Download as pdf or txt
You might also like
- Medical Examination For Teaching PermitDocument4 pagesMedical Examination For Teaching PermitEllina JamesNo ratings yet
- Business Plan For Orthopedic HospitalDocument5 pagesBusiness Plan For Orthopedic HospitalDarshan More100% (1)
- The Candidate Must Complete Section A of The Form and Submit It To The Med Al Fficer at T e Time of ExaminationDocument4 pagesThe Candidate Must Complete Section A of The Form and Submit It To The Med Al Fficer at T e Time of ExaminationJabdi LobahNo ratings yet
- GHS Health Declaration Form PDFDocument2 pagesGHS Health Declaration Form PDFFattah AfawNo ratings yet
- MD001 - Medical Examinations Supplement - CurrentDocument3 pagesMD001 - Medical Examinations Supplement - CurrentNatalie DouglasNo ratings yet
- 7.down SyndromeDocument15 pages7.down SyndromeTiara Khairina100% (1)
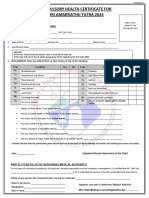
- Annexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Document1 pageAnnexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Shrasti SoniNo ratings yet
- English CHCDocument1 pageEnglish CHCBhupi AgrawalNo ratings yet
- English CHCDocument1 pageEnglish CHCShahvez AnsariNo ratings yet
- English CHCDocument1 pageEnglish CHCashish2225No ratings yet
- Compulsory Heal TH Certificate For Shri Amarna Thji Ya Tra 2023Document1 pageCompulsory Heal TH Certificate For Shri Amarna Thji Ya Tra 2023Eknath KoliNo ratings yet
- Medical Fitness Certificate For TrekkersDocument1 pageMedical Fitness Certificate For TrekkersRajatChadhaNo ratings yet
- FormatDocument3 pagesFormatchiragNo ratings yet
- Proposal of APGLI ProformaDocument5 pagesProposal of APGLI ProformaVenkataSubrahmanyamVennelakantiNo ratings yet
- Amarnath Yatra Compulsory Health Certificate 2017Document1 pageAmarnath Yatra Compulsory Health Certificate 2017Sneha KerkarNo ratings yet
- Chaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportDocument2 pagesChaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportbajibabuNo ratings yet
- Medical FormDocument3 pagesMedical FormPrincess Mae DesaculaNo ratings yet
- Your Lifestyle QuestionaireDocument2 pagesYour Lifestyle QuestionairevaluedynamicmarineNo ratings yet
- NUTP Health Declaration FormDocument2 pagesNUTP Health Declaration FormCik GeeNo ratings yet
- Death Summary Form For Covid-19: 1. Name of The Hospital: 2. Patient IdentificationDocument3 pagesDeath Summary Form For Covid-19: 1. Name of The Hospital: 2. Patient IdentificationFrank NobodNo ratings yet
- Health Certificate To Work in Confined SpaceDocument6 pagesHealth Certificate To Work in Confined SpacenmmarhelNo ratings yet
- Medical HistoryDocument3 pagesMedical HistorydjoiajgNo ratings yet
- Health Questionnaire For Online Version - Retail Revised VersionDocument4 pagesHealth Questionnaire For Online Version - Retail Revised VersionTrushaba B. JadejaNo ratings yet
- Forrm 4aDocument4 pagesForrm 4aJ.L. Jumbo XeroxNo ratings yet
- GPMRDocument5 pagesGPMRwisdom hameloNo ratings yet
- Medical Tasac New - Iso - 1Document11 pagesMedical Tasac New - Iso - 1Mustafa JumaNo ratings yet
- Medical Fitness FormDocument1 pageMedical Fitness FormvickyreddyNo ratings yet
- Pre-Anaesthetic Self Assessment FormDocument2 pagesPre-Anaesthetic Self Assessment FormmmmmNo ratings yet
- CHCAndApplicationForm2022 1 2Document2 pagesCHCAndApplicationForm2022 1 2sawant.httpNo ratings yet
