
(OS 213 Cardio B) E01-T02-History Taking in Adults With CVD
(OS 213 Cardio B) E01-T02-History Taking in Adults With CVD
You might also like
- Acute and Chronic Wounds - Current Management Concepts (PDFDrive)Document1,872 pagesAcute and Chronic Wounds - Current Management Concepts (PDFDrive)Tasha FarahNo ratings yet
- Good Practice: Communication Skills in English For The Medical PractitionerDocument13 pagesGood Practice: Communication Skills in English For The Medical PractitionerFarid Iqbal100% (1)
- 02 - 24 - Psychiatric Assessment PDFDocument7 pages02 - 24 - Psychiatric Assessment PDFAbi Sulit100% (1)
- Nssa - Si 68 - 1990Document187 pagesNssa - Si 68 - 1990Courage50% (2)
- 01b Calgary Cambridge Framework - Basic and DetailedDocument2 pages01b Calgary Cambridge Framework - Basic and DetailedJohn Sebastian Bittner SolisNo ratings yet
- NCMP1O3 - Community Health NursingDocument13 pagesNCMP1O3 - Community Health NursingNicole Faith L. NacarioNo ratings yet
- Communication Skills For Medical InterviewDocument26 pagesCommunication Skills For Medical InterviewArya Dananjaya100% (1)
- PPN2010220W202420week20420Nursing20Process20P120 (Final)Document65 pagesPPN2010220W202420week20420Nursing20Process20P120 (Final)5679No ratings yet
- BegaycDocument10 pagesBegaycapi-549236958No ratings yet
- Professional Development: Lynn Ly NURS 478Document11 pagesProfessional Development: Lynn Ly NURS 478api-740100360No ratings yet
- (CLR) 1.01 - Introduction To Clinical Research and Appraising An Article On TherapyDocument11 pages(CLR) 1.01 - Introduction To Clinical Research and Appraising An Article On Therapymuyot.ac.sNo ratings yet
- 01.07.01 Interviewing Skills - Filipino Medical LanguageDocument4 pages01.07.01 Interviewing Skills - Filipino Medical LanguageMikmik DGNo ratings yet
- Ncmp1o3 CHN Rle Midterms Reviewer PDFDocument13 pagesNcmp1o3 CHN Rle Midterms Reviewer PDFfeelthelovephNo ratings yet
- Importance of Preparedness Characteristics For Clinical Practice Perspectives of Nursing Students in DMC CollegeDocument87 pagesImportance of Preparedness Characteristics For Clinical Practice Perspectives of Nursing Students in DMC CollegeJohn Del YuntingNo ratings yet
- Student - PPN 102 W24 Week 4 Nursing Process P1Document44 pagesStudent - PPN 102 W24 Week 4 Nursing Process P1phuongphuonganhanh171203No ratings yet
- MATERIAL COMPLEMENTAR NHCP Guia para Conversas DifíceisDocument9 pagesMATERIAL COMPLEMENTAR NHCP Guia para Conversas DifíceisCarla HigaNo ratings yet
- Funda NotesDocument13 pagesFunda NotesMa. Christina Jane OmambacNo ratings yet
- NR 1Document24 pagesNR 1Kpop LoverNo ratings yet
- The Nursing ProcessDocument11 pagesThe Nursing ProcessRamzen Raphael DomingoNo ratings yet
- Better Handoffs. Safer CareDocument49 pagesBetter Handoffs. Safer CareSatanan DamrisuNo ratings yet
- Good Practice Student's BookDocument24 pagesGood Practice Student's BookHome ClassesNo ratings yet
- Research PrelimDocument23 pagesResearch PrelimDONNA MAE MABALOTNo ratings yet
- Fhatin Nurain Azrienna BT Mohd Fadly A158181 Paediatrics DR Wan Nurulhuda Wan MD ZinDocument2 pagesFhatin Nurain Azrienna BT Mohd Fadly A158181 Paediatrics DR Wan Nurulhuda Wan MD ZinFhatin Nurain Azrienna Binti Mohd FadlyNo ratings yet
- (EPI) 5.04 Analytic Observational Research Designs - Dr. NailesDocument10 pages(EPI) 5.04 Analytic Observational Research Designs - Dr. NailesJoshua CruzNo ratings yet
- CHP-7-NURSING PROCESS - Wecompress - ComDocument91 pagesCHP-7-NURSING PROCESS - Wecompress - ComAkhilesh TiwariNo ratings yet
