Download as pdf or txt
You might also like
- Complete Denture ProsthodonticsDocument348 pagesComplete Denture ProsthodonticsRazvan Ungureanu67% (3)
- Iti Treatment Guide Vol2 - Loading Protocols in Implant DentistryDocument12 pagesIti Treatment Guide Vol2 - Loading Protocols in Implant DentistryS. Benzaquen0% (1)
- Dental Fees Scale in Malaysia 2014Document1 pageDental Fees Scale in Malaysia 2014Arif Azizan100% (7)
- Clinical Assessment of Short Implants Retsining Removsble Partial DenturesDocument7 pagesClinical Assessment of Short Implants Retsining Removsble Partial DenturesLouis HutahaeanNo ratings yet
- CementumDocument47 pagesCementumpratikl12345No ratings yet
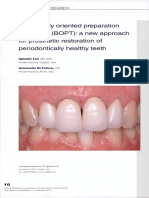
- Biologically Oriented Preparation Technique (BOPT) : A Ne/a/ Approach For Prosthetic Restoration of Periodontically Healthy TeethDocument15 pagesBiologically Oriented Preparation Technique (BOPT) : A Ne/a/ Approach For Prosthetic Restoration of Periodontically Healthy TeethDr. Marica Ramona Elena100% (2)
- Rde 39 51Document5 pagesRde 39 51Sashwat SathishNo ratings yet
- Surgical Management of A Large Periapical Lesion With PRF and Xenograft - A Case ReportDocument3 pagesSurgical Management of A Large Periapical Lesion With PRF and Xenograft - A Case ReportJohn SmithNo ratings yet
- 371-Article Text-1509-3-10-20210710Document6 pages371-Article Text-1509-3-10-20210710Fransiski HoNo ratings yet
- Surgical Management of Periapical Lesion Inmaxillary Incisorswith Combined Bone Graft and Platelet - Rich Fibrin: A Case ReportDocument5 pagesSurgical Management of Periapical Lesion Inmaxillary Incisorswith Combined Bone Graft and Platelet - Rich Fibrin: A Case ReportTMDCH JournalNo ratings yet
- NatlJMaxillofacSurg4194-4922055 134020Document6 pagesNatlJMaxillofacSurg4194-4922055 134020Zeyneb KadirNo ratings yet
- Management of The Open Apex Using New Biomaterials: 10.5005/jp-Journals-10047-0055Document5 pagesManagement of The Open Apex Using New Biomaterials: 10.5005/jp-Journals-10047-0055Asmita SonawneNo ratings yet
- The Management of Periodontitis With HypercementosDocument4 pagesThe Management of Periodontitis With HypercementosPretty HiaNo ratings yet
- Role of PeriodontistDocument5 pagesRole of PeriodontistNeetha ShenoyNo ratings yet
- 20 DR Arvind UDDocument7 pages20 DR Arvind UDJohn SmithNo ratings yet
- Regenerative Pulp Therapy For Immature Non-Vital Tooth: A Case ReportDocument4 pagesRegenerative Pulp Therapy For Immature Non-Vital Tooth: A Case ReportHansen WalaNo ratings yet
- 2022 AiutoDocument7 pages2022 AiutovivianaNo ratings yet
- PRF For ApicoectomyDocument7 pagesPRF For ApicoectomyShyambhavi SrivastavaNo ratings yet
- Apiko 3Document4 pagesApiko 3Asri DamayantiNo ratings yet
- BIODENTINEDocument5 pagesBIODENTINERiyoandaNo ratings yet
- Root Canat Tratment With RPFDocument6 pagesRoot Canat Tratment With RPFAna-Maria HriscuNo ratings yet
- CASE REPORT Esthetic Prosthodontics: Case Reports: October 2019Document5 pagesCASE REPORT Esthetic Prosthodontics: Case Reports: October 2019Thio TiganaNo ratings yet
- Combined Therapy With Mineral Trioxide ADocument5 pagesCombined Therapy With Mineral Trioxide AMihaela TuculinaNo ratings yet
- Artículo Khoury2018Document10 pagesArtículo Khoury2018Basma Derdabi100% (1)
- Apiko 4Document4 pagesApiko 4Asri DamayantiNo ratings yet
- Dentigerous CystDocument6 pagesDentigerous CystZahid ManzoorNo ratings yet
- Endo Perio2Document9 pagesEndo Perio2Fernando CordovaNo ratings yet
- A Case Report On Combination of Vista With Connective Tissue Graft As A Predictable Surgical Approach in Management of Multiple Gingival RecessionDocument5 pagesA Case Report On Combination of Vista With Connective Tissue Graft As A Predictable Surgical Approach in Management of Multiple Gingival RecessionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SaudiEndodJ113405-4168541 113445Document7 pagesSaudiEndodJ113405-4168541 113445nandaNo ratings yet
