Download as pdf or txt
You might also like
- Adrenergic ReceptorsDocument1 pageAdrenergic ReceptorsBobet ReñaNo ratings yet
- USONA INSTITUTE - 2018 - Psilocybin Investigator BrochureDocument59 pagesUSONA INSTITUTE - 2018 - Psilocybin Investigator BrochureSandro RodriguesNo ratings yet
- Anesthesia PharmacologyDocument41 pagesAnesthesia PharmacologyHassan.shehri88% (8)
- General Anesthetics TRANSDocument15 pagesGeneral Anesthetics TRANSNikki Tuazon BartolomeNo ratings yet
- SNS and PNS Drugs (Cholinergics and Adrenergics)Document5 pagesSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- Butorphanol Tartrate (Drug Study)Document2 pagesButorphanol Tartrate (Drug Study)Franz.thenurse6888100% (2)
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Nitrous Oxide Isoflurane Halothane Enflurane Sevoflurane DesfluraneDocument3 pagesNitrous Oxide Isoflurane Halothane Enflurane Sevoflurane DesfluraneNariska CooperNo ratings yet
- Sedative-Hypnotic Drugs: Alprazolam Chlordiazepoxide Clonazepam ClorazepateDocument8 pagesSedative-Hypnotic Drugs: Alprazolam Chlordiazepoxide Clonazepam ClorazepateCas BuNo ratings yet
- Sedatives & HypnoticsDocument49 pagesSedatives & HypnoticsShubha DiwakarNo ratings yet
- Barbiturates Drug SummaryDocument5 pagesBarbiturates Drug SummarySydney JenningsNo ratings yet
- Clinical Pharmacology of Anesthetic Drugs: Dr. Waddah H. AwadDocument37 pagesClinical Pharmacology of Anesthetic Drugs: Dr. Waddah H. AwadwaddahawadNo ratings yet
- CNS DepressantsDocument69 pagesCNS DepressantsMicah Lou Calamba100% (1)
- Sedative HypnoticDocument60 pagesSedative HypnoticNeeraj KumarNo ratings yet
- MalnutritionDocument22 pagesMalnutritionkelvinamin12No ratings yet
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 5Document5 pagesBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 5ravi2likeNo ratings yet
- General Anaesthesia: I Made Agus Kresna SucandraDocument38 pagesGeneral Anaesthesia: I Made Agus Kresna SucandraGianna GraciellaNo ratings yet
- Sedative HypnoticsDocument27 pagesSedative HypnoticsPrecious FulgarinasNo ratings yet
- Drugs For AsthmaDocument1 pageDrugs For Asthmakamil malikNo ratings yet
- Lecture 28 - 3rd Asessment - Sedatives, HypnoticsDocument32 pagesLecture 28 - 3rd Asessment - Sedatives, Hypnoticsapi-3703352100% (1)
- General Anaesthesia & Skeletal Muscle RelaxantDocument31 pagesGeneral Anaesthesia & Skeletal Muscle RelaxantDeepti SinglaNo ratings yet
- General Anesthesia For NursingDocument53 pagesGeneral Anesthesia For Nursingpuneetkumar7089No ratings yet
- Hypnotics and SedativesDocument22 pagesHypnotics and Sedativeskavya nainitaNo ratings yet
- Drugs Used For Treatment of Asthma - 1Document6 pagesDrugs Used For Treatment of Asthma - 1ireneNo ratings yet
- Impaired Gas ExchangeDocument1 pageImpaired Gas Exchangeruggero07No ratings yet
- General Anaesthesia: I Made Agus Kresna SucandraDocument37 pagesGeneral Anaesthesia: I Made Agus Kresna SucandraBakingpancakesNo ratings yet
- Local AnaestheticsDocument27 pagesLocal AnaestheticsRawand Ra'ed D.AlshawabkehNo ratings yet
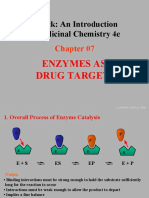
- Patrick: An Introduction To Medicinal Chemistry 4e: Enzymes As Drug TargetsDocument43 pagesPatrick: An Introduction To Medicinal Chemistry 4e: Enzymes As Drug TargetsVishaka KashyapNo ratings yet
- General Anesthesia: by Dr. AnindyaDocument83 pagesGeneral Anesthesia: by Dr. Anindyaalhada azofit almaNo ratings yet
- Recent Advances of TDDS: The Ultra-Deformable Vesicle (UDV) : by Sarah AdindaputeriDocument21 pagesRecent Advances of TDDS: The Ultra-Deformable Vesicle (UDV) : by Sarah AdindaputeriClarence WorthingtonNo ratings yet