- Midterms ReviewerDocument9 pagesMidterms Reviewerley.leslie1606No ratings yet
- Komunikasi Dan Etika: (Pasien Teman Sejawat, Antar Profesi)Document38 pagesKomunikasi Dan Etika: (Pasien Teman Sejawat, Antar Profesi)Muhammad Fadlillah Al FitrahNo ratings yet
- A-Year6 Consult Models (A) 5-9-2022Document53 pagesA-Year6 Consult Models (A) 5-9-2022Rahaf AlhubailNo ratings yet
- Consultaion ModelsDocument57 pagesConsultaion ModelsNoora AlmuailiNo ratings yet
- Nres ReviewerDocument16 pagesNres Reviewerkirstenfrancine28No ratings yet
- Professional Development 2Document11 pagesProfessional Development 2api-666238831No ratings yet
- NCA 2 12 Nursing Research Celajes Cerro ChucaDocument22 pagesNCA 2 12 Nursing Research Celajes Cerro ChucaFrancis Raphael PitogoNo ratings yet
- BeggvDocument11 pagesBeggvapi-450497170No ratings yet
- n479 Professional DevelopmentDocument11 pagesn479 Professional Developmentapi-509458762No ratings yet
- TomasjDocument10 pagesTomasjapi-457350761No ratings yet
- Leadership Development PPDocument11 pagesLeadership Development PPapi-643545031No ratings yet
- NCM 109 - Written Output 1Document8 pagesNCM 109 - Written Output 1Jayar ArabiaNo ratings yet
- Scholarly Paper CapstoneDocument6 pagesScholarly Paper Capstoneapi-662404021No ratings yet
- Clincal 3 MidtermDocument7 pagesClincal 3 Midtermapi-363629062No ratings yet
- 479 Professional DevelopmentDocument13 pages479 Professional Developmentapi-708880014No ratings yet
- NCM 101 Endterm NotessssDocument590 pagesNCM 101 Endterm NotessssJude Marie Claire DequiñaNo ratings yet
- Title Page HeheDocument10 pagesTitle Page Heheゝ NicoleNo ratings yet
- NCM 101 Prelim NotessDocument105 pagesNCM 101 Prelim NotessJude Marie Claire DequiñaNo ratings yet
- Cet Final For ClinicalDocument7 pagesCet Final For Clinicalapi-351971578No ratings yet
- Trans 16 FMPDocument6 pagesTrans 16 FMPPeach Amparo BuguinaNo ratings yet
- Types of Family-Nurse ContactDocument5 pagesTypes of Family-Nurse ContactBritthaney BuladacoNo ratings yet
- Lesson 2 Reviewer - Decision Making and PlanningDocument3 pagesLesson 2 Reviewer - Decision Making and PlanningmanuelNo ratings yet
- Nursing Research 1 PrelimDocument3 pagesNursing Research 1 PrelimKM PanganibanNo ratings yet
- 06 - LEC Family Nursing ProcessDocument10 pages06 - LEC Family Nursing ProcessJAN CAMILLE LENONNo ratings yet
- ITNRDocument6 pagesITNRJennifer AlamonNo ratings yet
- Logic ReviewerrrrDocument6 pagesLogic Reviewerrrrpatrickparil01.ppNo ratings yet
- 2.1 NCM 210 RLE - Types of Family-Nurse ContactDocument6 pages2.1 NCM 210 RLE - Types of Family-Nurse ContactLYRIZZA LEA BHEA DESIATANo ratings yet
- Meresum Jurnal KeperawatanDocument9 pagesMeresum Jurnal KeperawatanRicky Ahmad FahreziNo ratings yet
- MFD Level of Geriatric Care Given Among ElderlyDocument98 pagesMFD Level of Geriatric Care Given Among Elderlydelavegajealou00No ratings yet
- Nur412 Group 4 RleDocument57 pagesNur412 Group 4 RleKennedy PelicoNo ratings yet
- CHAPTER 2 LectureDocument5 pagesCHAPTER 2 LectureChristian Josh EspedillonNo ratings yet
- 1427 - Rana Kachouh Nursing Process HammoudDocument54 pages1427 - Rana Kachouh Nursing Process HammoudRumela Ganguly ChakrabortyNo ratings yet
- Professional Development PresentationDocument12 pagesProfessional Development Presentationapi-642955149No ratings yet
- Nursing Case Study OncologyDocument22 pagesNursing Case Study OncologyFuntwo FauzanNo ratings yet
- Senior Project Presentation 1Document30 pagesSenior Project Presentation 1api-732018343No ratings yet
- Student's Signature: - DateDocument7 pagesStudent's Signature: - Dateapi-384261910No ratings yet