- Hypertension QuestionnaireDocument1 pageHypertension QuestionnairekhalidsuccessfutureNo ratings yet
- Latihan MTK Un SMP BahasDocument2 pagesLatihan MTK Un SMP Bahasdinas pertanianNo ratings yet
- TYPED-medical SoftDocument5 pagesTYPED-medical SoftynrajambaNo ratings yet
- Application Form and CHC Form For Yatra 2021Document2 pagesApplication Form and CHC Form For Yatra 2021nitishNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFpierlisurNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- Medical ForDocument8 pagesMedical FormarandugebraNo ratings yet
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Document6 pagesPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieNo ratings yet
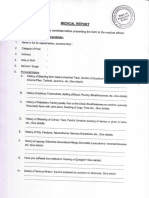
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- Medical FormDocument4 pagesMedical FormSujata DeviNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCODocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOsimpoonNo ratings yet
- Name (In Full) Date of Birth Gender Male / Female Blood Group Physical Disability, If Any Kindly Answer All The Following QuestionsDocument2 pagesName (In Full) Date of Birth Gender Male / Female Blood Group Physical Disability, If Any Kindly Answer All The Following QuestionsVikranth VeeraNo ratings yet
- Medical Fitness PDFDocument5 pagesMedical Fitness PDFVenkateshwara ReddyNo ratings yet
- Cashless Request Form PDFDocument2 pagesCashless Request Form PDFPrime multispecialiaty HospitalNo ratings yet
- ProposaForm Questionniare Linked CHRDocument1 pageProposaForm Questionniare Linked CHRPrachi DubeyNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsMaria JessaNo ratings yet
- NEW PE FORM Bangayan Vhynee SDocument4 pagesNEW PE FORM Bangayan Vhynee SVhynee BangayanNo ratings yet
- 00 Obs&Gyn Clerkship-1-1Document9 pages00 Obs&Gyn Clerkship-1-1samwel daniel100% (1)
- Compulsory Health Certificate For Shri Amarnathji Yatra 2023Document1 pageCompulsory Health Certificate For Shri Amarnathji Yatra 2023Eknath KoliNo ratings yet
- Medical Examination Form-2Document1 pageMedical Examination Form-2hassanNo ratings yet
- Individual Health Application FormDocument2 pagesIndividual Health Application FormRalph Wamae0% (1)
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- 00 Paediatric Clerkship-1Document9 pages00 Paediatric Clerkship-1Lexis SanchizieNo ratings yet
- Jointly Team: SMLE GroupDocument11 pagesJointly Team: SMLE GroupAkpevwe EmefeNo ratings yet
- Medical Second Opinion Request FormDocument5 pagesMedical Second Opinion Request Formapi-380809599No ratings yet
- Health Questionnaire CandidateDocument5 pagesHealth Questionnaire CandidateSaudia Arabia JobsNo ratings yet
- Medical Declaration Form: Family History of The ApplicantDocument3 pagesMedical Declaration Form: Family History of The ApplicantJae WaiNo ratings yet
- Hazz VCDocument1 pageHazz VCSoleman ITNo ratings yet
- Paediatric Clerkship 1Document9 pagesPaediatric Clerkship 1fredrick damian100% (1)
- Yusleydi Rivas Gastro QuestionaireDocument1 pageYusleydi Rivas Gastro Questionairejuan manuelNo ratings yet
- Sapna NCPDocument22 pagesSapna NCPgill priyaNo ratings yet
- Investigative Study Into the Relationship Between Gulf War Syndrome and Well-Being of Persian Gulf War VeteransFrom EverandInvestigative Study Into the Relationship Between Gulf War Syndrome and Well-Being of Persian Gulf War VeteransNo ratings yet
