Download as docx, pdf, or txt
You might also like
- Oscar Wilde - The Importance of Being EarnestDocument79 pagesOscar Wilde - The Importance of Being EarnestIvo Pires Das Neves100% (2)
- Case Write Up SURGERYDocument14 pagesCase Write Up SURGERYRahul Audenesen50% (2)
- Gastritis PresentationDocument23 pagesGastritis PresentationsiscapriliiaNo ratings yet
- CIVE263 Group Design Project Brief 2019-20 v6Document15 pagesCIVE263 Group Design Project Brief 2019-20 v6Marvin ItolondoNo ratings yet
- Unlearn Your Pain Chapter 5 TMSDocument17 pagesUnlearn Your Pain Chapter 5 TMSSyedNo ratings yet
- Case Presentation 1: Deviga Samy Velu Raja 012014100123Document47 pagesCase Presentation 1: Deviga Samy Velu Raja 012014100123Azizi RafieNo ratings yet
- Lifestyle Assessment FormDocument2 pagesLifestyle Assessment FormBbg011No ratings yet
- CVD Risk - Assessment - Form - Eng - FADocument1 pageCVD Risk - Assessment - Form - Eng - FAgmmateoNo ratings yet
- NEW PE FORM Bangayan Vhynee SDocument4 pagesNEW PE FORM Bangayan Vhynee SVhynee BangayanNo ratings yet
- PTPT Patient Health InformationDocument1 pagePTPT Patient Health InformationRachael DavisNo ratings yet
- CP1 Group A3 - 230811 - 090600Document37 pagesCP1 Group A3 - 230811 - 090600Muhammad HaziqNo ratings yet
- Haemorrhoid-Clinical Case Discussion 2Document15 pagesHaemorrhoid-Clinical Case Discussion 2jong siangNo ratings yet
- UTC SON Health Clinic: Student Name: Alyssa Matulich Date: 3/12/19Document5 pagesUTC SON Health Clinic: Student Name: Alyssa Matulich Date: 3/12/19api-456313554No ratings yet
- Case Write-Up 1Document22 pagesCase Write-Up 1Syed TalhaNo ratings yet
- "Please Do Something For My Period Pain": Max Brinsmead MB Bs PHD May 2015Document18 pages"Please Do Something For My Period Pain": Max Brinsmead MB Bs PHD May 2015NinaNo ratings yet
- General Medical History Form PDFDocument1 pageGeneral Medical History Form PDFണг. ധн¡тε H̶A̶T̶No ratings yet
- Dengue CBLDocument39 pagesDengue CBLsubhaNo ratings yet
- IPK - Pengantar PBL (Swamedikasi)Document30 pagesIPK - Pengantar PBL (Swamedikasi)Riani LetelayNo ratings yet
- Soap 3Document5 pagesSoap 3api-456313554No ratings yet
- Knowledge:: Knowledge Attitude and Practice Regarding Hypertension in General Population of IslamabadDocument2 pagesKnowledge:: Knowledge Attitude and Practice Regarding Hypertension in General Population of IslamabadAneesUrRahmanNo ratings yet
- H&P FormatDocument7 pagesH&P FormatRaffy Gutman100% (1)
- 02-03-2021 ADCON (Group 2, DR.)Document43 pages02-03-2021 ADCON (Group 2, DR.)Jolaine ValloNo ratings yet
- ANTENATAL ASSESSMENT Form 3Document4 pagesANTENATAL ASSESSMENT Form 3Kaku ManishaNo ratings yet
- Health CheckDocument9 pagesHealth Checkamoon08.arNo ratings yet
- AMBOSS CASES - Altered Bowel HabitsDocument9 pagesAMBOSS CASES - Altered Bowel HabitsFatimaNo ratings yet
- Dental and Medical History FormDocument1 pageDental and Medical History FormBon QuiapoNo ratings yet
- Antenatal Assessment Form 8Document4 pagesAntenatal Assessment Form 8Kaku Manisha100% (1)
- Case Write Up Obstructive UropathyDocument19 pagesCase Write Up Obstructive Uropathyjong siangNo ratings yet
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Document6 pagesPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieNo ratings yet
- OPD Case Protocol UTIDocument75 pagesOPD Case Protocol UTIJulienne Sanchez-SalazarNo ratings yet
