Download as pdf or txt
You might also like
- Cymbopogon Citratus (Lemon Grass), Garlic Clove Skin, and Azadirachta Indica (NeemDocument29 pagesCymbopogon Citratus (Lemon Grass), Garlic Clove Skin, and Azadirachta Indica (NeemJohn Drake TagavillaNo ratings yet
- DRUG STUDY - Ceftriaxone (Forgram)Document2 pagesDRUG STUDY - Ceftriaxone (Forgram)julesubayubay5428100% (8)
- Bacteria-Borne Diseases Handout 2022Document3 pagesBacteria-Borne Diseases Handout 2022Anna CrisNo ratings yet
- PharmacologyDocument20 pagesPharmacologyJayla MarieNo ratings yet
- Infectious Diseases USMLE Notes (Free Trial)Document1 pageInfectious Diseases USMLE Notes (Free Trial)Laura Tapia100% (1)
- MYCOBACTERIADocument8 pagesMYCOBACTERIAHANNA CASANDRA GARCIANo ratings yet
- Cefuroxime Axetil (IV)Document2 pagesCefuroxime Axetil (IV)STORAGE FILENo ratings yet
- High Fever Stiff Neck Severe HeadacheDocument3 pagesHigh Fever Stiff Neck Severe HeadacheDiana Jane LauretaNo ratings yet
- DrugsDocument2 pagesDrugsmelody_loki1464No ratings yet
- Haemophilus and BordetellaDocument12 pagesHaemophilus and BordetellaDaiki AomineNo ratings yet
- BBB - Respi&gi ReportsDocument11 pagesBBB - Respi&gi ReportsshesahNo ratings yet
- Shanz - Pedia Ii 2.03Document7 pagesShanz - Pedia Ii 2.03Petrina XuNo ratings yet
- Diphtheria: Sabah Mohsin Al-Maamuri MDDocument3 pagesDiphtheria: Sabah Mohsin Al-Maamuri MDAmmar AlnajjarNo ratings yet
- 3) Pharmacologic Management: Sound AlikeDocument7 pages3) Pharmacologic Management: Sound AlikeValerie LeddaNo ratings yet
- Neuron2 0331Document77 pagesNeuron2 0331baharehNo ratings yet
- Cefuroxime Axetil (Oral)Document2 pagesCefuroxime Axetil (Oral)STORAGE FILENo ratings yet
- Compiled Pedia Eye DiseasesDocument17 pagesCompiled Pedia Eye DiseasesJudy Ignacio EclarinoNo ratings yet
- Diphtheria NUN NOV 2023Document61 pagesDiphtheria NUN NOV 2023NUBWA MEDUGUNo ratings yet
- 18.1 - Infectious DiseasesDocument129 pages18.1 - Infectious DiseasesWarda TajammalNo ratings yet
- Fiji's EpiDocument13 pagesFiji's Epipofegeg809No ratings yet
- Micky Infectious NotesDocument10 pagesMicky Infectious NotesNoelani-Mei AscioNo ratings yet
- Pediatric Infectious Disease PT 2Document7 pagesPediatric Infectious Disease PT 2Erin Whisenand100% (1)
- Dengue-Malaria TOT For Doctors 2022 District Dengue PPTDocument88 pagesDengue-Malaria TOT For Doctors 2022 District Dengue PPTRanjeet SinghNo ratings yet
- Typhoid Fever, Paratyphoid Fever, and Typhoidal Fevers - Mandell's N DouglassDocument18 pagesTyphoid Fever, Paratyphoid Fever, and Typhoidal Fevers - Mandell's N DouglassNajmi QatrunnadaNo ratings yet
- Hemolytic Anemias: Common Findings in AllDocument4 pagesHemolytic Anemias: Common Findings in AllSamah KhanNo ratings yet
- SEPSIS Incomplete-NotesDocument4 pagesSEPSIS Incomplete-NotesbmiakhylaellaineNo ratings yet
- CNS Infections Aug 2022 Harsha - 2nd DraftDocument106 pagesCNS Infections Aug 2022 Harsha - 2nd Draftharsha sinhaNo ratings yet
- Sexually Transmitted Infections 19-21Document4 pagesSexually Transmitted Infections 19-21Ashar AhmadNo ratings yet
- UcellosisDocument4 pagesUcellosisyandraNo ratings yet
- Infections of The Eyes and The Central Nervous System - Dr. CerradaDocument68 pagesInfections of The Eyes and The Central Nervous System - Dr. CerradaMonique BorresNo ratings yet
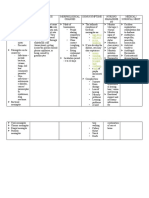
- Disease Causative Agent Diagnosis Classification/ S&S TreatmentDocument4 pagesDisease Causative Agent Diagnosis Classification/ S&S Treatmentfreya_28No ratings yet
