Download as pdf or txt
You might also like
- Problem-Oriented Medical Diagnosis 7thDocument228 pagesProblem-Oriented Medical Diagnosis 7thnhtoan3286% (7)
- Prometheus Prometheus Texto Y Atlas de Anatomia Prometheus Textbook and Anatomy Atlas Spanish Edition by Michael SchunkeErik SchulteUdo SchumacherDocument6 pagesPrometheus Prometheus Texto Y Atlas de Anatomia Prometheus Textbook and Anatomy Atlas Spanish Edition by Michael SchunkeErik SchulteUdo SchumacherYukii Triby-a AnniimesztNo ratings yet
- Final Report On VolkswagenDocument70 pagesFinal Report On Volkswagenvjbhardwaj80% (20)
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument9 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribev_ratNo ratings yet
- Arentz 2017Document11 pagesArentz 2017Nur AwaliyaNo ratings yet
- Fertility Preservation Options For Transgender and Gender-Nonconforming IndividualsDocument7 pagesFertility Preservation Options For Transgender and Gender-Nonconforming IndividualsAnonymous 75M6uB3OwNo ratings yet
- Bardaweel 2015Document8 pagesBardaweel 2015sali Kriya.salimaNo ratings yet
- Healthcare Decisionmaking Targeting Women As Leaders of Change For Population Health 2376 127X 1000221Document7 pagesHealthcare Decisionmaking Targeting Women As Leaders of Change For Population Health 2376 127X 1000221Arifah UsrahNo ratings yet
- LANCET - 1 - Time For A Balanced Conversation About Menopause (Hickney Et Al., 2024)Document11 pagesLANCET - 1 - Time For A Balanced Conversation About Menopause (Hickney Et Al., 2024)Rebeca PeñuelaNo ratings yet
- Prospektive Cohort Study of Risk Factors For Breast Cancer in Post Menopausal WomenDocument9 pagesProspektive Cohort Study of Risk Factors For Breast Cancer in Post Menopausal WomenAdi KaswadiNo ratings yet
- Putting Abortion Pills Into Women's Hands: Realizing The Full Potential of Medical AbortionDocument4 pagesPutting Abortion Pills Into Women's Hands: Realizing The Full Potential of Medical AbortionFake_Me_No ratings yet
- 1 - Beyond Rep Health - BeirutDocument25 pages1 - Beyond Rep Health - BeirutAshima YadavNo ratings yet
- Capstone Final Paper MasterDocument24 pagesCapstone Final Paper Masterapi-667931371No ratings yet
- Research Final DraftDocument15 pagesResearch Final Draftapi-736869233No ratings yet
- Guttmacher Institute International Perspectives On Sexual and Reproductive HealthDocument11 pagesGuttmacher Institute International Perspectives On Sexual and Reproductive Healthandres57042No ratings yet
- Leslie V FarlandDocument10 pagesLeslie V FarlandtiaranindyNo ratings yet
- In Partial Fullfilment in Requirements in Practical Research 2Document7 pagesIn Partial Fullfilment in Requirements in Practical Research 2Famella JaneNo ratings yet
- Piis0002937809020031 PDFDocument6 pagesPiis0002937809020031 PDFRaisa AriesthaNo ratings yet
- Hope, Burden or Risk FPDocument24 pagesHope, Burden or Risk FPDolores GalloNo ratings yet
- NSG 106Document12 pagesNSG 106Anipah AmintaoNo ratings yet
- Call To Action For Contraceptive SafetyDocument16 pagesCall To Action For Contraceptive SafetyPopulation & Development Program (PopDev)No ratings yet
- Sexual and Reproductive Health OverviewDocument12 pagesSexual and Reproductive Health OverviewAssishNo ratings yet
- Contraceptive CHOICE Project SecuraDocument7 pagesContraceptive CHOICE Project Secura9C Hamdaan (HamdaanPro)No ratings yet
- Jcrpe 12 50 28 40Document13 pagesJcrpe 12 50 28 40Iis DamayantiNo ratings yet
- BHP Williams 2012Document6 pagesBHP Williams 2012AnyaNo ratings yet
- Sessionsetal High Alert Meds 919 JANDocument15 pagesSessionsetal High Alert Meds 919 JANichabojanNo ratings yet
- Pregnancy CAM TurkeyDocument10 pagesPregnancy CAM TurkeyTuğba ÖzcanNo ratings yet
- ResearchDocument15 pagesResearchapi-736973985No ratings yet
- Consecuencias Del DefectoDocument9 pagesConsecuencias Del DefectoChemo PantigozoNo ratings yet