- Medicalhistoryformpg 1Document2 pagesMedicalhistoryformpg 1reynanfrancebernabeNo ratings yet
- MSA Medical QuestionnaireDocument2 pagesMSA Medical QuestionnairekqbyvmqcdmNo ratings yet
- How To Write An HpiDocument9 pagesHow To Write An Hpiheidel anneNo ratings yet
- Living Donor Packet PDF September 2020Document8 pagesLiving Donor Packet PDF September 2020Emilia ColladoNo ratings yet
- Ws Viii Dyspepsia - Dr. Ignatia Sinta Murti, SP - Pd-KgehDocument79 pagesWs Viii Dyspepsia - Dr. Ignatia Sinta Murti, SP - Pd-KgehSriHandaryatiNo ratings yet
- A 20-Year-Old Female With Bloody DiarrhoeaDocument41 pagesA 20-Year-Old Female With Bloody DiarrhoeaMatthew LoopNo ratings yet
- Cwu - SurgeryDocument9 pagesCwu - SurgeryThiviyaa SivaselvamNo ratings yet
- M&M Hepatocellular CarcinomaDocument68 pagesM&M Hepatocellular Carcinomacharmaine BallanoNo ratings yet
- Patients History and Physical ExaminationDocument4 pagesPatients History and Physical Examinationeranga002No ratings yet
- Ward 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaDocument30 pagesWard 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaJoezelleNo ratings yet
- Antenatal Assessment - 1: TH THDocument4 pagesAntenatal Assessment - 1: TH THKaku ManishaNo ratings yet
- Soap Note 2 Alyssa MatulichDocument8 pagesSoap Note 2 Alyssa Matulichapi-456313554No ratings yet
- Deipan Arjunan - 20UMB03886 - CWU 2 - IM Group 1Document30 pagesDeipan Arjunan - 20UMB03886 - CWU 2 - IM Group 1Deipan ArjunanNo ratings yet
- GORDONS Durano Aireen E.Document4 pagesGORDONS Durano Aireen E.Doneva Lyn MedinaNo ratings yet
- Acute CaseDocument20 pagesAcute CaseNarendran MuthusamyNo ratings yet
- Acute PancreatitisDocument5 pagesAcute PancreatitisSophia RubiaNo ratings yet
- Health Assessment ExampleDocument2 pagesHealth Assessment Exampleakoeljames8543No ratings yet
- Liver Function Tests - CP - Pharmd 4th YearDocument62 pagesLiver Function Tests - CP - Pharmd 4th Yearsri deepika sri deepikaNo ratings yet
- Gastrointestinal History - VomitingDocument2 pagesGastrointestinal History - VomitingAmjad_2020No ratings yet
- CaseDocument38 pagesCase--No ratings yet
- The Digestive Health Assessment PDFDocument1 pageThe Digestive Health Assessment PDFStaci MunroNo ratings yet
- University of BoholDocument5 pagesUniversity of BoholMARIA CHARMIN M. MEJIANo ratings yet
- Health SummaryDocument2 pagesHealth SummaryFrank RenNo ratings yet
- Antenatal Assessment Form 14Document4 pagesAntenatal Assessment Form 14Kaku Manisha100% (1)
- Dengue Reporting FormDocument5 pagesDengue Reporting FormAbhi ShahNo ratings yet
- Clinical Presentation On ObgDocument20 pagesClinical Presentation On ObgValarmathiNo ratings yet
- Colic Abdomen E.C Peritonitis E.C Perforasi Gaster + AKI + Dehidrasi Ringan-SedangDocument22 pagesColic Abdomen E.C Peritonitis E.C Perforasi Gaster + AKI + Dehidrasi Ringan-SedangInesia Putri WulandariNo ratings yet
- PagesDocument4 pagesPagesjanicewhismanNo ratings yet
- Be Review of Systems Questionairet 122714Document1 pageBe Review of Systems Questionairet 122714Djev David DazaNo ratings yet
- ANTENATAL ASSESSMENT Form 13Document4 pagesANTENATAL ASSESSMENT Form 13Kaku ManishaNo ratings yet
- Adult Med HXDocument2 pagesAdult Med HXapi-3868874No ratings yet
- ANTENATAL ASSESSMENT Form 12Document4 pagesANTENATAL ASSESSMENT Form 12Kaku Manisha100% (2)
