Paper 1Document27 pagesFinal Paper 1api-315734227No ratings yet
- Fruit Juice BusinessDocument2 pagesFruit Juice BusinessRiddhi ShahNo ratings yet
- A - Two-Stage - Isolated - Resonant - DC-DC - Converter - For - Wide - Voltage - Range - OperationDocument6 pagesA - Two-Stage - Isolated - Resonant - DC-DC - Converter - For - Wide - Voltage - Range - OperationMahad NadeemNo ratings yet
- Trouble Diagnosis Circuit Diagram: (QG (With Euro-Obd) )Document18 pagesTrouble Diagnosis Circuit Diagram: (QG (With Euro-Obd) )Electronicdeivi DeiviNo ratings yet
- BRC Food Issue 7 Audit ChecklistDocument4 pagesBRC Food Issue 7 Audit ChecklistGlobal Manager Group0% (1)
- Alpha Series MotorDocument274 pagesAlpha Series MotorSri KrishNo ratings yet
- Spice List 20121Document2 pagesSpice List 20121ravivarmahyd8173No ratings yet
- OrmaxDocument26 pagesOrmaxNandini GoyalNo ratings yet
- 2019-11 Hydrocarbon EngineeringDocument92 pages2019-11 Hydrocarbon Engineeringjdgh1986No ratings yet
- TLE Worksheets Carpentry 7 and 8 Q3Document2 pagesTLE Worksheets Carpentry 7 and 8 Q3Xyra Zheniel PerezNo ratings yet
- Literary Criticsm The Greatest ShowmanDocument10 pagesLiterary Criticsm The Greatest ShowmanZafira MalikNo ratings yet
- 816 2328 1 SM PDFDocument4 pages816 2328 1 SM PDFRahki BhatiNo ratings yet
- Coronavirus FutureDocument110 pagesCoronavirus FutureAngelicaNo ratings yet
- The Opportunities of Lithium in Thermal Energy Storage: A State-Of-The-Art ReviewDocument24 pagesThe Opportunities of Lithium in Thermal Energy Storage: A State-Of-The-Art ReviewFrancisco DazaNo ratings yet
- Psych BulletsDocument16 pagesPsych BulletsPrince Rener Velasco PeraNo ratings yet
- Essa Sampling Systems: Engineered Representative Sampling SolutionsDocument3 pagesEssa Sampling Systems: Engineered Representative Sampling SolutionsMilan SjausNo ratings yet
- LP Askep Keluarga Gouth AthritisDocument50 pagesLP Askep Keluarga Gouth AthritisSeptyari100% (3)
- TM9 1755BB EngineDocument331 pagesTM9 1755BB EngineAmiVolatNo ratings yet
- TP2 24 AprilDocument12 pagesTP2 24 AprilAnaSlavovaNo ratings yet
- School Library System An OverviewDocument1 pageSchool Library System An OverviewAbid HussainNo ratings yet
- E-Registration Presentation - 10APR2019Document137 pagesE-Registration Presentation - 10APR2019Joshua RingorNo ratings yet
- 13-Incident Investigation and Corrective ActionREVISED PDFDocument56 pages13-Incident Investigation and Corrective ActionREVISED PDFSafiuddin Afdal LaudinNo ratings yet
- Section: Section:: Student's Information Student's InformationDocument1 pageSection: Section:: Student's Information Student's InformationMello Jane Garcia DedosinNo ratings yet
- Health Risk Assessments: Opportunities and Pitfalls: Common Errors Relating To EnvironmentalDocument32 pagesHealth Risk Assessments: Opportunities and Pitfalls: Common Errors Relating To EnvironmentalOmar HeshamNo ratings yet
























































































Download as pdf or txt
You might also like
- AHA ACLS Megacode Scenarios PDFDocument6 pagesAHA ACLS Megacode Scenarios PDFNavin ShawnNo ratings yet
- TLS 3 Day Workout RoutineDocument14 pagesTLS 3 Day Workout RoutineamberNo ratings yet
- Nursing Care Plan For Palliative Care Nursing NotesDocument2 pagesNursing Care Plan For Palliative Care Nursing NotesblaireNo ratings yet
- Types of Assisted VentilationDocument1 pageTypes of Assisted VentilationJerry G100% (3)
- ACLS Megacode Testing ScenariosDocument12 pagesACLS Megacode Testing Scenariosealm10100% (2)
- Advanced Cardiac ArrestDocument1 pageAdvanced Cardiac ArrestDebbie MeyerNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Pamet and PasmethDocument4 pagesPamet and PasmethBash De Guzman50% (2)
- v723 6986675 SM 4-10 (Full Permission) - UnprotectedDocument913 pagesv723 6986675 SM 4-10 (Full Permission) - UnprotectedAaron VanceNo ratings yet
- All India 20 Crore Database SampleDocument304 pagesAll India 20 Crore Database SampleVikram100% (1)
- Procedure TextDocument4 pagesProcedure TextIrfanuddin MudzakiNo ratings yet
- Effect of PH and Temperature On Enzyma Activity Formal ReportDocument5 pagesEffect of PH and Temperature On Enzyma Activity Formal ReportAshNo ratings yet