- Treatment Planning in Restorative Dentistry and Implant ProsthodonticsFrom EverandTreatment Planning in Restorative Dentistry and Implant ProsthodonticsNo ratings yet
- Nalbuphine - Drug StudyDocument3 pagesNalbuphine - Drug Studygrazel calubNo ratings yet
- Doctor-Patient-Relationship-.ppt (1) 2Document28 pagesDoctor-Patient-Relationship-.ppt (1) 2nketjimotswaledi100% (1)
- Patna HospitalDocument5 pagesPatna Hospitalmahwish khanNo ratings yet
- Review On Inflammatory DisesesDocument21 pagesReview On Inflammatory Disesesdigitalmazdoor5201No ratings yet
- Validation of The Adolescent Self Esteem QuestionnaireDocument34 pagesValidation of The Adolescent Self Esteem Questionnairevijayalakshmi100% (1)
- Why I Am Intersted in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The FutureDocument3 pagesWhy I Am Intersted in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The FuturehermawanNo ratings yet
- Nurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationDocument4 pagesNurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationEmma WatsonNo ratings yet
- Campbell, James - CV - 25 Feb 2016Document42 pagesCampbell, James - CV - 25 Feb 2016meenakshi.r.agrawalNo ratings yet
- Safe Work Method Statement For High Risk Construction Work (SWMS) TemplateDocument3 pagesSafe Work Method Statement For High Risk Construction Work (SWMS) TemplateMarulituaNo ratings yet
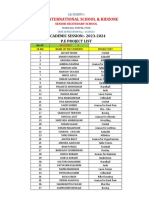
- XII A PE Project ListDocument2 pagesXII A PE Project ListShriyanshi DasNo ratings yet
- SAGDocument229 pagesSAGMalshej Goat Farm All about goatsNo ratings yet
- Antiscale (DEQUEST SPE 0001)Document7 pagesAntiscale (DEQUEST SPE 0001)mahdi rasoulianNo ratings yet
- Ethical Case StudiesDocument9 pagesEthical Case StudiesًNo ratings yet
- Standard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisDocument11 pagesStandard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisAbuNo ratings yet
- NCM 114 Care For Older Adults MODULE 5Document5 pagesNCM 114 Care For Older Adults MODULE 5Meryville JacildoNo ratings yet
- 1205WHO Vs GMP Slide 16 OnwardsDocument31 pages1205WHO Vs GMP Slide 16 OnwardsTumma RamaraoNo ratings yet
- DN4 Assessment ToolDocument1 pageDN4 Assessment ToolrahmiNo ratings yet
- AV eIFU 10223671 Mg-En V03Document68 pagesAV eIFU 10223671 Mg-En V03Goutham RevuruNo ratings yet
- New Graduate RN Cover Letter SamplesDocument7 pagesNew Graduate RN Cover Letter Samplesf60pk9dc100% (3)
- Ethics Unit 2Document22 pagesEthics Unit 2SaniNo ratings yet
- 2 Ethical Aspects of Nursing ResearchDocument35 pages2 Ethical Aspects of Nursing ResearchGrape JuiceNo ratings yet
- Psychological Testing Report-1Document80 pagesPsychological Testing Report-1Laveeza KhurramNo ratings yet
- Griffith'S Experiment: Frederick Griffith (1877-1941) Was A British Bacteriologist Whose Focus Was TheDocument16 pagesGriffith'S Experiment: Frederick Griffith (1877-1941) Was A British Bacteriologist Whose Focus Was TheKeljang MoktanNo ratings yet
- Operational Control Procedure For Noise MonitoringDocument2 pagesOperational Control Procedure For Noise MonitoringKishan MauryaNo ratings yet
- 5 Sciatica Exercises For Pain Relief (With Pictures) : Back IntelligenceDocument26 pages5 Sciatica Exercises For Pain Relief (With Pictures) : Back Intelligenceanand sahu100% (1)
- 358 Developmental DomainsDocument2 pages358 Developmental Domainsapi-285147481No ratings yet
- Hlthaff 23 4 202 PDFDocument11 pagesHlthaff 23 4 202 PDFexaNo ratings yet
