
Nejmoa1702752 Appendix
Nejmoa1702752 Appendix
You might also like
- PADI Enriched Air Diver Knowledge ReviewDocument2 pagesPADI Enriched Air Diver Knowledge ReviewTracey0% (3)
- A Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)Document434 pagesA Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)AbdulraHman KhalEd100% (2)
- Atlas of Full Breast Ultrasonography - 1st PDFDocument392 pagesAtlas of Full Breast Ultrasonography - 1st PDFIosub Lica-Claudiu100% (3)
- Applied Kinesiology Collected Papers 2001-2006Document124 pagesApplied Kinesiology Collected Papers 2001-2006Huib Salomons80% (10)
- Into The Wild SummaryDocument8 pagesInto The Wild SummarydaggoooNo ratings yet
- A Rectification Manual - ExampleDocument41 pagesA Rectification Manual - Examplesorobanista100% (1)
- Cardiovascular ImagingDocument401 pagesCardiovascular ImagingRani Mulia100% (5)
- Chiropractic and Manual Therapies 1st EditionDocument240 pagesChiropractic and Manual Therapies 1st EditionRukaphuong100% (1)
- (CPG) Philippine Practice Guidelines For The Diagnosis, Staging, and Management of Lung CarcinomaDocument54 pages(CPG) Philippine Practice Guidelines For The Diagnosis, Staging, and Management of Lung CarcinomaJobelleNo ratings yet
- Guia de MielomaDocument57 pagesGuia de MielomaVerónica Gabriela Pacheco PilcoNo ratings yet
- Physiology and Pathophysiology of ItchDocument104 pagesPhysiology and Pathophysiology of ItchBladimir CentenoNo ratings yet
- CD007498Document131 pagesCD007498Nuklear AdiwenaNo ratings yet
- Ingles 4 Tesis Abayomi SorinolaDocument154 pagesIngles 4 Tesis Abayomi SorinolaThe Almighty BelugaNo ratings yet
- Cytology Versus HPV Testing For Cervical Cancer Screening in The General PopulationDocument99 pagesCytology Versus HPV Testing For Cervical Cancer Screening in The General PopulationJosé HidalgoNo ratings yet
- Sakai Et Al-2019-Cochrane Database of Systematic ReviewsDocument47 pagesSakai Et Al-2019-Cochrane Database of Systematic ReviewsNakarit SangsirinawinNo ratings yet
- Journal - Dolutegravir - Supplementary AppendixDocument119 pagesJournal - Dolutegravir - Supplementary AppendixAey ArsasuwanNo ratings yet
- Izazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMDocument221 pagesIzazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMHokusyNo ratings yet
- All UL Systems - Scientific Article - Toshiba Publications & Clinical Evidence Radiology 2016Document66 pagesAll UL Systems - Scientific Article - Toshiba Publications & Clinical Evidence Radiology 2016Арнольд ЧайкоNo ratings yet
- 5 A4 Critical Care and Hospitalist Medicine Made Ridiculously SimpleDocument390 pages5 A4 Critical Care and Hospitalist Medicine Made Ridiculously Simpleepic sound everNo ratings yet
- RPT - 87 مهم PDFDocument84 pagesRPT - 87 مهم PDFNureddin MusaNo ratings yet
- Transplant and Dialysis Handbook 2nd Edition January 2017Document125 pagesTransplant and Dialysis Handbook 2nd Edition January 2017nathanielNo ratings yet
- Dissertation DurmazDocument204 pagesDissertation DurmazsodiogoesNo ratings yet
- Handbook of Nuclear Medicine and Molecular Imaging For PhysicistsDocument375 pagesHandbook of Nuclear Medicine and Molecular Imaging For PhysicistsNovi OktaviantiNo ratings yet
- Epa Glyphosate Carcinogenic Potential ReportDocument227 pagesEpa Glyphosate Carcinogenic Potential ReportSamantha WongNo ratings yet
- Ventilation tubes - מאמרDocument48 pagesVentilation tubes - מאמרAvishay ZoarNo ratings yet
- Anthrotech ReportDocument117 pagesAnthrotech ReportHuru HaraNo ratings yet
- ProMax Dimax3 Pan User Manual v25Document134 pagesProMax Dimax3 Pan User Manual v25OpelточкаNo ratings yet