- IBS Irritable Bowel Syndrome A Gastroenterologist Answers Your Questions: What Is It? Why Do I Have It? How Can I Get Well?From EverandIBS Irritable Bowel Syndrome A Gastroenterologist Answers Your Questions: What Is It? Why Do I Have It? How Can I Get Well?No ratings yet
- Nwankwo Ukamaka ChiomaDocument4 pagesNwankwo Ukamaka ChiomaMarvin ItolondoNo ratings yet
- Solution 1Document14 pagesSolution 1Marvin ItolondoNo ratings yet
- 01Document1 page01Marvin ItolondoNo ratings yet
- SsDocument3 pagesSsMarvin ItolondoNo ratings yet
- Vassignment 1Document4 pagesVassignment 1Marvin ItolondoNo ratings yet
- Phase 2Document10 pagesPhase 2Marvin ItolondoNo ratings yet
- Mama Helen HouseDocument1 pageMama Helen HouseMarvin ItolondoNo ratings yet
- Set 2Document8 pagesSet 2Marvin ItolondoNo ratings yet
- Saudi Arabia Stock MarketDocument16 pagesSaudi Arabia Stock MarketMarvin ItolondoNo ratings yet
- Requiem Mass For Lawrence Mullama ItolondoDocument8 pagesRequiem Mass For Lawrence Mullama ItolondoMarvin ItolondoNo ratings yet
- Mama Helen FDocument10 pagesMama Helen FMarvin ItolondoNo ratings yet
- WWWWWDocument1 pageWWWWWMarvin ItolondoNo ratings yet
- Visio-Drawing1 Copy-1691823179070Document1 pageVisio-Drawing1 Copy-1691823179070Marvin ItolondoNo ratings yet
- Kabasis-15 - BBS Concrete Sleeper DetailsDocument1 pageKabasis-15 - BBS Concrete Sleeper DetailsMarvin ItolondoNo ratings yet
- Geometric Design of A Highway Using Autocad Civil 3D: Presenter NameDocument11 pagesGeometric Design of A Highway Using Autocad Civil 3D: Presenter NameMarvin ItolondoNo ratings yet
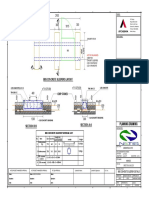
- Planning Drawing: Bts Concrete Sleepers Material ListDocument1 pagePlanning Drawing: Bts Concrete Sleepers Material ListMarvin ItolondoNo ratings yet
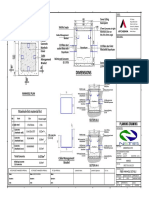
- Kabasis-12 - Generator Concrete SleeperDocument1 pageKabasis-12 - Generator Concrete SleeperMarvin ItolondoNo ratings yet
- CIV E 482 - Design Lab Stromwater Management: What Is The Importance of Today's Lab?Document14 pagesCIV E 482 - Design Lab Stromwater Management: What Is The Importance of Today's Lab?Marvin ItolondoNo ratings yet
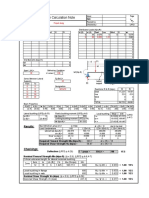
- Steel I - Beam Calculation Note Steel I - Beam Calculation NoteDocument2 pagesSteel I - Beam Calculation Note Steel I - Beam Calculation NoteMarvin ItolondoNo ratings yet
- Project Designing A Habitat in MarsDocument13 pagesProject Designing A Habitat in MarsMarvin ItolondoNo ratings yet
- The Report: Sewer DesignDocument20 pagesThe Report: Sewer DesignMarvin ItolondoNo ratings yet
- Geometric Design of A Highway Using Autocad Civil 3D: Presenter NameDocument12 pagesGeometric Design of A Highway Using Autocad Civil 3D: Presenter NameMarvin ItolondoNo ratings yet
- Factoring The Load Demand: SolutionDocument8 pagesFactoring The Load Demand: SolutionMarvin ItolondoNo ratings yet
- Kabasis-16 - Fiber Manhole DetailsDocument1 pageKabasis-16 - Fiber Manhole DetailsMarvin ItolondoNo ratings yet
- Freddie Jeffries - Fang You - Hajie Shan - Linghao Chen - Mischa Patel - Hywel BeasdaleDocument39 pagesFreddie Jeffries - Fang You - Hajie Shan - Linghao Chen - Mischa Patel - Hywel BeasdaleMarvin ItolondoNo ratings yet
- Myofascial PainDocument8 pagesMyofascial PainEnyaw Droffats100% (1)
