Download as pdf or txt
You might also like
- IntelliVue Information Center HL7 Programmer S Guide PDFDocument210 pagesIntelliVue Information Center HL7 Programmer S Guide PDFhugutuxNo ratings yet
- Executive Coaching Workbook PDFDocument19 pagesExecutive Coaching Workbook PDFDiego Fortes100% (4)
- Boeing 737-300 Transit CheckDocument6 pagesBoeing 737-300 Transit CheckUmer JavedNo ratings yet
- FM - Ag 08 - TP 088 3Document64 pagesFM - Ag 08 - TP 088 3cmpmarinhoNo ratings yet
- Trisomy 21 Fetus Co-Existent With A Partial Molar Pregnancy: Case ReportDocument2 pagesTrisomy 21 Fetus Co-Existent With A Partial Molar Pregnancy: Case ReportArga KafiNo ratings yet
- Inguinal Hernia in Preterm Infants ( 32-Week Gestation) : Original ArticleDocument7 pagesInguinal Hernia in Preterm Infants ( 32-Week Gestation) : Original ArticleBlank SpaceNo ratings yet
- Successful Maternal and Fetal Outcome of Guillain-Barre Syndrome Complicating Pregnancy: A Case ReportDocument2 pagesSuccessful Maternal and Fetal Outcome of Guillain-Barre Syndrome Complicating Pregnancy: A Case ReportmelvaNo ratings yet
- Torch Infection and Its Management With Ayurveda, An Indigenous MedicineDocument2 pagesTorch Infection and Its Management With Ayurveda, An Indigenous MedicineDhiraj BaksheNo ratings yet
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafNo ratings yet
- Esclerosis y Embarazo 5Document2 pagesEsclerosis y Embarazo 5povadicNo ratings yet
- Interesting Case Precocious - EditedDocument17 pagesInteresting Case Precocious - EditedSherilyn Joy AdelNo ratings yet
- Management of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineDocument10 pagesManagement of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineimeldahermnNo ratings yet
- Less Is More Modern NeonatologyDocument11 pagesLess Is More Modern NeonatologyEN BUNo ratings yet
- CRP Pregnancy Cohen 2014Document4 pagesCRP Pregnancy Cohen 2014samiNo ratings yet
- COVID-19 Vaccination During Pregnancy: Coverage and Safety: ObstetricsDocument14 pagesCOVID-19 Vaccination During Pregnancy: Coverage and Safety: ObstetricsErik SusantoNo ratings yet
- Placental Abruption in Term and Preterm.8 PDFDocument8 pagesPlacental Abruption in Term and Preterm.8 PDFMuhammad Riza FahlawiNo ratings yet
- Assessment of Pregnancy Outcome in Primigravida: Comparison Between Booked and Un-Booked PatientsDocument3 pagesAssessment of Pregnancy Outcome in Primigravida: Comparison Between Booked and Un-Booked PatientsIndhumathiNo ratings yet
- Acute Pyelonephritis in PregnancyDocument7 pagesAcute Pyelonephritis in PregnancyKvmLlyNo ratings yet
- Dengue in Pregnancy: An Under-Reported Illness, With Special Reference To Other Existing Co-InfectionsDocument3 pagesDengue in Pregnancy: An Under-Reported Illness, With Special Reference To Other Existing Co-InfectionsLeonardoMartínezNo ratings yet
- Diagnosing Antenatal Fetal Distress: Igor Victorovich Lakhno, Kemine UzelDocument3 pagesDiagnosing Antenatal Fetal Distress: Igor Victorovich Lakhno, Kemine Uzelyenni anggrainiNo ratings yet
- Gastroschisis: Case ReportDocument2 pagesGastroschisis: Case ReportMuhammad Syamil RozlanNo ratings yet
- A Case of Successful Management of Guillainbarre Syndrome in PregnancyDocument3 pagesA Case of Successful Management of Guillainbarre Syndrome in PregnancyTias DiahNo ratings yet
- SLE and PregnancyDocument10 pagesSLE and PregnancySergio CerpaNo ratings yet
- Maternal and Perinatal Outcomes of Pregnant WomenDocument11 pagesMaternal and Perinatal Outcomes of Pregnant Womenida husenNo ratings yet
- Lack of Effects On Female Fertility and Prenatal and Postnat 2021 ReproductiDocument8 pagesLack of Effects On Female Fertility and Prenatal and Postnat 2021 ReproductiJindřich CieślickiNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- The Impact of in Utero Transfusions On Perinatal Outcomes in Patients With Alpha Thalassemia MajorDocument11 pagesThe Impact of in Utero Transfusions On Perinatal Outcomes in Patients With Alpha Thalassemia Majoraulia firdausNo ratings yet
- S - Cervical Ectopic PregnancyDocument8 pagesS - Cervical Ectopic PregnancyCitra Wahyu Tri UtamiNo ratings yet