- Toxic Shock Syndrome - PPTX 1-1Document49 pagesToxic Shock Syndrome - PPTX 1-1Mohammed Khedr100% (1)
- Brand Name Generic Name Dosage Action Indication Contra-Indication Precautions Nursing ConsiderationDocument6 pagesBrand Name Generic Name Dosage Action Indication Contra-Indication Precautions Nursing ConsiderationDrexcy Jhoy San AntonioNo ratings yet
- MeningitisDocument16 pagesMeningitishunzala shamirNo ratings yet
- Drug Study NicoleDocument6 pagesDrug Study NicoleFrancheska Nicole Delos SantosNo ratings yet
- CNS InfectionDocument10 pagesCNS InfectionShunqing ZhangNo ratings yet
- Period of Communicability: ChloramphenicolDocument10 pagesPeriod of Communicability: ChloramphenicolDona Mae TaberaNo ratings yet
- 4 - Gram Negative BacteriaDocument7 pages4 - Gram Negative BacteriaPHAMAE JOY MEMBREVENo ratings yet
- Measles Virus (Rubeola) : Anne A. GershonDocument10 pagesMeasles Virus (Rubeola) : Anne A. GershonTammy Utami DewiNo ratings yet
- Sepsis and MODS 2Document12 pagesSepsis and MODS 2Alex ChiuNo ratings yet
- Micropara Rev Ppt10Document12 pagesMicropara Rev Ppt10femmeclub coNo ratings yet
- Concept Map 4 AnsiiDocument1 pageConcept Map 4 Ansiiapi-523409624No ratings yet
- Meningitis .pptx-2Document29 pagesMeningitis .pptx-2inderaaputraaNo ratings yet
- Gram Positive Rod of Medical Imortance IIDocument36 pagesGram Positive Rod of Medical Imortance IIJoeyNo ratings yet
- 5 Systemic-MycosesDocument2 pages5 Systemic-MycosesMariz MartinezNo ratings yet
- Review For Infec-Tious D.: Brain InflammationDocument25 pagesReview For Infec-Tious D.: Brain InflammationFaith S KimNo ratings yet
- MeaslesDocument12 pagesMeaslesjanapolana9No ratings yet
- DiphtheriaDocument3 pagesDiphtheriakpkr603No ratings yet
- Hiv Aids-3Document5 pagesHiv Aids-3ADRIATICO JAROSLUVNo ratings yet
- Leptospirosis - Ferri's Clinical AdvisorDocument2 pagesLeptospirosis - Ferri's Clinical AdvisorAndika GhifariNo ratings yet
- Remaining Bacteria NotesDocument12 pagesRemaining Bacteria NotescahapaynathanieljoshuaNo ratings yet
- Thrombolic, Thrombocytopenic Purpurvhemoclytic Uremic Syndrome (SeizuresDocument1 pageThrombolic, Thrombocytopenic Purpurvhemoclytic Uremic Syndrome (Seizuresgeorgeloto12No ratings yet
- Diseases of Public Health Part 1Document3 pagesDiseases of Public Health Part 1Jas GandingcoNo ratings yet
- Neuro NotesDocument15 pagesNeuro NotesClyde CapapasNo ratings yet
- Exam 2 Study Guide 2018Document21 pagesExam 2 Study Guide 2018EvanNo ratings yet
- Ilovepdf MergedDocument18 pagesIlovepdf MergedAnita Paredes VillegasNo ratings yet
- Ceftriaxone SodiumDocument2 pagesCeftriaxone SodiumSTORAGE FILENo ratings yet
- PnemoniaDocument4 pagesPnemoniadhavalNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Autonomic SystemDocument5 pagesAutonomic Systemdqnxfdw6bjNo ratings yet
- General AnesthesiaDocument4 pagesGeneral Anesthesiadqnxfdw6bjNo ratings yet
- Pharma and GraphDocument2 pagesPharma and Graphdqnxfdw6bjNo ratings yet
- Crazy Laura Printable Pack JournalDocument65 pagesCrazy Laura Printable Pack Journaldqnxfdw6bjNo ratings yet
- Spinal Cord LesionDocument3 pagesSpinal Cord Lesiondqnxfdw6bjNo ratings yet
- تدبر في القرآن و ادعيهDocument27 pagesتدبر في القرآن و ادعيهdqnxfdw6bjNo ratings yet
- العون الإلهيDocument3 pagesالعون الإلهيdqnxfdw6bjNo ratings yet
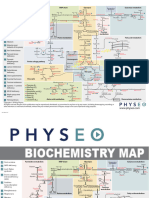
- Bio MapDocument2 pagesBio Mapdqnxfdw6bjNo ratings yet
- 6-Month UFABB With FA 2021Document16 pages6-Month UFABB With FA 2021dqnxfdw6bjNo ratings yet
- Final Memorial From Side StateDocument14 pagesFinal Memorial From Side StateSAUMYA GIRINo ratings yet