- Guidelines For The Management of Multidrug-Resistant Tuberculosis in MyanmarDocument192 pagesGuidelines For The Management of Multidrug-Resistant Tuberculosis in MyanmarAdhi PradanaNo ratings yet
- Full Download Book Sers For Point of Care and Clinical Applications PDFDocument41 pagesFull Download Book Sers For Point of Care and Clinical Applications PDFwayne.mcgee247100% (29)
- Epidemiology of Scars and Their Consequences: Burn Scars: Margriet E. Van BaarDocument1 pageEpidemiology of Scars and Their Consequences: Burn Scars: Margriet E. Van BaarKdc Ouinbilo0% (1)
- Neustein MichelleDocument120 pagesNeustein MichellesaranyarajuNo ratings yet
- Jaslan Dawid TPC1 MutantsDocument132 pagesJaslan Dawid TPC1 MutantsIndrė LapeikaitėNo ratings yet
- Book of AbstractDocument47 pagesBook of AbstractsvirkomartinkoNo ratings yet
- JnikDocument133 pagesJnikSukanthan RNo ratings yet
- Manual de Buzunar Transplant Renal (2017)Document460 pagesManual de Buzunar Transplant Renal (2017)Stefania Tacu100% (2)
- Guidelines Repro Toxicity PDFDocument143 pagesGuidelines Repro Toxicity PDFLemon DropNo ratings yet
- NASA Spinoff 2007Document5 pagesNASA Spinoff 2007ghoshsanjoy1986No ratings yet
- Crossm: Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral ToxoplasmosisDocument28 pagesCrossm: Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral Toxoplasmosisvdy nndNo ratings yet
- Case Studies Important Environmental - Risk - v1Document124 pagesCase Studies Important Environmental - Risk - v1olaya atouifeNo ratings yet
- PHD Asprusten 2022Document112 pagesPHD Asprusten 2022Mansoura CafeNo ratings yet
- 051-Anaesthesia, Pharmacology, Intensive Care and Emergency a.P.I.C.E. - 23rd Annual Meeting-AntoDocument396 pages051-Anaesthesia, Pharmacology, Intensive Care and Emergency a.P.I.C.E. - 23rd Annual Meeting-AntoDita Retno Wulandari100% (1)
- LAURENSIA DENISE U P, Prof - Dr.marsetyawan Soesatyo, M.SC, PH.D Dr. Dra. Ning Rintiswati, M.KesDocument5 pagesLAURENSIA DENISE U P, Prof - Dr.marsetyawan Soesatyo, M.SC, PH.D Dr. Dra. Ning Rintiswati, M.Kesnaili nsnNo ratings yet
- TB and Leprosy Manual 2020 2021 1Document293 pagesTB and Leprosy Manual 2020 2021 1Satrumin ShirimaNo ratings yet
- Effectiveness Sterile NeedleDocument61 pagesEffectiveness Sterile NeedleDescriminalización.orgNo ratings yet
- Modelling of Installation Effect of Driven Piles by Hypoplasticity - Dung PDFDocument109 pagesModelling of Installation Effect of Driven Piles by Hypoplasticity - Dung PDFvilaneneNo ratings yet
- Cardiovascular Imaging For Clinical Practice - Nicholls e WorthleyDocument397 pagesCardiovascular Imaging For Clinical Practice - Nicholls e WorthleyStephanie ElexiasNo ratings yet
- White Paper IONMDocument77 pagesWhite Paper IONMJiebo LuNo ratings yet
- Boehm StephanieDocument111 pagesBoehm StephaniePrima Akli SetyoNo ratings yet
- #Thesis Final v1-06082021Document47 pages#Thesis Final v1-06082021bcaNo ratings yet
- Manual PDFDocument149 pagesManual PDFCoria AndresNo ratings yet
- RP - 978 87 93102 43 9 PDFDocument68 pagesRP - 978 87 93102 43 9 PDFMartin ValdezNo ratings yet
- WHO SecretariatDocument137 pagesWHO SecretariatmauludiNo ratings yet
- RPT 246Document46 pagesRPT 246Victoria LefiqueoNo ratings yet
- Wound Management in Urgent CareDocument93 pagesWound Management in Urgent CareFahmi RizalNo ratings yet
- Current Clinical Evidence OphtDocument183 pagesCurrent Clinical Evidence OphtouranpisNo ratings yet
- ProtocolBook 2.1Document180 pagesProtocolBook 2.1Louis N HermanNo ratings yet
- Full Chapter Reviews of Physiology Biochemistry and Pharmacology Stine Helene Falsig Pedersen 2 PDFDocument63 pagesFull Chapter Reviews of Physiology Biochemistry and Pharmacology Stine Helene Falsig Pedersen 2 PDFleroy.reyes896100% (5)