- Individual, Provider and System Risk Factor For Breast and Cervical CancerDocument8 pagesIndividual, Provider and System Risk Factor For Breast and Cervical Cancervyvie89No ratings yet
- Cancer CervixDocument7 pagesCancer CervixarrigoNo ratings yet
- s41182 023 00531 XDocument12 pagess41182 023 00531 Xmanage logNo ratings yet
- Annotated BibDocument4 pagesAnnotated Bibapi-458216829No ratings yet
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- Jurnal Dr. BobbinDocument11 pagesJurnal Dr. BobbinNhiyar Indah HasniarNo ratings yet
- Christine Tagliaferri Rael Doyel Das Jose Bauermeister Cody Lentz Alex Carballo Diéguez Rebecca Giguere Rachel K. Scott Craig W. HendrixDocument19 pagesChristine Tagliaferri Rael Doyel Das Jose Bauermeister Cody Lentz Alex Carballo Diéguez Rebecca Giguere Rachel K. Scott Craig W. HendrixMichael DeniNo ratings yet
- Male Involvement and Maternal Health Outcomes: Systematic Review and Meta-AnalysisDocument9 pagesMale Involvement and Maternal Health Outcomes: Systematic Review and Meta-AnalysisRirinPakayaNo ratings yet
- ReportDocument13 pagesReportapi-663410827No ratings yet
- Ebsco Fulltext 2024 04 04Document6 pagesEbsco Fulltext 2024 04 04api-733572095No ratings yet
- 2021 - Disfunção Sexual em Mulheres Com CADocument12 pages2021 - Disfunção Sexual em Mulheres Com CAHeriksonNo ratings yet
- Use of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelDocument7 pagesUse of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelEndahNo ratings yet
- AnnotationDocument2 pagesAnnotationJannah Monaliza BambaNo ratings yet
- Gift 935 AsignmentDocument11 pagesGift 935 Asignmenttaizya cNo ratings yet
- Compet. de SaúdeDocument11 pagesCompet. de SaúdeLuciana OliveiraNo ratings yet
- Factors Associated With Contraceptive Choice and Inconsistent Method Use, United States, 2004Document11 pagesFactors Associated With Contraceptive Choice and Inconsistent Method Use, United States, 2004Amalia Dwi AryantiNo ratings yet
- 50 Years of Evolution of Contraception MedicineDocument2 pages50 Years of Evolution of Contraception MedicineardirshajiNo ratings yet
- Eary Marriege and Age Gap (Medical) 10-1108 - JHR-01-2021-0062Document13 pagesEary Marriege and Age Gap (Medical) 10-1108 - JHR-01-2021-0062Jwala AhirwarNo ratings yet
- Personalized Medicine Universe: Jack Kushner, MD, MGA, FACS, FICS, FAANS, HDGDocument4 pagesPersonalized Medicine Universe: Jack Kushner, MD, MGA, FACS, FICS, FAANS, HDGvara prasadNo ratings yet
- Promoting Safe Prescribing in Primary Care With A Contraceptive Vital Sign: A Cluster-Randomized Controlled TrialDocument7 pagesPromoting Safe Prescribing in Primary Care With A Contraceptive Vital Sign: A Cluster-Randomized Controlled TrialDookNo ratings yet
- Implicit Bias in Counseling For Permanent Contraception: Historical Context and Recommendations For CounselingDocument4 pagesImplicit Bias in Counseling For Permanent Contraception: Historical Context and Recommendations For CounselingyogurtNo ratings yet
- Artice 3Document10 pagesArtice 3Noreen MbabuNo ratings yet
- Maternal ThesisDocument10 pagesMaternal ThesisMerwynmae PobletinNo ratings yet
- Actualidades en AnticoncepciónDocument87 pagesActualidades en AnticoncepciónDamián López RangelNo ratings yet
- Misoprostol in Women's Hands: A Harm Reduction Strategy For Unsafe AbortionDocument3 pagesMisoprostol in Women's Hands: A Harm Reduction Strategy For Unsafe AbortionFake_Me_No ratings yet
- New Advances in Contraceptive Methods: ISSN 2347-3614Document10 pagesNew Advances in Contraceptive Methods: ISSN 2347-3614ArumaiselviNo ratings yet
- New Advances in Contraceptive Methods: ISSN 2347-3614Document10 pagesNew Advances in Contraceptive Methods: ISSN 2347-3614ArumaiselviNo ratings yet
- Factors Influencing Women's Preference To Select A Combined Hormonal Contraceptive Method: A Cross-Sectional Survey in LithuaniaDocument7 pagesFactors Influencing Women's Preference To Select A Combined Hormonal Contraceptive Method: A Cross-Sectional Survey in LithuaniaNur Syamsiah MNo ratings yet