- The National Bursary PolicyDocument20 pagesThe National Bursary PolicyCrazyCrafterYTNo ratings yet

























































































Download as pdf or txt
You might also like
- Acute and Chronic Wounds - Current Management Concepts (PDFDrive)Document1,872 pagesAcute and Chronic Wounds - Current Management Concepts (PDFDrive)Tasha FarahNo ratings yet
- Good Practice: Communication Skills in English For The Medical PractitionerDocument13 pagesGood Practice: Communication Skills in English For The Medical PractitionerFarid Iqbal100% (1)
- 02 - 24 - Psychiatric Assessment PDFDocument7 pages02 - 24 - Psychiatric Assessment PDFAbi Sulit100% (1)
- Nssa - Si 68 - 1990Document187 pagesNssa - Si 68 - 1990Courage50% (2)
- 01b Calgary Cambridge Framework - Basic and DetailedDocument2 pages01b Calgary Cambridge Framework - Basic and DetailedJohn Sebastian Bittner SolisNo ratings yet
- NCMP1O3 - Community Health NursingDocument13 pagesNCMP1O3 - Community Health NursingNicole Faith L. NacarioNo ratings yet
- Communication Skills For Medical InterviewDocument26 pagesCommunication Skills For Medical InterviewArya Dananjaya100% (1)
- PPN2010220W202420week20420Nursing20Process20P120 (Final)Document65 pagesPPN2010220W202420week20420Nursing20Process20P120 (Final)5679No ratings yet
- BegaycDocument10 pagesBegaycapi-549236958No ratings yet
- Professional Development: Lynn Ly NURS 478Document11 pagesProfessional Development: Lynn Ly NURS 478api-740100360No ratings yet
- (CLR) 1.01 - Introduction To Clinical Research and Appraising An Article On TherapyDocument11 pages(CLR) 1.01 - Introduction To Clinical Research and Appraising An Article On Therapymuyot.ac.sNo ratings yet
- 01.07.01 Interviewing Skills - Filipino Medical LanguageDocument4 pages01.07.01 Interviewing Skills - Filipino Medical LanguageMikmik DGNo ratings yet
- Ncmp1o3 CHN Rle Midterms Reviewer PDFDocument13 pagesNcmp1o3 CHN Rle Midterms Reviewer PDFfeelthelovephNo ratings yet
- Importance of Preparedness Characteristics For Clinical Practice Perspectives of Nursing Students in DMC CollegeDocument87 pagesImportance of Preparedness Characteristics For Clinical Practice Perspectives of Nursing Students in DMC CollegeJohn Del YuntingNo ratings yet
- Student - PPN 102 W24 Week 4 Nursing Process P1Document44 pagesStudent - PPN 102 W24 Week 4 Nursing Process P1phuongphuonganhanh171203No ratings yet
- MATERIAL COMPLEMENTAR NHCP Guia para Conversas DifíceisDocument9 pagesMATERIAL COMPLEMENTAR NHCP Guia para Conversas DifíceisCarla HigaNo ratings yet
- Funda NotesDocument13 pagesFunda NotesMa. Christina Jane OmambacNo ratings yet
- NR 1Document24 pagesNR 1Kpop LoverNo ratings yet
- The Nursing ProcessDocument11 pagesThe Nursing ProcessRamzen Raphael DomingoNo ratings yet
- Better Handoffs. Safer CareDocument49 pagesBetter Handoffs. Safer CareSatanan DamrisuNo ratings yet
- Good Practice Student's BookDocument24 pagesGood Practice Student's BookHome ClassesNo ratings yet
- Research PrelimDocument23 pagesResearch PrelimDONNA MAE MABALOTNo ratings yet
- Fhatin Nurain Azrienna BT Mohd Fadly A158181 Paediatrics DR Wan Nurulhuda Wan MD ZinDocument2 pagesFhatin Nurain Azrienna BT Mohd Fadly A158181 Paediatrics DR Wan Nurulhuda Wan MD ZinFhatin Nurain Azrienna Binti Mohd FadlyNo ratings yet
- (EPI) 5.04 Analytic Observational Research Designs - Dr. NailesDocument10 pages(EPI) 5.04 Analytic Observational Research Designs - Dr. NailesJoshua CruzNo ratings yet
- CHP-7-NURSING PROCESS - Wecompress - ComDocument91 pagesCHP-7-NURSING PROCESS - Wecompress - ComAkhilesh TiwariNo ratings yet