- ALS Code Card - Adult Systematic AssessmentDocument1 pageALS Code Card - Adult Systematic AssessmentphoxxyNo ratings yet
- BLS Code Card - Basic Life Support Adults and AdolescentsDocument2 pagesBLS Code Card - Basic Life Support Adults and AdolescentsphuongNo ratings yet
- BLS Code Card - Basic Life Support Children and InfantsDocument2 pagesBLS Code Card - Basic Life Support Children and InfantsphuongNo ratings yet
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDocument7 pagesIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaNo ratings yet
- Course Task Week 7 Fluid ImbalancesDocument6 pagesCourse Task Week 7 Fluid ImbalancesNathan MielNo ratings yet
- Intravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid StatusDocument13 pagesIntravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid Statusfernin96No ratings yet
- Acls Algorithms Acls Algorithms: (Cardiac Arrest) (Bradycardia) Assessment ActionDocument5 pagesAcls Algorithms Acls Algorithms: (Cardiac Arrest) (Bradycardia) Assessment ActionCabales EmmanNo ratings yet
- Card ACLSDocument2 pagesCard ACLSSaman FirdousNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- Website Tachycardia Algorithm DiagramDocument1 pageWebsite Tachycardia Algorithm Diagramcolette zgheibNo ratings yet
- AlgorithmsDocument16 pagesAlgorithmsirish laglevaNo ratings yet
- Pediatric Tachycardia With A Pulse Algorithm: Yes NoDocument1 pagePediatric Tachycardia With A Pulse Algorithm: Yes NoRatna TambaNo ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- SepsisDocument10 pagesSepsisJessa MaeNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Adenosine 8-28-22Document1 pageAdenosine 8-28-22ladawskiNo ratings yet
- CBR Midterms: Assessment of Vital Signs Key TermsDocument4 pagesCBR Midterms: Assessment of Vital Signs Key TermsFlint RockNo ratings yet
- 11 Care of The CV Surgery Patient EmilDocument2 pages11 Care of The CV Surgery Patient EmilameliajamirusNo ratings yet
- PALS Practice 1 Hypovolemic ShockDocument64 pagesPALS Practice 1 Hypovolemic ShockGlen LazarusNo ratings yet
- Caro NCPDocument17 pagesCaro NCPAbegail PolicarpioNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612must dietNo ratings yet
- Haemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareDocument7 pagesHaemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareClaudia IsabelNo ratings yet
- CC Opioid OverdoseDocument1 pageCC Opioid Overdosestarskyhutch0000No ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- L8 9 Cardiac Fluids Disorders in ChildrenDocument17 pagesL8 9 Cardiac Fluids Disorders in ChildrenRose Anne AbivaNo ratings yet
- 2492 AAP RCUK Algorithms-26 1 - AIHCADocument1 page2492 AAP RCUK Algorithms-26 1 - AIHCAGayani UdayangaNo ratings yet
- Atrial Fibrillation: Key TreatmentsDocument2 pagesAtrial Fibrillation: Key TreatmentschoobiNo ratings yet
- Critical Care - Hemodynamic Monitoring TableDocument7 pagesCritical Care - Hemodynamic Monitoring TableVictoria Romero100% (2)
- Nursing Care Plan Related To Pospartum HemmorhageDocument5 pagesNursing Care Plan Related To Pospartum HemmorhageAsmin BalahNo ratings yet
- Norepinephrine FinalDocument2 pagesNorepinephrine FinalNelly CruzNo ratings yet
- Algorithms of AHA 2020Document23 pagesAlgorithms of AHA 2020Emirhan llkhanNo ratings yet
- Decreased Cardiac Output RT HypertensionDocument3 pagesDecreased Cardiac Output RT Hypertensionjessa maeNo ratings yet
- Веб-страница 2Document1 pageВеб-страница 2Zalina IvanovaNo ratings yet
- Post Arrest CareDocument23 pagesPost Arrest CareMohamed RasoolNo ratings yet
- Wa0080.Document2 pagesWa0080.eee83353No ratings yet
- 8-Suspected Stroke AlgrthmDocument1 page8-Suspected Stroke AlgrthmterminallllNo ratings yet
- 2020 Acls Megacode Testing Scenarios - 2Document13 pages2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNo ratings yet
- BEC Module 1 Part 1Document26 pagesBEC Module 1 Part 1colorred818No ratings yet
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdNo ratings yet
- S T A R T: Imple Riage ND Apid ReatmentDocument17 pagesS T A R T: Imple Riage ND Apid ReatmentNavine NavNo ratings yet
- ILS 2014 Final Year Revision LectureDocument54 pagesILS 2014 Final Year Revision Lectureunstoppable jionNo ratings yet