- Refrence Article 1Document29 pagesRefrence Article 1Muhammad naveedNo ratings yet
- Preconception Health and Care: A Life Course ApproachFrom EverandPreconception Health and Care: A Life Course ApproachJill ShaweNo ratings yet
- Evolving Paradigms in Women's HealthDocument26 pagesEvolving Paradigms in Women's HealthSex & Gender Women's Health CollaborativeNo ratings yet
- Light, Zimbrunes, & Gomez-Lobo, 2017Document7 pagesLight, Zimbrunes, & Gomez-Lobo, 2017Anonymous 75M6uB3OwNo ratings yet
- The Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousDocument8 pagesThe Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousNoraNo ratings yet
- RH BillDocument13 pagesRH BillDr. Liza ManaloNo ratings yet
- Exploded Parts List VTB 370Document2 pagesExploded Parts List VTB 370Dusan MilosevicNo ratings yet
- Civil Engineering SustainabilityDocument55 pagesCivil Engineering SustainabilityEinstine Opiso100% (1)
- BASF Global Construction Brochure enDocument68 pagesBASF Global Construction Brochure enHector OliverNo ratings yet
- PRIME: Phobos Reconnaissance & International Mars ExplorationDocument1 pagePRIME: Phobos Reconnaissance & International Mars ExplorationRick FeedNo ratings yet
- HFJHDocument7 pagesHFJHMelly Fitriany SyamNo ratings yet
- GRAVITY - by Hobie Thompson and Sarah HavernDocument2 pagesGRAVITY - by Hobie Thompson and Sarah HavernJohn OsborneNo ratings yet
- Sales Final ExamDocument1 pageSales Final ExamIan PangNo ratings yet
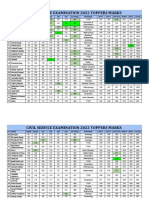
- Selected Candidates Marks CSE 2022Document6 pagesSelected Candidates Marks CSE 2022hara vardhan reddy naruNo ratings yet
- 1PRIMAMED SCHWERT 26. Laparatomy Instrument SetDocument4 pages1PRIMAMED SCHWERT 26. Laparatomy Instrument SetNanangGranDéNo ratings yet
- Sheabutter A+Document2 pagesSheabutter A+AmmuNo ratings yet
- MITSUBISHI OUTLANDER 2007 SERVICE MANUAL Volume 1 2 3 Engine LubricationDocument6 pagesMITSUBISHI OUTLANDER 2007 SERVICE MANUAL Volume 1 2 3 Engine LubricationAlberto José Meta GoudinhoNo ratings yet
- 1SDA066549R1 A2b 250 TMF 160 1600 3p F FDocument3 pages1SDA066549R1 A2b 250 TMF 160 1600 3p F FkjushnNo ratings yet
- Hook UpDocument104 pagesHook UpMeraj AlamNo ratings yet
- Performance of Digital Communication LabDocument4 pagesPerformance of Digital Communication LabFrogie HuniebieNo ratings yet
- Aggmax: Integrated Scrubbing SystemDocument15 pagesAggmax: Integrated Scrubbing SystemPoyaNo ratings yet
- SUMO PresentationDocument25 pagesSUMO Presentationarash_gourtaniNo ratings yet
- Carlip-Is Quantum Gravity Necessary? (2008)Document8 pagesCarlip-Is Quantum Gravity Necessary? (2008)bhpliaoNo ratings yet
- Reed Switch Appln PDFDocument15 pagesReed Switch Appln PDFJeeva BharathiNo ratings yet
- TND381 DDocument63 pagesTND381 DteomondoNo ratings yet
- Extravasation Mucocele - A Case ReportDocument3 pagesExtravasation Mucocele - A Case ReportSSR-IIJLS JournalNo ratings yet
- British Universal Columns and BeamsDocument4 pagesBritish Universal Columns and BeamsblaqhaqarNo ratings yet
- Hino 500 Series - Medium Duty Trucks DetailsDocument3 pagesHino 500 Series - Medium Duty Trucks DetailsJames ContiNo ratings yet
- TOPIC 27 Line SpectraDocument8 pagesTOPIC 27 Line SpectraSlamet WibowoNo ratings yet
- Remote Control ManualDocument16 pagesRemote Control ManualRajput PratiksinghNo ratings yet
- 21-4 - All - Use - Subject - To - JSTOR - Terms - and - CoDocument64 pages21-4 - All - Use - Subject - To - JSTOR - Terms - and - CoJavier Martinez EspuñaNo ratings yet
- Logic DiagramDocument1 pageLogic DiagramkapsarcNo ratings yet
- The Kapampangan Listorian - 103. 10 ARTS AND CRAFTS OF PAMPANGADocument21 pagesThe Kapampangan Listorian - 103. 10 ARTS AND CRAFTS OF PAMPANGAKlein HowergeNo ratings yet