- ACMCR v13 2159Document7 pagesACMCR v13 2159Omar GadNo ratings yet
- An Innovative Technique To Restore The Non Vital Teeth With Wide Open Canals - A Clinical StudyDocument4 pagesAn Innovative Technique To Restore The Non Vital Teeth With Wide Open Canals - A Clinical StudyIOSRjournalNo ratings yet
- Jurnal Periapikal 2Document6 pagesJurnal Periapikal 2Rahmania AlikhlasNo ratings yet
- J Clinic Periodontology - 2018 - PC218 Periodontal Regeneration With The Use of Injectable Platelet Rich FibrinDocument2 pagesJ Clinic Periodontology - 2018 - PC218 Periodontal Regeneration With The Use of Injectable Platelet Rich FibrinDadi SindhuNo ratings yet
- Sept2020 ToothDocument3 pagesSept2020 ToothTrina ViskhawatNo ratings yet
- Periodontal Management of Non Healing Endodontic Lesion - A Case ReportDocument5 pagesPeriodontal Management of Non Healing Endodontic Lesion - A Case ReportbubuvulpeaNo ratings yet
- Case Report Management of Adverse Tissue Response To Faulty Pontic Design-A Case ReportDocument5 pagesCase Report Management of Adverse Tissue Response To Faulty Pontic Design-A Case ReportNajeeb UllahNo ratings yet
- EDI Journal - A Graftless Solution For Adjacent Implants in The Aesthetic Zone - Dr. Tunkiwala Et AlDocument6 pagesEDI Journal - A Graftless Solution For Adjacent Implants in The Aesthetic Zone - Dr. Tunkiwala Et AlNaina TalwarNo ratings yet
- Caso Clínico de Sausage TechniqueDocument12 pagesCaso Clínico de Sausage Techniquealessandra camposNo ratings yet
- Surgical and Endodontic Management of Large Cystic Lesion: AbstractDocument5 pagesSurgical and Endodontic Management of Large Cystic Lesion: AbstractanamaghfirohNo ratings yet
- Pre-Prosthetic Periodontal Surgery To Enhance Patient's Esthetic Need: Case SeriesDocument7 pagesPre-Prosthetic Periodontal Surgery To Enhance Patient's Esthetic Need: Case SeriesSergio Losada AmayaNo ratings yet
- Conservative Endodontic Microsurgery To Protect Critical Anatomical Structures - Selective Curettage: A Case SeriesDocument12 pagesConservative Endodontic Microsurgery To Protect Critical Anatomical Structures - Selective Curettage: A Case SeriesClaudia Pérez LuisNo ratings yet
- Platelet Rich Fibrin in Implant Dentistry in Combination With New Bone Regenerative Techique in Elderly PatientsDocument12 pagesPlatelet Rich Fibrin in Implant Dentistry in Combination With New Bone Regenerative Techique in Elderly PatientsgeraldineNo ratings yet
- Interdisciplinary Management of A Severely Compromised Periodontal Patient - Case ReportDocument10 pagesInterdisciplinary Management of A Severely Compromised Periodontal Patient - Case ReportAPinhaoFerreiraNo ratings yet
- Management of Internal Resorption: A Catch-22 Situation: Sahle AK Karanath, IB Geeta, Jayson M JamesDocument5 pagesManagement of Internal Resorption: A Catch-22 Situation: Sahle AK Karanath, IB Geeta, Jayson M JamesMelvinda ZhuoNo ratings yet
- Diagnosis and Management of Root Resorption in Traumatized TeethDocument4 pagesDiagnosis and Management of Root Resorption in Traumatized TeethDana StanciuNo ratings yet
- Ramus Onlay Bone Graft For Maxillary Alveolar Ridge Augmentation-A Case ReportDocument9 pagesRamus Onlay Bone Graft For Maxillary Alveolar Ridge Augmentation-A Case ReportIJAR JOURNALNo ratings yet
- Paper Cirugía ApicalDocument6 pagesPaper Cirugía ApicalJavier VillalobosNo ratings yet
- Egilmez 2015Document7 pagesEgilmez 2015Cecilia AhuetNo ratings yet
- A Multiple Tooth Tale: A Unique Case Report of 33 OdontomesDocument5 pagesA Multiple Tooth Tale: A Unique Case Report of 33 OdontomesIJAR JOURNALNo ratings yet
- Immediate Dentoalveolar RestorationDocument8 pagesImmediate Dentoalveolar RestorationДмитрий ЦененкоNo ratings yet
- 2022 - Platelet-Rich Fibrin - A Wonder Material For Periodontal Regeneration - A Clinical Case SeriesDocument4 pages2022 - Platelet-Rich Fibrin - A Wonder Material For Periodontal Regeneration - A Clinical Case SeriesJontavius GilbertNo ratings yet
