Download as docx, pdf, or txt
You might also like
- Taller ContaminantesDocument11 pagesTaller ContaminantesDaniel F Amado0% (1)
- Consultants List-ADCEDocument6 pagesConsultants List-ADCEJaveed Taji100% (3)
- A Peacock in The Land of Penguins - A Tale of Diversity and Discovery (PDFDrive)Document164 pagesA Peacock in The Land of Penguins - A Tale of Diversity and Discovery (PDFDrive)Zeenat ZahirNo ratings yet
- The Souled StoreDocument8 pagesThe Souled StoreRani DispotaNo ratings yet
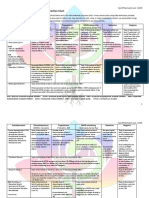
- Antidepressant & Psychedelic Drug Interaction ChartDocument3 pagesAntidepressant & Psychedelic Drug Interaction ChartFred The Nomad100% (2)
- 06 - The Modes of Ancient Greece - Elsie HamiltonDocument20 pages06 - The Modes of Ancient Greece - Elsie HamiltonRafa Noguera FernándezNo ratings yet
- Genres and Text Types in English Language TeachingDocument18 pagesGenres and Text Types in English Language TeachingAryadne AraujoNo ratings yet
- Anti DepressentsDocument2 pagesAnti DepressentsAch Ri Fa INo ratings yet
- 3.1 Pharmacology Lecture Part-II 2023Document53 pages3.1 Pharmacology Lecture Part-II 2023Talha TariqNo ratings yet
- CNS 29 - 39Document12 pagesCNS 29 - 39Michiko_Lois_Tao_203No ratings yet
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- Antidepressants Drug SnigDocument18 pagesAntidepressants Drug SnigSnigdha MishraNo ratings yet
- A. Stahl - STAHL's, Essential PharmacologyDocument53 pagesA. Stahl - STAHL's, Essential PharmacologyDaniel De los SantosNo ratings yet
- Antidepresive Sedative ActivatoareDocument2 pagesAntidepresive Sedative ActivatoareDrima EdiNo ratings yet
- Tramadol, Paracetamol, Calmoseptine, B12Document5 pagesTramadol, Paracetamol, Calmoseptine, B12Denise EspinosaNo ratings yet
- AntidepressantsDocument12 pagesAntidepressantsMonica PaulNo ratings yet
- MEDICAL SURGICAL NURSING ASSESSMENT AND MANAGEMENT OF CLINICAL PROBLEMS 9th EditionDocument1 pageMEDICAL SURGICAL NURSING ASSESSMENT AND MANAGEMENT OF CLINICAL PROBLEMS 9th EditionMeryPinkihanNo ratings yet
- Antidepressant DrugsDocument19 pagesAntidepressant DrugsUMESH KANDELNo ratings yet
- 1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsDocument2 pages1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsPopov VictorNo ratings yet
- Philippine College of Health Sciences Pharmacology 1Document5 pagesPhilippine College of Health Sciences Pharmacology 1Ric BarrosNo ratings yet
- 21 Management of Affective Disorder - Blok 18 - UNTAD - 2011Document20 pages21 Management of Affective Disorder - Blok 18 - UNTAD - 2011Yulita PurbaNo ratings yet
- AntidepressantDocument8 pagesAntidepressantKlarasita WibowoNo ratings yet
- Drugs Affecting The Central Nervous SystemDocument16 pagesDrugs Affecting The Central Nervous SystemShafaqNo ratings yet
- Diploma Pembantu Perubatan: Tajuk: Antipsikotik & AntidepresiDocument3 pagesDiploma Pembantu Perubatan: Tajuk: Antipsikotik & AntidepresiazrulNo ratings yet
- Drug StudyDocument4 pagesDrug StudyDean Angelo BarrientosNo ratings yet
- Drug Study: Sedation, Dizziness/vertigo, Headache, Hypotension Sweating, Nausea, VomitingDocument1 pageDrug Study: Sedation, Dizziness/vertigo, Headache, Hypotension Sweating, Nausea, VomitingRoland YusteNo ratings yet
- Clinical ToxicologyDocument6 pagesClinical ToxicologyGrace MarinoNo ratings yet
- Drug Study: TramadolDocument5 pagesDrug Study: TramadolOmyl-Khayr M. SulogNo ratings yet
- Cholinoceptor AntagonistDocument21 pagesCholinoceptor Antagonistraafat mohammedNo ratings yet