- Eng - PDF JsessionidDocument68 pagesEng - PDF JsessionidHIilda V. SerranoNo ratings yet
- Surgery of Cerebellopontine Lesions: Madjid Samii Venelin GerganovDocument894 pagesSurgery of Cerebellopontine Lesions: Madjid Samii Venelin GerganovSIMON PEREZ LOPEZNo ratings yet
- Cardiothoracic Care for Children and Young People: A Multidisciplinary ApproachFrom EverandCardiothoracic Care for Children and Young People: A Multidisciplinary ApproachKerry CookNo ratings yet
- Cargo Handling and Stowage Pages 120Document21 pagesCargo Handling and Stowage Pages 120arafeeu83% (12)
- Darft Pas Xii GasalDocument11 pagesDarft Pas Xii GasalMutia ChimoetNo ratings yet
- Phillips Et Al. 2003, Journal of Ecology, Amazon Tree SpecieDocument19 pagesPhillips Et Al. 2003, Journal of Ecology, Amazon Tree SpeciegruporeddperuNo ratings yet
- Cold AgglutinationDocument4 pagesCold AgglutinationSajjad AhmadNo ratings yet
- Workshop 9 FUTURE TENSES-2Document3 pagesWorkshop 9 FUTURE TENSES-2FABIAN ANDRES VILLANUEVA SANCHEZNo ratings yet
- 11-40 - SINUMERIK Edge - Concept - AppsDocument15 pages11-40 - SINUMERIK Edge - Concept - AppsAshish PatwardhanNo ratings yet
- I) Height of Retaining Wall H: Preliminary DataDocument10 pagesI) Height of Retaining Wall H: Preliminary DataOmPrakashNo ratings yet
- Ethical Issues in Management: Individual ProjectDocument12 pagesEthical Issues in Management: Individual ProjectARVIND SINGALNo ratings yet
- Nightingale PledgeDocument26 pagesNightingale PledgeIcee SaputilNo ratings yet
- L. N .E.R.-'': and The Silver Jubilee'' TrainDocument3 pagesL. N .E.R.-'': and The Silver Jubilee'' TrainIan FlackNo ratings yet
- Rajpura Escorts - ChandigarhnightDocument2 pagesRajpura Escorts - ChandigarhnightChandigarh NightNo ratings yet
- Resensi Novel B.inggris RikaDocument5 pagesResensi Novel B.inggris RikaRizqi RahmaniaNo ratings yet
- Ex 3 SIDocument25 pagesEx 3 SIAB123No ratings yet
- Separators of Different GenerationsDocument46 pagesSeparators of Different GenerationsISLAM I. Fekry100% (8)
- B NilfiskDocument16 pagesB Nilfiskarjun0188No ratings yet
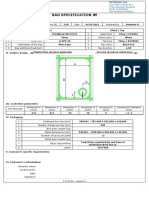
- Bag Specification 3LDocument1 pageBag Specification 3LBookWayNo ratings yet
- An Overview of Function Point AnalysisDocument6 pagesAn Overview of Function Point AnalysisavinashnNo ratings yet
- Tagmemics and Its ImplicationDocument13 pagesTagmemics and Its ImplicationtiqumNo ratings yet
- Multiple IntelligencesDocument3 pagesMultiple IntelligencesRaisa NicoldNo ratings yet
- My Happy Marriage Volume 01 LNDocument225 pagesMy Happy Marriage Volume 01 LNnailsnailsgoodinbed100% (5)
- G.O. (MS) No. 92Document10 pagesG.O. (MS) No. 92PAPD NAMAKKALNo ratings yet
- Mix 2Document4 pagesMix 2yebexa3845No ratings yet
- CBSE Class 10 English Assignment - OzymandiasDocument5 pagesCBSE Class 10 English Assignment - OzymandiasParthiva SinhaNo ratings yet
- Ziehl Neelsen Staining - Principle, Procedure and Interpretations - HowMedDocument4 pagesZiehl Neelsen Staining - Principle, Procedure and Interpretations - HowMedMeenachi ChidambaramNo ratings yet
- CHEM 580: Computational Chemistry Fall 2020 From Schrodinger To Hartree-FockDocument41 pagesCHEM 580: Computational Chemistry Fall 2020 From Schrodinger To Hartree-FockciwebNo ratings yet
- Grade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)Document2 pagesGrade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)rqb7704No ratings yet
- MBD Final Exam 2019 Model Answer PDFDocument2 pagesMBD Final Exam 2019 Model Answer PDFMina ZakariaNo ratings yet




















































