- Midterms ReviewerDocument9 pagesMidterms Reviewerley.leslie1606No ratings yet
- Komunikasi Dan Etika: (Pasien Teman Sejawat, Antar Profesi)Document38 pagesKomunikasi Dan Etika: (Pasien Teman Sejawat, Antar Profesi)Muhammad Fadlillah Al FitrahNo ratings yet
- A-Year6 Consult Models (A) 5-9-2022Document53 pagesA-Year6 Consult Models (A) 5-9-2022Rahaf AlhubailNo ratings yet
- Consultaion ModelsDocument57 pagesConsultaion ModelsNoora AlmuailiNo ratings yet
- Nres ReviewerDocument16 pagesNres Reviewerkirstenfrancine28No ratings yet
- Professional Development 2Document11 pagesProfessional Development 2api-666238831No ratings yet
- NCA 2 12 Nursing Research Celajes Cerro ChucaDocument22 pagesNCA 2 12 Nursing Research Celajes Cerro ChucaFrancis Raphael PitogoNo ratings yet
- BeggvDocument11 pagesBeggvapi-450497170No ratings yet
- n479 Professional DevelopmentDocument11 pagesn479 Professional Developmentapi-509458762No ratings yet
- TomasjDocument10 pagesTomasjapi-457350761No ratings yet
- Leadership Development PPDocument11 pagesLeadership Development PPapi-643545031No ratings yet
- NCM 109 - Written Output 1Document8 pagesNCM 109 - Written Output 1Jayar ArabiaNo ratings yet
- Scholarly Paper CapstoneDocument6 pagesScholarly Paper Capstoneapi-662404021No ratings yet
- Clincal 3 MidtermDocument7 pagesClincal 3 Midtermapi-363629062No ratings yet
- 479 Professional DevelopmentDocument13 pages479 Professional Developmentapi-708880014No ratings yet
- NCM 101 Endterm NotessssDocument590 pagesNCM 101 Endterm NotessssJude Marie Claire DequiñaNo ratings yet
- Title Page HeheDocument10 pagesTitle Page Heheゝ NicoleNo ratings yet
- NCM 101 Prelim NotessDocument105 pagesNCM 101 Prelim NotessJude Marie Claire DequiñaNo ratings yet
- Cet Final For ClinicalDocument7 pagesCet Final For Clinicalapi-351971578No ratings yet
- Trans 16 FMPDocument6 pagesTrans 16 FMPPeach Amparo BuguinaNo ratings yet
- Types of Family-Nurse ContactDocument5 pagesTypes of Family-Nurse ContactBritthaney BuladacoNo ratings yet
- Lesson 2 Reviewer - Decision Making and PlanningDocument3 pagesLesson 2 Reviewer - Decision Making and PlanningmanuelNo ratings yet
- Nursing Research 1 PrelimDocument3 pagesNursing Research 1 PrelimKM PanganibanNo ratings yet
- 06 - LEC Family Nursing ProcessDocument10 pages06 - LEC Family Nursing ProcessJAN CAMILLE LENONNo ratings yet
- ITNRDocument6 pagesITNRJennifer AlamonNo ratings yet
- Logic ReviewerrrrDocument6 pagesLogic Reviewerrrrpatrickparil01.ppNo ratings yet
- 2.1 NCM 210 RLE - Types of Family-Nurse ContactDocument6 pages2.1 NCM 210 RLE - Types of Family-Nurse ContactLYRIZZA LEA BHEA DESIATANo ratings yet
- Meresum Jurnal KeperawatanDocument9 pagesMeresum Jurnal KeperawatanRicky Ahmad FahreziNo ratings yet
- MFD Level of Geriatric Care Given Among ElderlyDocument98 pagesMFD Level of Geriatric Care Given Among Elderlydelavegajealou00No ratings yet
- Nur412 Group 4 RleDocument57 pagesNur412 Group 4 RleKennedy PelicoNo ratings yet
- CHAPTER 2 LectureDocument5 pagesCHAPTER 2 LectureChristian Josh EspedillonNo ratings yet
- 1427 - Rana Kachouh Nursing Process HammoudDocument54 pages1427 - Rana Kachouh Nursing Process HammoudRumela Ganguly ChakrabortyNo ratings yet
- Professional Development PresentationDocument12 pagesProfessional Development Presentationapi-642955149No ratings yet
- Nursing Case Study OncologyDocument22 pagesNursing Case Study OncologyFuntwo FauzanNo ratings yet
- Senior Project Presentation 1Document30 pagesSenior Project Presentation 1api-732018343No ratings yet
- Student's Signature: - DateDocument7 pagesStudent's Signature: - Dateapi-384261910No ratings yet