- AntidepressantsDocument4 pagesAntidepressantsGrace CabilloNo ratings yet
- Anti-Depressants: Soumya Mary 1 Year MSC (N)Document22 pagesAnti-Depressants: Soumya Mary 1 Year MSC (N)Salman HabeebNo ratings yet
- Drug StudyDocument6 pagesDrug StudyLovelyNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJerica Mae VenoyaNo ratings yet
- Final Trivia - Preparation Sheet-LibreOffice 2345678Document4 pagesFinal Trivia - Preparation Sheet-LibreOffice 2345678angel aguileraNo ratings yet
- Final Trivia - Preparation Sheet-LibreOfficeDocument4 pagesFinal Trivia - Preparation Sheet-LibreOfficeangel aguileraNo ratings yet
- Pharmacology of AntidepressantsDocument28 pagesPharmacology of Antidepressantsحيدر كريم سعيد حمزهNo ratings yet
- HW 2 Na 3Document7 pagesHW 2 Na 3Araw GabiNo ratings yet
- 1 - PharmacologyDocument18 pages1 - PharmacologyLuidgi MichelNo ratings yet
- Anti Depresan1Document39 pagesAnti Depresan1Akmal SafwanNo ratings yet
- Long Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreDocument55 pagesLong Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreGirish NagarNo ratings yet
- 2015 Psych DrugsDocument1 page2015 Psych DrugsmounicapaturuNo ratings yet
- Drug Study: Sedation, Dizziness/vertigo, Headache, Hypotension Sweating, Nausea, VomitingDocument1 pageDrug Study: Sedation, Dizziness/vertigo, Headache, Hypotension Sweating, Nausea, VomitingJoshua DavantesNo ratings yet
- AntidepressantsDocument4 pagesAntidepressantsAhmed MansourNo ratings yet
- Fin 20160705 Stimulants-And-Ssris PDFDocument2 pagesFin 20160705 Stimulants-And-Ssris PDFmahesh babu100% (1)
- Antidepressants: Elisabeth F. BildenDocument14 pagesAntidepressants: Elisabeth F. BildenSNo ratings yet
- Did Seizures QN 1Document31 pagesDid Seizures QN 1api-608647584No ratings yet
- 7 HBA DI Lecture 3 Spring 2023 2024Document26 pages7 HBA DI Lecture 3 Spring 2023 2024nonam7879No ratings yet
- Pharmacodynamics How Drugs WorkDocument21 pagesPharmacodynamics How Drugs WorkWen SilverNo ratings yet
- CNS Drugs-2Document34 pagesCNS Drugs-2semessor021245No ratings yet
- Drugs Used in Neuro PharmacologyDocument3 pagesDrugs Used in Neuro PharmacologyNabeel Kouka, MD, DO, MBA, MPH100% (1)
- PsychopharmacologyDocument8 pagesPsychopharmacologyzashileighNo ratings yet
- Drug Study TramadolDocument3 pagesDrug Study TramadolJulie LesmorasNo ratings yet
- Antidepressants UOLDocument85 pagesAntidepressants UOLYahya AhmedNo ratings yet
- Analytical Methods For Venlaflaxine Hydrochloride and Metabolites Determinations in Different MatricesDocument9 pagesAnalytical Methods For Venlaflaxine Hydrochloride and Metabolites Determinations in Different Matricesmadaci yasserNo ratings yet
- DRUGSTUDY Private RoomDocument5 pagesDRUGSTUDY Private RoomlordwinjohnbernardoNo ratings yet
- Figueroa, John Kyle PhillipDocument5 pagesFigueroa, John Kyle Phillipduca.danrainer02No ratings yet
- نسخة ANTI-ARRHYTHMIC 2Document28 pagesنسخة ANTI-ARRHYTHMIC 2ManWol JangNo ratings yet
- Running Head: Tricyclic Antidepresants 1Document3 pagesRunning Head: Tricyclic Antidepresants 1edwin nyagaNo ratings yet
- DrugofchoiceDocument16 pagesDrugofchoiceAbdualaziz AlmalkiNo ratings yet
- Notes File - MergedDocument99 pagesNotes File - MergedMian. Shoaib.No ratings yet
- Drug Data Classification Mechanism of Action Indications Contraindica Tion Adverse Reactions Nursing ResponsibilitiesDocument4 pagesDrug Data Classification Mechanism of Action Indications Contraindica Tion Adverse Reactions Nursing ResponsibilitiesFlorante AnibanNo ratings yet