Download as pdf or txt
You might also like
- PADI Enriched Air Diver Knowledge ReviewDocument2 pagesPADI Enriched Air Diver Knowledge ReviewTracey0% (3)
- A Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)Document434 pagesA Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)AbdulraHman KhalEd100% (2)
- Atlas of Full Breast Ultrasonography - 1st PDFDocument392 pagesAtlas of Full Breast Ultrasonography - 1st PDFIosub Lica-Claudiu100% (3)
- Applied Kinesiology Collected Papers 2001-2006Document124 pagesApplied Kinesiology Collected Papers 2001-2006Huib Salomons80% (10)
- Into The Wild SummaryDocument8 pagesInto The Wild SummarydaggoooNo ratings yet
- A Rectification Manual - ExampleDocument41 pagesA Rectification Manual - Examplesorobanista100% (1)
- Cardiovascular ImagingDocument401 pagesCardiovascular ImagingRani Mulia100% (5)
- Chiropractic and Manual Therapies 1st EditionDocument240 pagesChiropractic and Manual Therapies 1st EditionRukaphuong100% (1)
- (CPG) Philippine Practice Guidelines For The Diagnosis, Staging, and Management of Lung CarcinomaDocument54 pages(CPG) Philippine Practice Guidelines For The Diagnosis, Staging, and Management of Lung CarcinomaJobelleNo ratings yet
- Guia de MielomaDocument57 pagesGuia de MielomaVerónica Gabriela Pacheco PilcoNo ratings yet
- Physiology and Pathophysiology of ItchDocument104 pagesPhysiology and Pathophysiology of ItchBladimir CentenoNo ratings yet
- CD007498Document131 pagesCD007498Nuklear AdiwenaNo ratings yet
- Ingles 4 Tesis Abayomi SorinolaDocument154 pagesIngles 4 Tesis Abayomi SorinolaThe Almighty BelugaNo ratings yet
- Cytology Versus HPV Testing For Cervical Cancer Screening in The General PopulationDocument99 pagesCytology Versus HPV Testing For Cervical Cancer Screening in The General PopulationJosé HidalgoNo ratings yet
- Sakai Et Al-2019-Cochrane Database of Systematic ReviewsDocument47 pagesSakai Et Al-2019-Cochrane Database of Systematic ReviewsNakarit SangsirinawinNo ratings yet
- Journal - Dolutegravir - Supplementary AppendixDocument119 pagesJournal - Dolutegravir - Supplementary AppendixAey ArsasuwanNo ratings yet
- Izazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMDocument221 pagesIzazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMHokusyNo ratings yet
- All UL Systems - Scientific Article - Toshiba Publications & Clinical Evidence Radiology 2016Document66 pagesAll UL Systems - Scientific Article - Toshiba Publications & Clinical Evidence Radiology 2016Арнольд ЧайкоNo ratings yet
- 5 A4 Critical Care and Hospitalist Medicine Made Ridiculously SimpleDocument390 pages5 A4 Critical Care and Hospitalist Medicine Made Ridiculously Simpleepic sound everNo ratings yet
- RPT - 87 مهم PDFDocument84 pagesRPT - 87 مهم PDFNureddin MusaNo ratings yet
- Transplant and Dialysis Handbook 2nd Edition January 2017Document125 pagesTransplant and Dialysis Handbook 2nd Edition January 2017nathanielNo ratings yet
- Dissertation DurmazDocument204 pagesDissertation DurmazsodiogoesNo ratings yet
- Handbook of Nuclear Medicine and Molecular Imaging For PhysicistsDocument375 pagesHandbook of Nuclear Medicine and Molecular Imaging For PhysicistsNovi OktaviantiNo ratings yet
- Epa Glyphosate Carcinogenic Potential ReportDocument227 pagesEpa Glyphosate Carcinogenic Potential ReportSamantha WongNo ratings yet
- Ventilation tubes - מאמרDocument48 pagesVentilation tubes - מאמרAvishay ZoarNo ratings yet
- Anthrotech ReportDocument117 pagesAnthrotech ReportHuru HaraNo ratings yet
- ProMax Dimax3 Pan User Manual v25Document134 pagesProMax Dimax3 Pan User Manual v25OpelточкаNo ratings yet