- Learning Outcomes: Able To LIST Scope in ParasitologyDocument32 pagesLearning Outcomes: Able To LIST Scope in ParasitologySyahirah Binti Husairi100% (1)
- Staying at Home and Away From Others Social Distancing PDF Upload For Gov - Uk PDFDocument6 pagesStaying at Home and Away From Others Social Distancing PDF Upload For Gov - Uk PDFTeymur DadashovNo ratings yet
- FAQ On Rescinding The Local Stay at Home Order 5.8.20Document2 pagesFAQ On Rescinding The Local Stay at Home Order 5.8.20The UnionNo ratings yet
- Principles of Diagnostic Medical MicrobiologyDocument4 pagesPrinciples of Diagnostic Medical MicrobiologyTarequl Islam NishadNo ratings yet
- The Right-Wing of Fly (Musca Domestica) As A Neutralization of Drinks Contaminated by MicrobeDocument3 pagesThe Right-Wing of Fly (Musca Domestica) As A Neutralization of Drinks Contaminated by MicrobeLove DubaiNo ratings yet
- 1 OnlineDocument6 pages1 Onlineanalisaapil312No ratings yet
- Directorate General of Health ServicesDocument1 pageDirectorate General of Health Servicesmujahid_islam85No ratings yet
- Biology ProjectDocument18 pagesBiology Project39 Aditiya DuttaNo ratings yet
- Food Microbiology PDFDocument217 pagesFood Microbiology PDFFernando Dias100% (3)
- A Fuller Picture of Vaccination - FinalDocument36 pagesA Fuller Picture of Vaccination - FinalJessica Learmond-CriquiNo ratings yet
- Dengue FeverDocument28 pagesDengue Fevercooky maknaeNo ratings yet
- Archives of Clinical MicrobiologyDocument86 pagesArchives of Clinical MicrobiologyInternational Medical PublisherNo ratings yet
- Procedure For Assessing The Acceptability, in Principle, of Vaccines (Page 315)Document398 pagesProcedure For Assessing The Acceptability, in Principle, of Vaccines (Page 315)Abdelkarim BelkebirNo ratings yet
- Journal of Plant PhysiologyDocument4 pagesJournal of Plant PhysiologygillNo ratings yet
- Z481upi 03Document2 pagesZ481upi 03Ahmed AliNo ratings yet
- Further: Honey Bee Pathology1Document23 pagesFurther: Honey Bee Pathology1LoredanaNo ratings yet
- Lymphatic System OutlineDocument4 pagesLymphatic System OutlineMelljonhNo ratings yet
- Inspekcija Krompir, NAKDocument38 pagesInspekcija Krompir, NAKgandra80No ratings yet
- Kanagalingam2015 PDFDocument10 pagesKanagalingam2015 PDFwatidinaNo ratings yet
- Absolute Lymphocyte Count Normal Range - Google SDocument1 pageAbsolute Lymphocyte Count Normal Range - Google SAshraf C VNo ratings yet
- Immunity EPIDocument37 pagesImmunity EPIluttomiayvonneNo ratings yet
- Handbook of Specimen Collection and Handling in MicrobiologyDocument72 pagesHandbook of Specimen Collection and Handling in MicrobiologyMiguel MataNo ratings yet
- DR Bhavini Sandip Shah Director: Microbiology Department of Microbiology Neuberg Supratech Labs AhmedabadDocument49 pagesDR Bhavini Sandip Shah Director: Microbiology Department of Microbiology Neuberg Supratech Labs Ahmedabadkrutarth shahNo ratings yet
- Sample Research Paper BacteriaDocument7 pagesSample Research Paper Bacteriafvjebmpk100% (1)
- AuditDocument5 pagesAuditkatie_112885729No ratings yet
- Covid 19 Charter of Iob KSDocument5 pagesCovid 19 Charter of Iob KSAnonymous 4yXWpDNo ratings yet
- RA-EHS-047-E2 - Covid-19 Site Risk Assessment 002Document16 pagesRA-EHS-047-E2 - Covid-19 Site Risk Assessment 002Samsu RizalNo ratings yet
- Lippincott - S Illustrated Q - A Review of Microbiology - Immunology VirusDocument17 pagesLippincott - S Illustrated Q - A Review of Microbiology - Immunology VirusGoose ChapmanNo ratings yet