- Azusa Pacific University School of Nursing GNRS 588: Advanced Nursing Care For Adults Comprehensive Care Plan #: - 1Document18 pagesAzusa Pacific University School of Nursing GNRS 588: Advanced Nursing Care For Adults Comprehensive Care Plan #: - 1api-325691098No ratings yet
- Drug Study: Valerie V. Villanueva BN3-CDocument1 pageDrug Study: Valerie V. Villanueva BN3-CValerie VillanuevaNo ratings yet
- Evaluation of The Patient With Hip PainDocument12 pagesEvaluation of The Patient With Hip PainannisaNo ratings yet
- New Questions 2015 DentalDocument115 pagesNew Questions 2015 DentalDr-ShadyElOssailyNo ratings yet
- Chronic Kidney Disease Malaysian CPG 2011Document22 pagesChronic Kidney Disease Malaysian CPG 2011aideeh31100% (1)
- Pharmacoepidemiology Pharmacoepidemiology At3: Studies Using Automated Databases GDocument27 pagesPharmacoepidemiology Pharmacoepidemiology At3: Studies Using Automated Databases GRuth Vargas GonzalesNo ratings yet
- Undergraduate Nutrition Nursing, Health Polytechnic of YogyakartaDocument1 pageUndergraduate Nutrition Nursing, Health Polytechnic of YogyakartaAditya hari KusumaNo ratings yet
- Fluid TherapyDocument9 pagesFluid TherapyMadiha MadiNo ratings yet
- Ruminant LAM NotesDocument11 pagesRuminant LAM NotesAsh-Lee HugginsNo ratings yet
- How Fast Food Affects Thai Teenagers LifeDocument15 pagesHow Fast Food Affects Thai Teenagers Lifeapi-263388641No ratings yet
- London SmogDocument7 pagesLondon SmogRitu PandeNo ratings yet
- Night Sweats: A Systematic Review of The LiteratureDocument16 pagesNight Sweats: A Systematic Review of The LiteraturesyafahalimNo ratings yet
- ORAL-PATH-QP.-2021 RguhsDocument22 pagesORAL-PATH-QP.-2021 RguhsgautNo ratings yet
- ORDINATIO Heel ANARANJADO Productos en BTQ PDFDocument212 pagesORDINATIO Heel ANARANJADO Productos en BTQ PDFVinicio RevelantNo ratings yet
- Heart Failure and Liver DiseaseDocument11 pagesHeart Failure and Liver DiseaseFreddy PanjaitanNo ratings yet
- NUX VOMICA - HOMOEOPATHIC MATERIA MEDICA - by William BOERICKEDocument1 pageNUX VOMICA - HOMOEOPATHIC MATERIA MEDICA - by William BOERICKEASHAR JUMAN 17No ratings yet
- CRP TestDocument7 pagesCRP TestYOGANANTH mscasNo ratings yet
- Ed001 The Biological ClockDocument2 pagesEd001 The Biological ClockAnonymous YaOsE6nNo ratings yet
- Cytochemical Stains in Haematology PDFDocument3 pagesCytochemical Stains in Haematology PDFABHINABA GUPTANo ratings yet
- 9th-10-11th May-2016 Papers (1650 MCQS) by Amlodipine Besylate PDFDocument161 pages9th-10-11th May-2016 Papers (1650 MCQS) by Amlodipine Besylate PDFAmlodipine BesylateNo ratings yet
- Cardiovascular Physical TherapyDocument206 pagesCardiovascular Physical TherapyJuanitoCabatañaLimIII100% (2)
- Dermovate Cream: (Clobetasol Propionate)Document4 pagesDermovate Cream: (Clobetasol Propionate)Ian Joseph Dionisio TenorioNo ratings yet
- Health Teaching For AsthmaDocument2 pagesHealth Teaching For AsthmaDianne MaeNo ratings yet
- Micu MedsDocument3 pagesMicu MedsanreilegardeNo ratings yet
- DLP-Bohol - Science9 Q1 W2 D4Document6 pagesDLP-Bohol - Science9 Q1 W2 D4Marfe MontelibanoNo ratings yet
- Philippine College of Physicians Daily Census Ward Hospital de Los Santos-Sti Medical CenterDocument22 pagesPhilippine College of Physicians Daily Census Ward Hospital de Los Santos-Sti Medical Centercruz_johnraymondNo ratings yet
- Level 12 Analogies 2 PDFDocument3 pagesLevel 12 Analogies 2 PDFCarlson AberinNo ratings yet