- Treatment Planning in Restorative Dentistry and Implant ProsthodonticsFrom EverandTreatment Planning in Restorative Dentistry and Implant ProsthodonticsNo ratings yet
- Nalbuphine - Drug StudyDocument3 pagesNalbuphine - Drug Studygrazel calubNo ratings yet
- Doctor-Patient-Relationship-.ppt (1) 2Document28 pagesDoctor-Patient-Relationship-.ppt (1) 2nketjimotswaledi100% (1)
- Patna HospitalDocument5 pagesPatna Hospitalmahwish khanNo ratings yet
- Review On Inflammatory DisesesDocument21 pagesReview On Inflammatory Disesesdigitalmazdoor5201No ratings yet
- Validation of The Adolescent Self Esteem QuestionnaireDocument34 pagesValidation of The Adolescent Self Esteem Questionnairevijayalakshmi100% (1)
- Why I Am Intersted in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The FutureDocument3 pagesWhy I Am Intersted in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The FuturehermawanNo ratings yet
- Nurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationDocument4 pagesNurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationEmma WatsonNo ratings yet
- Campbell, James - CV - 25 Feb 2016Document42 pagesCampbell, James - CV - 25 Feb 2016meenakshi.r.agrawalNo ratings yet
- Safe Work Method Statement For High Risk Construction Work (SWMS) TemplateDocument3 pagesSafe Work Method Statement For High Risk Construction Work (SWMS) TemplateMarulituaNo ratings yet
- XII A PE Project ListDocument2 pagesXII A PE Project ListShriyanshi DasNo ratings yet
- SAGDocument229 pagesSAGMalshej Goat Farm All about goatsNo ratings yet
- Antiscale (DEQUEST SPE 0001)Document7 pagesAntiscale (DEQUEST SPE 0001)mahdi rasoulianNo ratings yet
- Ethical Case StudiesDocument9 pagesEthical Case StudiesًNo ratings yet
- Standard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisDocument11 pagesStandard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisAbuNo ratings yet
- NCM 114 Care For Older Adults MODULE 5Document5 pagesNCM 114 Care For Older Adults MODULE 5Meryville JacildoNo ratings yet
- 1205WHO Vs GMP Slide 16 OnwardsDocument31 pages1205WHO Vs GMP Slide 16 OnwardsTumma RamaraoNo ratings yet
- DN4 Assessment ToolDocument1 pageDN4 Assessment ToolrahmiNo ratings yet
- AV eIFU 10223671 Mg-En V03Document68 pagesAV eIFU 10223671 Mg-En V03Goutham RevuruNo ratings yet
- New Graduate RN Cover Letter SamplesDocument7 pagesNew Graduate RN Cover Letter Samplesf60pk9dc100% (3)
- Ethics Unit 2Document22 pagesEthics Unit 2SaniNo ratings yet
- 2 Ethical Aspects of Nursing ResearchDocument35 pages2 Ethical Aspects of Nursing ResearchGrape JuiceNo ratings yet
- Psychological Testing Report-1Document80 pagesPsychological Testing Report-1Laveeza KhurramNo ratings yet
- Griffith'S Experiment: Frederick Griffith (1877-1941) Was A British Bacteriologist Whose Focus Was TheDocument16 pagesGriffith'S Experiment: Frederick Griffith (1877-1941) Was A British Bacteriologist Whose Focus Was TheKeljang MoktanNo ratings yet
- Operational Control Procedure For Noise MonitoringDocument2 pagesOperational Control Procedure For Noise MonitoringKishan MauryaNo ratings yet
- 5 Sciatica Exercises For Pain Relief (With Pictures) : Back IntelligenceDocument26 pages5 Sciatica Exercises For Pain Relief (With Pictures) : Back Intelligenceanand sahu100% (1)
- 358 Developmental DomainsDocument2 pages358 Developmental Domainsapi-285147481No ratings yet
- Hlthaff 23 4 202 PDFDocument11 pagesHlthaff 23 4 202 PDFexaNo ratings yet
- The National Bursary PolicyDocument20 pagesThe National Bursary PolicyCrazyCrafterYTNo ratings yet