- Fetomaternal Outcome of Pregnancy With Hepatitis E InfectionDocument4 pagesFetomaternal Outcome of Pregnancy With Hepatitis E InfectionNZ FreelancersNo ratings yet
- What Is Causing This Girl S Abdominal Pain .10Document2 pagesWhat Is Causing This Girl S Abdominal Pain .10LuisNo ratings yet
- Jurnal Internasional 3Document4 pagesJurnal Internasional 3P17312215223 LINDA ANISANo ratings yet
- Congenital Varicella Syndrome CaseDocument3 pagesCongenital Varicella Syndrome CasemirbanNo ratings yet
- Q Fever in PregnancyDocument1 pageQ Fever in Pregnancyyewha550No ratings yet
- Late Presentation of Post Diphtheritic Myocarditis in A 15-Year MaleDocument3 pagesLate Presentation of Post Diphtheritic Myocarditis in A 15-Year MaleFaqih Alam RuqmanaNo ratings yet
- A Case Report On Pregnancy With Systemic SclerosisDocument3 pagesA Case Report On Pregnancy With Systemic SclerosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pregnancy With Epilepsy - A Retrospective Analysis: Gynetology & ObstetricsDocument6 pagesPregnancy With Epilepsy - A Retrospective Analysis: Gynetology & ObstetricsDwi Rofiqoh FauzahNo ratings yet
- Expectant Versus Aggressive Management in Severe Preeclampsia Remote From TermDocument6 pagesExpectant Versus Aggressive Management in Severe Preeclampsia Remote From Termmiss.JEJENo ratings yet
- Maternal and Obstetric Outcome of Women With Epilepsy 2009 SeizureDocument4 pagesMaternal and Obstetric Outcome of Women With Epilepsy 2009 Seizurebilal hadiNo ratings yet
- Early Onset Neonatal Sepsis. Diagnostic Dilemmas and Practical ManagementDocument6 pagesEarly Onset Neonatal Sepsis. Diagnostic Dilemmas and Practical Managementlink0105No ratings yet
- MCN Case Study-2pDocument76 pagesMCN Case Study-2pAngeline ShackletonNo ratings yet
- 11 HivDocument15 pages11 HivAswin BoyNo ratings yet
- 6 Hepatitis BDocument12 pages6 Hepatitis BAswin BoyNo ratings yet
- Management of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineDocument6 pagesManagement of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice Guidelineabu abdirrahmanNo ratings yet
- Case Summary OGDocument4 pagesCase Summary OGsyahirjohan2000No ratings yet
- Expert Perspective On A Clinical Challenge Lupus 2024Document11 pagesExpert Perspective On A Clinical Challenge Lupus 2024yokotoyNo ratings yet
- Asociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Document8 pagesAsociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Andrés Gaviria CNo ratings yet
- Konstantopoulos 2020Document14 pagesKonstantopoulos 2020Corey WoodsNo ratings yet
- Predictores Tempranos Del Síndrome de Guillain-Barré en El Curso de La Vida de Las MujeresDocument9 pagesPredictores Tempranos Del Síndrome de Guillain-Barré en El Curso de La Vida de Las Mujeresfrancisco bacaNo ratings yet
- Guillian Barre Treatament 2009Document3 pagesGuillian Barre Treatament 2009MEG GANNo ratings yet
- Maternal Sepsis Update - Curr Opin Anesthesiol - 2021Document6 pagesMaternal Sepsis Update - Curr Opin Anesthesiol - 2021Alex Degracia100% (1)
- Congenital Syphilis Associated With Cholestatic and Cardiomyopathy Diagnosed in An Infant Past The Newborn Period - A Case ReportDocument3 pagesCongenital Syphilis Associated With Cholestatic and Cardiomyopathy Diagnosed in An Infant Past The Newborn Period - A Case ReportMeliana SulistioNo ratings yet
- Jorgensen 2017Document6 pagesJorgensen 2017jessicapxeNo ratings yet
- FetalDocument2 pagesFetalHay PeeNo ratings yet
- Seizures in Infancy in The Offspring of Women With Epilepsy 2019Document5 pagesSeizures in Infancy in The Offspring of Women With Epilepsy 2019Josefco RiveroNo ratings yet
- Miliary Tuberculosis Associated 08022024 4Document5 pagesMiliary Tuberculosis Associated 08022024 4Novelty JournalsNo ratings yet
- Nur 1208 Maternal Concept Case 1 1Document11 pagesNur 1208 Maternal Concept Case 1 1Sheyra Angelica “Shey” BerdonarNo ratings yet
- Lepine2018 PDFDocument6 pagesLepine2018 PDFYaddi Fernanda Solarte MenjuraNo ratings yet
- Pregnancy in Patients With B-Thalassemia Intermedia: Outcome of Mothers and NewbornsDocument4 pagesPregnancy in Patients With B-Thalassemia Intermedia: Outcome of Mothers and NewbornsIlham RamadhanisNo ratings yet