- A-Z Ayurveda Practical Prescriber (Atreya'S Guidelines For Ayurveda Practice Book 3) by Vaidya Vasant PatilDocument8 pagesA-Z Ayurveda Practical Prescriber (Atreya'S Guidelines For Ayurveda Practice Book 3) by Vaidya Vasant Patilsrikanth PosaNo ratings yet
- Case Presentation FormateDocument51 pagesCase Presentation Formatepriyanka bhavsarNo ratings yet
- Terapi Nutrisi Pada Obesitas - Dr. GagaDocument6 pagesTerapi Nutrisi Pada Obesitas - Dr. Gagavina hidayatNo ratings yet
- Diseases of Muscular SystemDocument2 pagesDiseases of Muscular SystemChari Mae Tamayo PanganibanNo ratings yet
- A Case of Renal Stone With Moderate Hepatospleenomegaly and ?cystitisDocument6 pagesA Case of Renal Stone With Moderate Hepatospleenomegaly and ?cystitisHomoeopathic PulseNo ratings yet
- Tuberculous Mastitis A Case ReportDocument4 pagesTuberculous Mastitis A Case ReportLmao DNo ratings yet
- CNCPDocument4 pagesCNCPJOHN ROIENo ratings yet
- Table of Contents CTD FormatDocument5 pagesTable of Contents CTD Formatgsharma20203158No ratings yet
- Mortalidad Adultos MundoDocument86 pagesMortalidad Adultos MundoJacob DavisNo ratings yet
- Ashly M. Hemstreet: ObjectiveDocument2 pagesAshly M. Hemstreet: Objectiveapi-253534469No ratings yet
- Wound Closure ManualDocument127 pagesWound Closure ManualDougyStoffell100% (6)
- Steps in Outbreak InvestigationDocument34 pagesSteps in Outbreak Investigationsharmaine peroNo ratings yet
- Tobacco ControlDocument19 pagesTobacco ControlWekesa EvansNo ratings yet
- Vithoulkas Talks On Homeopathy Part3 Discussions PDFDocument60 pagesVithoulkas Talks On Homeopathy Part3 Discussions PDFtejaswi_nisanth100% (3)
- Universitas Muhammadiyah Ponorogo Health Sciences Journal: Ilham Muhammad, Laily Isro'in, Metti VerawatiDocument17 pagesUniversitas Muhammadiyah Ponorogo Health Sciences Journal: Ilham Muhammad, Laily Isro'in, Metti VerawatiQurrotul AnnisaNo ratings yet
- Comprehensive NursingDocument29 pagesComprehensive NursingAmir Ahmed GezaNo ratings yet
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrsSrinivasamurthy KamarthiNo ratings yet
- Overview of HEPO RoadmapDocument21 pagesOverview of HEPO RoadmapAbdulmejid AbdureufNo ratings yet
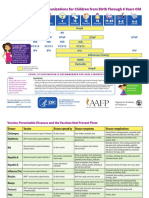
- National Immunisation ScheduleDocument2 pagesNational Immunisation SchedulegreatvedasNo ratings yet
- Goldendent CatalogDocument28 pagesGoldendent CatalogabhinavNo ratings yet
- 091 - Athaya Karima Mahira (Tongue Diagnosis)Document4 pages091 - Athaya Karima Mahira (Tongue Diagnosis)Athaya Karima MahiraNo ratings yet
- C1 Ob-Gyn-2020Document33 pagesC1 Ob-Gyn-2020yabsera mulatuNo ratings yet
- Fneur 13 871187Document7 pagesFneur 13 871187Yery AparicioNo ratings yet
- Feltölt1 PDFDocument11 pagesFeltölt1 PDFMa Vi100% (1)
- NEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0 PDFDocument1 pageNEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0 PDFArisita Andy PutriNo ratings yet
- PFCM - Technical Paper Preventive MedicineDocument2 pagesPFCM - Technical Paper Preventive MedicineYolanda Primrosa NurhanNo ratings yet
- Diabetic FootDocument46 pagesDiabetic FootRhapsody RedNo ratings yet
- Cyclosporine For Moderate-To-Severe Alopecia Areata: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial of Efficacy and SafetyDocument8 pagesCyclosporine For Moderate-To-Severe Alopecia Areata: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial of Efficacy and Safetysupaidi97No ratings yet