- Guidelines For The Management of Multidrug-Resistant Tuberculosis in MyanmarDocument192 pagesGuidelines For The Management of Multidrug-Resistant Tuberculosis in MyanmarAdhi PradanaNo ratings yet
- Full Download Book Sers For Point of Care and Clinical Applications PDFDocument41 pagesFull Download Book Sers For Point of Care and Clinical Applications PDFwayne.mcgee247100% (29)
- Epidemiology of Scars and Their Consequences: Burn Scars: Margriet E. Van BaarDocument1 pageEpidemiology of Scars and Their Consequences: Burn Scars: Margriet E. Van BaarKdc Ouinbilo0% (1)
- Neustein MichelleDocument120 pagesNeustein MichellesaranyarajuNo ratings yet
- Jaslan Dawid TPC1 MutantsDocument132 pagesJaslan Dawid TPC1 MutantsIndrė LapeikaitėNo ratings yet
- Book of AbstractDocument47 pagesBook of AbstractsvirkomartinkoNo ratings yet
- JnikDocument133 pagesJnikSukanthan RNo ratings yet
- Manual de Buzunar Transplant Renal (2017)Document460 pagesManual de Buzunar Transplant Renal (2017)Stefania Tacu100% (2)
- Guidelines Repro Toxicity PDFDocument143 pagesGuidelines Repro Toxicity PDFLemon DropNo ratings yet
- NASA Spinoff 2007Document5 pagesNASA Spinoff 2007ghoshsanjoy1986No ratings yet
- Crossm: Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral ToxoplasmosisDocument28 pagesCrossm: Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral Toxoplasmosisvdy nndNo ratings yet
- Case Studies Important Environmental - Risk - v1Document124 pagesCase Studies Important Environmental - Risk - v1olaya atouifeNo ratings yet
- PHD Asprusten 2022Document112 pagesPHD Asprusten 2022Mansoura CafeNo ratings yet
- 051-Anaesthesia, Pharmacology, Intensive Care and Emergency a.P.I.C.E. - 23rd Annual Meeting-AntoDocument396 pages051-Anaesthesia, Pharmacology, Intensive Care and Emergency a.P.I.C.E. - 23rd Annual Meeting-AntoDita Retno Wulandari100% (1)
- LAURENSIA DENISE U P, Prof - Dr.marsetyawan Soesatyo, M.SC, PH.D Dr. Dra. Ning Rintiswati, M.KesDocument5 pagesLAURENSIA DENISE U P, Prof - Dr.marsetyawan Soesatyo, M.SC, PH.D Dr. Dra. Ning Rintiswati, M.Kesnaili nsnNo ratings yet
- TB and Leprosy Manual 2020 2021 1Document293 pagesTB and Leprosy Manual 2020 2021 1Satrumin ShirimaNo ratings yet
- Effectiveness Sterile NeedleDocument61 pagesEffectiveness Sterile NeedleDescriminalización.orgNo ratings yet
- Modelling of Installation Effect of Driven Piles by Hypoplasticity - Dung PDFDocument109 pagesModelling of Installation Effect of Driven Piles by Hypoplasticity - Dung PDFvilaneneNo ratings yet
- Cardiovascular Imaging For Clinical Practice - Nicholls e WorthleyDocument397 pagesCardiovascular Imaging For Clinical Practice - Nicholls e WorthleyStephanie ElexiasNo ratings yet
- White Paper IONMDocument77 pagesWhite Paper IONMJiebo LuNo ratings yet
- Boehm StephanieDocument111 pagesBoehm StephaniePrima Akli SetyoNo ratings yet
- #Thesis Final v1-06082021Document47 pages#Thesis Final v1-06082021bcaNo ratings yet
- Manual PDFDocument149 pagesManual PDFCoria AndresNo ratings yet
- RP - 978 87 93102 43 9 PDFDocument68 pagesRP - 978 87 93102 43 9 PDFMartin ValdezNo ratings yet
- WHO SecretariatDocument137 pagesWHO SecretariatmauludiNo ratings yet
- RPT 246Document46 pagesRPT 246Victoria LefiqueoNo ratings yet
- Wound Management in Urgent CareDocument93 pagesWound Management in Urgent CareFahmi RizalNo ratings yet
- Current Clinical Evidence OphtDocument183 pagesCurrent Clinical Evidence OphtouranpisNo ratings yet
- ProtocolBook 2.1Document180 pagesProtocolBook 2.1Louis N HermanNo ratings yet