- Day 3Document31 pagesDay 3Sara AlramdhanNo ratings yet
- Pulmonary EmbolismDocument2 pagesPulmonary EmbolismAnjana BasilNo ratings yet
- Microsoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1Document23 pagesMicrosoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1api-19824701100% (1)
- C19 SPACE ToolKit ChecklistsDocument8 pagesC19 SPACE ToolKit ChecklistsAdrian BălanNo ratings yet
- Marcos Er NCPDocument1 pageMarcos Er NCPAssasination ClassroomNo ratings yet
- Central Venous Pressure Monitoring: Assisting With CVP PlacementDocument3 pagesCentral Venous Pressure Monitoring: Assisting With CVP PlacementGlare RhayneNo ratings yet
- Damage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and CorpsmenDocument1 pageDamage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and Corpsmenchou youNo ratings yet
- طوارئDocument9 pagesطوارئbestmsaasNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- NCP HyperthermiaDocument2 pagesNCP HyperthermiaKirby ContaoiNo ratings yet
- Aha Acls GuideDocument11 pagesAha Acls GuideIrene PimentelNo ratings yet
- Guide To Caring For Acutely Ill Patients For Non Critical Care Staff in An Emergency SituationDocument29 pagesGuide To Caring For Acutely Ill Patients For Non Critical Care Staff in An Emergency Situationmy dreamNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Final Paper 1Document27 pagesFinal Paper 1api-315734227No ratings yet
- Fruit Juice BusinessDocument2 pagesFruit Juice BusinessRiddhi ShahNo ratings yet
- A - Two-Stage - Isolated - Resonant - DC-DC - Converter - For - Wide - Voltage - Range - OperationDocument6 pagesA - Two-Stage - Isolated - Resonant - DC-DC - Converter - For - Wide - Voltage - Range - OperationMahad NadeemNo ratings yet
- Trouble Diagnosis Circuit Diagram: (QG (With Euro-Obd) )Document18 pagesTrouble Diagnosis Circuit Diagram: (QG (With Euro-Obd) )Electronicdeivi DeiviNo ratings yet
- BRC Food Issue 7 Audit ChecklistDocument4 pagesBRC Food Issue 7 Audit ChecklistGlobal Manager Group0% (1)
- Alpha Series MotorDocument274 pagesAlpha Series MotorSri KrishNo ratings yet
- Spice List 20121Document2 pagesSpice List 20121ravivarmahyd8173No ratings yet
- OrmaxDocument26 pagesOrmaxNandini GoyalNo ratings yet
- 2019-11 Hydrocarbon EngineeringDocument92 pages2019-11 Hydrocarbon Engineeringjdgh1986No ratings yet
- TLE Worksheets Carpentry 7 and 8 Q3Document2 pagesTLE Worksheets Carpentry 7 and 8 Q3Xyra Zheniel PerezNo ratings yet
- Literary Criticsm The Greatest ShowmanDocument10 pagesLiterary Criticsm The Greatest ShowmanZafira MalikNo ratings yet
- 816 2328 1 SM PDFDocument4 pages816 2328 1 SM PDFRahki BhatiNo ratings yet
- Coronavirus FutureDocument110 pagesCoronavirus FutureAngelicaNo ratings yet
- The Opportunities of Lithium in Thermal Energy Storage: A State-Of-The-Art ReviewDocument24 pagesThe Opportunities of Lithium in Thermal Energy Storage: A State-Of-The-Art ReviewFrancisco DazaNo ratings yet
- Psych BulletsDocument16 pagesPsych BulletsPrince Rener Velasco PeraNo ratings yet
- Essa Sampling Systems: Engineered Representative Sampling SolutionsDocument3 pagesEssa Sampling Systems: Engineered Representative Sampling SolutionsMilan SjausNo ratings yet
- LP Askep Keluarga Gouth AthritisDocument50 pagesLP Askep Keluarga Gouth AthritisSeptyari100% (3)
- TM9 1755BB EngineDocument331 pagesTM9 1755BB EngineAmiVolatNo ratings yet
- TP2 24 AprilDocument12 pagesTP2 24 AprilAnaSlavovaNo ratings yet
- School Library System An OverviewDocument1 pageSchool Library System An OverviewAbid HussainNo ratings yet
- E-Registration Presentation - 10APR2019Document137 pagesE-Registration Presentation - 10APR2019Joshua RingorNo ratings yet
- 13-Incident Investigation and Corrective ActionREVISED PDFDocument56 pages13-Incident Investigation and Corrective ActionREVISED PDFSafiuddin Afdal LaudinNo ratings yet
- Section: Section:: Student's Information Student's InformationDocument1 pageSection: Section:: Student's Information Student's InformationMello Jane Garcia DedosinNo ratings yet
- Health Risk Assessments: Opportunities and Pitfalls: Common Errors Relating To EnvironmentalDocument32 pagesHealth Risk Assessments: Opportunities and Pitfalls: Common Errors Relating To EnvironmentalOmar HeshamNo ratings yet