- 2 Flash CardDocument14 pages2 Flash CardKhem BhattaraiNo ratings yet
- Antidepressant PharmacologyDocument57 pagesAntidepressant Pharmacologyrakesh meherNo ratings yet
- Drugs Affecting Gi System: Macaraig, Janine Mae Macalalad, Maria Abegail Macatangay, Maria LourdesDocument4 pagesDrugs Affecting Gi System: Macaraig, Janine Mae Macalalad, Maria Abegail Macatangay, Maria LourdesMicah Joy MacalaladNo ratings yet
- Drugs For Psyciatric DisordersDocument19 pagesDrugs For Psyciatric Disordersapi-36993610% (1)
- Introduction To Business Research Methods Vamsi KrishnaDocument25 pagesIntroduction To Business Research Methods Vamsi KrishnaEng MatanaNo ratings yet
- Hollow Fiber Membrane ContactorsDocument47 pagesHollow Fiber Membrane ContactorsEvelyn AntunesNo ratings yet
- Syllabus: M. Tech. Energy Management (Regular)Document28 pagesSyllabus: M. Tech. Energy Management (Regular)Digvijay SinghNo ratings yet
- Kundalini YogaDocument153 pagesKundalini Yogaprajjwal singhNo ratings yet
- Social Constructivism in Learning TheoryDocument7 pagesSocial Constructivism in Learning TheoryDebrah NavajjahNo ratings yet
- A Study On Effective Cash Management System Performance in Abc Techno Labs India Private LimitedDocument8 pagesA Study On Effective Cash Management System Performance in Abc Techno Labs India Private LimitedBabasaheb JawalgeNo ratings yet
- Copper Tube HandbookDocument66 pagesCopper Tube HandbookRafael Leonardo GomezNo ratings yet
- Atheism and Radical Skepticism Ibn Taymiyyahs Epistemic CritiqueDocument52 pagesAtheism and Radical Skepticism Ibn Taymiyyahs Epistemic CritiqueZaky MuzaffarNo ratings yet
- Physical Education and Physical FitnessDocument33 pagesPhysical Education and Physical FitnessKaitlinn Jamila AltatisNo ratings yet
- Create Microsoft-Signed Phishing DocumentsDocument9 pagesCreate Microsoft-Signed Phishing Documentsamir mansouriNo ratings yet
- Steroid Use in The Elderly: Postgraduate MedicineDocument8 pagesSteroid Use in The Elderly: Postgraduate MedicineValdi DwiramaNo ratings yet
- 130724Document20 pages130724Caracal MohNo ratings yet
- Medieval PhilosophyDocument39 pagesMedieval PhilosophyJorhen PanisNo ratings yet
- Alport'S SyndromeDocument8 pagesAlport'S SyndromeHemanth PrakashNo ratings yet
- Practice 9.đáDocument5 pagesPractice 9.đáNguyễn Vân QuỳnhhNo ratings yet
- Xdr2 Memory ArchitectureDocument2 pagesXdr2 Memory ArchitectureElizabethNo ratings yet
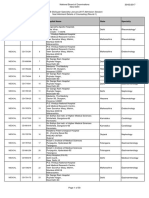
- SS Seat Allotment Details of Round-1Document50 pagesSS Seat Allotment Details of Round-1Suresh KumarNo ratings yet
- New Project ACI - PoltakDocument13 pagesNew Project ACI - PoltakD.b. TampubolonNo ratings yet
- Buddha and His ContemporariesDocument7 pagesBuddha and His ContemporariesAlok VermaNo ratings yet
- Informed Consent, Parental Permission & Assent: Jeffrey M. Cohen, PH.D., CIP President, HRP Associates, IncDocument26 pagesInformed Consent, Parental Permission & Assent: Jeffrey M. Cohen, PH.D., CIP President, HRP Associates, IncRoman Al MamunNo ratings yet
- Hasegawa v. GironDocument5 pagesHasegawa v. Gironjohaldiel muringNo ratings yet
- RegTech Medici Top-21Document38 pagesRegTech Medici Top-21ShakespeareWallaNo ratings yet
- CP E80.50 EPSWindowsClient UserGuide enDocument36 pagesCP E80.50 EPSWindowsClient UserGuide enmbaezasotoNo ratings yet
- Bas 98 Atex 2156 XDocument11 pagesBas 98 Atex 2156 XFelipe CamusNo ratings yet