- General Anaesthesia: I Made Agus Kresna SucandraDocument39 pagesGeneral Anaesthesia: I Made Agus Kresna SucandraDoqaNo ratings yet
- Local AnestheticsDocument44 pagesLocal Anestheticsblack pink in ur area 21No ratings yet
- Pharmacology - Drugs For CNS DisordersDocument4 pagesPharmacology - Drugs For CNS DisordersJireh MejinoNo ratings yet
- Cocaine Corneal Sloughing: Low Potency (Short DOA)Document4 pagesCocaine Corneal Sloughing: Low Potency (Short DOA)Thulasi tootsieNo ratings yet
- Pharmacology IV L5Document4 pagesPharmacology IV L5سلطان القلحNo ratings yet
- Drugs Acting On CNSDocument19 pagesDrugs Acting On CNSAditya sagarNo ratings yet
- Chapter 22 Sedative HypnoticsDocument7 pagesChapter 22 Sedative HypnoticsChristine Annmarie TapawanNo ratings yet
- SioooDocument4 pagesSioooanonymousNo ratings yet
- Basic Pharmacology PDFDocument27 pagesBasic Pharmacology PDFVizit DubeyNo ratings yet
- Farmako AnastesiaDocument4 pagesFarmako AnastesiaMuhammad Dafa Tira Pratista AkbarNo ratings yet
- Intravenous Anaesthetics: Thiopentone Methohexitone Propofol KetamineDocument9 pagesIntravenous Anaesthetics: Thiopentone Methohexitone Propofol KetamineTomNo ratings yet
- Name: Enjel Fanecha Difa NIM: 21117049 Major: Psik BDocument5 pagesName: Enjel Fanecha Difa NIM: 21117049 Major: Psik BEnjelNo ratings yet
- (Local Anaesthetics) : Dr. MizajDocument17 pages(Local Anaesthetics) : Dr. MizajaliNo ratings yet
- Jenis ShockDocument6 pagesJenis ShockMUHAMAD PATHU ROHMANNo ratings yet
- Sedative & HypnoticsDocument60 pagesSedative & HypnoticsDr Nilesh Patel100% (1)
- ANS DrugsDocument68 pagesANS DrugsROSEMARIE ONGNo ratings yet
- BenzodiazepinesDocument35 pagesBenzodiazepinesanaeshklNo ratings yet
- Leanna R. Miller: LRM ConsultingDocument20 pagesLeanna R. Miller: LRM ConsultingreneecolemanNo ratings yet
- Wsop Asma - Prof Bambang SDocument67 pagesWsop Asma - Prof Bambang SSiti Arieanni KesumaNo ratings yet
- Simplified ACLS AlgorithmDocument1 pageSimplified ACLS AlgorithmBrianNo ratings yet
- Hypnotic and SedativeDocument16 pagesHypnotic and SedativeAnim 2499No ratings yet
- Sedative-Hypnotics (SeH) and AnxiolyticsDocument101 pagesSedative-Hypnotics (SeH) and Anxiolyticsmatchees-gone rogueNo ratings yet
- Learning Objectives: Drugs That Enhance Cholinergic TransmissionDocument3 pagesLearning Objectives: Drugs That Enhance Cholinergic TransmissionSamer FarhanNo ratings yet
- Ek Ah YG EIA: Page 4 Out of 11 PagesDocument1 pageEk Ah YG EIA: Page 4 Out of 11 PagesRebekah EquizNo ratings yet
- Assignment AnesthesiaDocument9 pagesAssignment AnesthesiaRavi PatelNo ratings yet
- Pre Anesthetics Local AnestheticsDocument45 pagesPre Anesthetics Local AnestheticsDR AbidNo ratings yet
- Hydrophobic Ion PairingDocument14 pagesHydrophobic Ion PairingSilvia Argelia Peraza KuNo ratings yet
- (Surg2) 5.1b Introduction To Anesthesia-Part 2Document16 pages(Surg2) 5.1b Introduction To Anesthesia-Part 2AlloiBialbaNo ratings yet
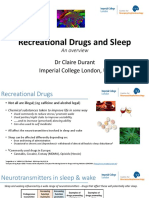
- Recreational Drugs and Sleep: DR Claire Durant Imperial College London, UKDocument24 pagesRecreational Drugs and Sleep: DR Claire Durant Imperial College London, UKSantiago Urzúa SaldívarNo ratings yet
- LOCAL ANESTHETICS and EMERGENCY DRUGSDocument7 pagesLOCAL ANESTHETICS and EMERGENCY DRUGSrosheanne0913No ratings yet
- Anti EmeticsDocument7 pagesAnti EmeticsPatricia BuzonNo ratings yet
- Autonomic SystemDocument5 pagesAutonomic Systemdqnxfdw6bjNo ratings yet
- MeningitisDocument5 pagesMeningitisdqnxfdw6bjNo ratings yet