- Full Chapter Reviews of Physiology Biochemistry and Pharmacology Stine Helene Falsig Pedersen 2 PDFDocument63 pagesFull Chapter Reviews of Physiology Biochemistry and Pharmacology Stine Helene Falsig Pedersen 2 PDFleroy.reyes896100% (5)
- Eng - PDF JsessionidDocument68 pagesEng - PDF JsessionidHIilda V. SerranoNo ratings yet
- Surgery of Cerebellopontine Lesions: Madjid Samii Venelin GerganovDocument894 pagesSurgery of Cerebellopontine Lesions: Madjid Samii Venelin GerganovSIMON PEREZ LOPEZNo ratings yet
- Cardiothoracic Care for Children and Young People: A Multidisciplinary ApproachFrom EverandCardiothoracic Care for Children and Young People: A Multidisciplinary ApproachKerry CookNo ratings yet
- Cargo Handling and Stowage Pages 120Document21 pagesCargo Handling and Stowage Pages 120arafeeu83% (12)
- Darft Pas Xii GasalDocument11 pagesDarft Pas Xii GasalMutia ChimoetNo ratings yet
- Phillips Et Al. 2003, Journal of Ecology, Amazon Tree SpecieDocument19 pagesPhillips Et Al. 2003, Journal of Ecology, Amazon Tree SpeciegruporeddperuNo ratings yet
- Cold AgglutinationDocument4 pagesCold AgglutinationSajjad AhmadNo ratings yet
- Workshop 9 FUTURE TENSES-2Document3 pagesWorkshop 9 FUTURE TENSES-2FABIAN ANDRES VILLANUEVA SANCHEZNo ratings yet
- 11-40 - SINUMERIK Edge - Concept - AppsDocument15 pages11-40 - SINUMERIK Edge - Concept - AppsAshish PatwardhanNo ratings yet
- I) Height of Retaining Wall H: Preliminary DataDocument10 pagesI) Height of Retaining Wall H: Preliminary DataOmPrakashNo ratings yet
- Ethical Issues in Management: Individual ProjectDocument12 pagesEthical Issues in Management: Individual ProjectARVIND SINGALNo ratings yet
- Nightingale PledgeDocument26 pagesNightingale PledgeIcee SaputilNo ratings yet
- L. N .E.R.-'': and The Silver Jubilee'' TrainDocument3 pagesL. N .E.R.-'': and The Silver Jubilee'' TrainIan FlackNo ratings yet
- Rajpura Escorts - ChandigarhnightDocument2 pagesRajpura Escorts - ChandigarhnightChandigarh NightNo ratings yet
- Resensi Novel B.inggris RikaDocument5 pagesResensi Novel B.inggris RikaRizqi RahmaniaNo ratings yet
- Ex 3 SIDocument25 pagesEx 3 SIAB123No ratings yet
- Separators of Different GenerationsDocument46 pagesSeparators of Different GenerationsISLAM I. Fekry100% (8)
- B NilfiskDocument16 pagesB Nilfiskarjun0188No ratings yet
- Bag Specification 3LDocument1 pageBag Specification 3LBookWayNo ratings yet
- An Overview of Function Point AnalysisDocument6 pagesAn Overview of Function Point AnalysisavinashnNo ratings yet
- Tagmemics and Its ImplicationDocument13 pagesTagmemics and Its ImplicationtiqumNo ratings yet
- Multiple IntelligencesDocument3 pagesMultiple IntelligencesRaisa NicoldNo ratings yet
- My Happy Marriage Volume 01 LNDocument225 pagesMy Happy Marriage Volume 01 LNnailsnailsgoodinbed100% (5)
- G.O. (MS) No. 92Document10 pagesG.O. (MS) No. 92PAPD NAMAKKALNo ratings yet
- Mix 2Document4 pagesMix 2yebexa3845No ratings yet
- CBSE Class 10 English Assignment - OzymandiasDocument5 pagesCBSE Class 10 English Assignment - OzymandiasParthiva SinhaNo ratings yet
- Ziehl Neelsen Staining - Principle, Procedure and Interpretations - HowMedDocument4 pagesZiehl Neelsen Staining - Principle, Procedure and Interpretations - HowMedMeenachi ChidambaramNo ratings yet
- CHEM 580: Computational Chemistry Fall 2020 From Schrodinger To Hartree-FockDocument41 pagesCHEM 580: Computational Chemistry Fall 2020 From Schrodinger To Hartree-FockciwebNo ratings yet
- Grade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)Document2 pagesGrade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)rqb7704No ratings yet
- MBD Final Exam 2019 Model Answer PDFDocument2 pagesMBD Final Exam 2019 Model Answer PDFMina ZakariaNo ratings yet