- Associations of Snoring Frequency and Intensity in Pregnancy With Time-To - DeliveryDocument8 pagesAssociations of Snoring Frequency and Intensity in Pregnancy With Time-To - Delivery杨钦杰No ratings yet
- LBW ImmunizationDocument7 pagesLBW ImmunizationLaras San ChizeteNo ratings yet
- Reply Ymob 10Document1 pageReply Ymob 10Apple StarNo ratings yet
- Vitamin A Deficiency in Human Immunodeficiency Virus Type-1 Infected and Un-Infected Pregnant Women in KPK, PakistanDocument7 pagesVitamin A Deficiency in Human Immunodeficiency Virus Type-1 Infected and Un-Infected Pregnant Women in KPK, PakistanOpenaccess Research paperNo ratings yet
- First Trimester Cystic Hygroma - Herald To Early Diagnosis of Congenital Diaphragmatic HerniaDocument3 pagesFirst Trimester Cystic Hygroma - Herald To Early Diagnosis of Congenital Diaphragmatic HerniaFernanda SmerkinNo ratings yet
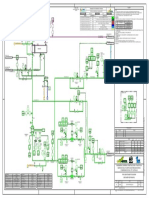
- HE-210 P-2604A-B - DEBUTANIZER FEED PREHEATING - Rev 0CxDocument1 pageHE-210 P-2604A-B - DEBUTANIZER FEED PREHEATING - Rev 0CxMariaNo ratings yet
- Gestational Hypertension - UTD PDFDocument21 pagesGestational Hypertension - UTD PDFShahar Perea ArizaNo ratings yet
- Analisis Permasalahan Hukum E-Commerce Dan Pengaturannya Di Indonesia Tansah RahmatullahDocument14 pagesAnalisis Permasalahan Hukum E-Commerce Dan Pengaturannya Di Indonesia Tansah RahmatullahFrans RajagukgukNo ratings yet
- Philippines RegionsDocument5 pagesPhilippines RegionsKristine MercadoNo ratings yet
- DLL Mathematics 6 q4 w6Document7 pagesDLL Mathematics 6 q4 w6Abegail CorpuzNo ratings yet
- Class 9 Science Worksheet - Matter in Our Surroundings - 1Document2 pagesClass 9 Science Worksheet - Matter in Our Surroundings - 1Sumedha Thakur100% (1)
- Daughtrey v. Fresno City Police Department, Et Al. - Document No. 4Document1 pageDaughtrey v. Fresno City Police Department, Et Al. - Document No. 4Justia.comNo ratings yet
- Introductory Entomology: Third Semester Lamjung CampusDocument206 pagesIntroductory Entomology: Third Semester Lamjung Campusnishan khatriNo ratings yet
- GregormendelandhispeasreadingandquestionsDocument2 pagesGregormendelandhispeasreadingandquestionsapi-248015505No ratings yet
- 03-15-2016 ECF 305 USA V JON RITZHEIMER - Response To Motion by USA As To Jon Ritzheimer Re Motion For Release From CustodyDocument12 pages03-15-2016 ECF 305 USA V JON RITZHEIMER - Response To Motion by USA As To Jon Ritzheimer Re Motion For Release From CustodyJack RyanNo ratings yet
- Manual DESERT EAGLE PDFDocument48 pagesManual DESERT EAGLE PDFlachie2703100% (1)
- Balancing of Single and Multi - Cylinder EnginesDocument24 pagesBalancing of Single and Multi - Cylinder Enginesdinesh veerNo ratings yet
- Combiflam Tablets PI - 08072019Document13 pagesCombiflam Tablets PI - 08072019ArunNo ratings yet
- Homotoxicology 6 Phase TableDocument1 pageHomotoxicology 6 Phase TableSamNo ratings yet
- Walther Handgun Comparison ChartDocument1 pageWalther Handgun Comparison ChartSasaki KyoukaNo ratings yet
- AP 5902 Liability Supporting NotesDocument6 pagesAP 5902 Liability Supporting NotesMeojh Imissu100% (1)
- Rex International Holding Limited Preliminary Offer DocumentDocument723 pagesRex International Holding Limited Preliminary Offer DocumentInvest StockNo ratings yet
- Create Request For QuotationDocument18 pagesCreate Request For QuotationAdauto PolizeliNo ratings yet
- Instruction SMA TripowerDocument10 pagesInstruction SMA TripowerMirea AurelNo ratings yet
- Plagiarism Prevention Software: TurnitinDocument24 pagesPlagiarism Prevention Software: TurnitinJoshua QuayeNo ratings yet
- Assembly of PartsDocument29 pagesAssembly of PartsthirumalaikumaranNo ratings yet
- The Fox Project, A ReappraisalDocument22 pagesThe Fox Project, A ReappraisalZemin OonNo ratings yet
- Series HDocument6 pagesSeries HAviation World100% (3)
- Table of ASCII CharactersDocument2 pagesTable of ASCII CharactersVü PhämNo ratings yet
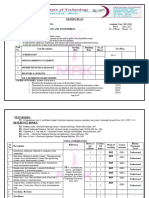
- Lesson Plan Ds 8603Document7 pagesLesson Plan Ds 8603sramalingam288953No ratings yet
- T07-Knowledge Application SystemsDocument18 pagesT07-Knowledge Application SystemsSamar sarahnaNo ratings yet