- Pharma and GraphDocument2 pagesPharma and Graphdqnxfdw6bjNo ratings yet
- Crazy Laura Printable Pack JournalDocument65 pagesCrazy Laura Printable Pack Journaldqnxfdw6bjNo ratings yet
- Spinal Cord LesionDocument3 pagesSpinal Cord Lesiondqnxfdw6bjNo ratings yet
- تدبر في القرآن و ادعيهDocument27 pagesتدبر في القرآن و ادعيهdqnxfdw6bjNo ratings yet
- العون الإلهيDocument3 pagesالعون الإلهيdqnxfdw6bjNo ratings yet
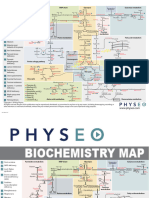
- Bio MapDocument2 pagesBio Mapdqnxfdw6bjNo ratings yet
- 6-Month UFABB With FA 2021Document16 pages6-Month UFABB With FA 2021dqnxfdw6bjNo ratings yet
- Jurnal EBCRDocument13 pagesJurnal EBCRDestry AryantyNo ratings yet
- Full Download PDF of Pharmacology For Medical Graduates, 4th Updated Edition Shanbhag - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Pharmacology For Medical Graduates, 4th Updated Edition Shanbhag - Ebook PDF All Chaptermawlwdszende100% (6)
- HBI Blacklist Journals 2018Document123 pagesHBI Blacklist Journals 2018pptpptNo ratings yet
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: Multiple Choice Questions (Pharmacology)Document65 pagesDr. Naitik D Trivedi & Dr. Upama N. Trivedi: Multiple Choice Questions (Pharmacology)Lokesh Mahata100% (1)
- 05 Paeds Drug Doses-1Document4 pages05 Paeds Drug Doses-1JunaidahMubarakAliNo ratings yet
- Puente PiedraDocument6 pagesPuente PiedraBotica Super FarmaNo ratings yet
- Bahasa Inggris Iii: 6. Giving InjectionDocument15 pagesBahasa Inggris Iii: 6. Giving InjectionErlangga PratamaNo ratings yet
- Magnesium Hydroxide (Milk of Magnesia)Document1 pageMagnesium Hydroxide (Milk of Magnesia)ENo ratings yet
- Pharmacology MnemonicsDocument17 pagesPharmacology MnemonicsJuvenis SampangNo ratings yet
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocument1 pageSteroid Tapering and Supportive Treatment Guidance V1.0 PDFPatricia MaisekaNo ratings yet
- Final ColistinDocument3 pagesFinal ColistinGwyn RosalesNo ratings yet
- Soal KpbiDocument5 pagesSoal KpbiTiffany Sabilla RamadhaniNo ratings yet
- Pharmacology ScrapbookDocument89 pagesPharmacology ScrapbookJesell France PlanaNo ratings yet
- 3.2 TheophyllineDocument3 pages3.2 TheophyllinesarahabdullahNo ratings yet
- Price ListDocument39 pagesPrice ListHarloXsiNo ratings yet
- Farmakologi KlinikDocument29 pagesFarmakologi KlinikMaria elisabethNo ratings yet
- SemaglutideDocument95 pagesSemaglutideShigma Putra Mahaley100% (1)
- Hydroxy ZineDocument2 pagesHydroxy ZineSharmaine Grace FlorigNo ratings yet
- Good Practice in CompoundingDocument53 pagesGood Practice in Compoundingvicky_law_2100% (1)
- PharmacologyDocument3 pagesPharmacologyVISHAKHANo ratings yet
- CCIM MD Dravyaguna Final SyllabusDocument12 pagesCCIM MD Dravyaguna Final SyllabusGiridhar VedantamNo ratings yet
- Clinical Trials and Drug DevelopmentDocument109 pagesClinical Trials and Drug DevelopmentYasimini RamadhaniNo ratings yet
- GuidelinesDocument94 pagesGuidelinesMichael PiducaNo ratings yet
- The Extract of Mucuna Pruriens Possesses Histamine Activity: Asian Pacific Journal of Tropical MedicineDocument3 pagesThe Extract of Mucuna Pruriens Possesses Histamine Activity: Asian Pacific Journal of Tropical MedicineSergio Andres Salas CoronelNo ratings yet
- Item Baru Klinik Pekanbaru 2022Document12 pagesItem Baru Klinik Pekanbaru 2022Listia NingsihNo ratings yet
- Fitri BHPDocument3 pagesFitri BHPekadwiyantiNo ratings yet
- Cms High Risk MedicationsDocument8 pagesCms High Risk MedicationsMihai VladescuNo ratings yet
- SPC - Ma130 00201Document6 pagesSPC - Ma130 00201Cassia FistulaNo ratings yet