- Recovery of Pulp Sensibility After The Surgical Management of A Large Radicular CystDocument5 pagesRecovery of Pulp Sensibility After The Surgical Management of A Large Radicular CystmeryemeNo ratings yet
- Badami 2011Document5 pagesBadami 2011ayoubNo ratings yet
- Management of Limited Interocclusal Distance With The Aid of A Modified Surgical Guide: A Clinical ReportDocument5 pagesManagement of Limited Interocclusal Distance With The Aid of A Modified Surgical Guide: A Clinical ReporttovarichNo ratings yet
- 10 1111@cid 12748Document8 pages10 1111@cid 12748Behnam TaghaviNo ratings yet
- Case PPDocument8 pagesCase PPAbhishek GuptaNo ratings yet
- Assessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportDocument4 pagesAssessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fibrina Rica en Plaquetas Autóloga - ¿Puede Asegurar Una Mejor Cicatrización?Document29 pagesFibrina Rica en Plaquetas Autóloga - ¿Puede Asegurar Una Mejor Cicatrización?Rainer MujicaNo ratings yet
- Dens Evaginatus and Type V Canal Configuration: A Case ReportDocument4 pagesDens Evaginatus and Type V Canal Configuration: A Case ReportAmee PatelNo ratings yet
- Technique For Soft Tissue Modification For Pontic Reception: A Case ReportDocument4 pagesTechnique For Soft Tissue Modification For Pontic Reception: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jced 13 E75Document6 pagesJced 13 E75Ezza RezzaNo ratings yet
- 737 Ijar-23255Document7 pages737 Ijar-23255Louis HutahaeanNo ratings yet
- Reviving Immature Permanent Teeth: A Case Report On Regenerative Endodontic Treatment As A Retreatment OptionDocument3 pagesReviving Immature Permanent Teeth: A Case Report On Regenerative Endodontic Treatment As A Retreatment OptionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Witek 2019Document7 pagesWitek 2019Alejandro FereñoNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- A Review of The Uses of Fluoride and Outcomes of - Dental Caries Control in SingaporeDocument5 pagesA Review of The Uses of Fluoride and Outcomes of - Dental Caries Control in SingaporeMichelleLeeNo ratings yet
- Executive Summary: Company OverviewDocument8 pagesExecutive Summary: Company OverviewAbhishek KumarNo ratings yet
- CementumDocument26 pagesCementumPrathik RaiNo ratings yet
- Crown 6 (Dralaa)Document6 pagesCrown 6 (Dralaa)Abdullah EmadNo ratings yet
- Irrigating Solutions in Endodontics: A Brief ReviewDocument9 pagesIrrigating Solutions in Endodontics: A Brief ReviewScienceVolksNo ratings yet
- Dental ImplantsDocument15 pagesDental ImplantsSurjith JithuNo ratings yet
- Cambra PDFDocument2 pagesCambra PDFDaniel Esteban Veas GálvezNo ratings yet
- Treatment Impaksi M1 Dengan Removable Appliance PDFDocument7 pagesTreatment Impaksi M1 Dengan Removable Appliance PDFTokubetsu VidadiNo ratings yet
- Cover Letter 6Document2 pagesCover Letter 6api-553076081No ratings yet
- The Bathroom Personal Hygiene VerbsDocument1 pageThe Bathroom Personal Hygiene Verbsmargarita100% (2)
- A Multicenter Randomized Controlled Clinical Trial Using A New Resorbable Non-Cross-Linked Collagen Membrane For Guided Bone Regeneration at Dehisced Single Implant Sites InteDocument9 pagesA Multicenter Randomized Controlled Clinical Trial Using A New Resorbable Non-Cross-Linked Collagen Membrane For Guided Bone Regeneration at Dehisced Single Implant Sites Intevanessa_werbickyNo ratings yet
- Overdenture Attachment 1Document7 pagesOverdenture Attachment 1Dr Tarak ChavadaNo ratings yet
- Autoeficacia OralDocument12 pagesAutoeficacia OralSamantha OrtizNo ratings yet
- Dental HomeDocument25 pagesDental HomeAishwarya Joshi100% (2)
- Sleep Bruxism: An Overview For Clinicians: ClinicalDocument5 pagesSleep Bruxism: An Overview For Clinicians: ClinicalCristobalVeraNo ratings yet
- Adj12077 PDF JsessionidDocument2 pagesAdj12077 PDF JsessionidhayiarNo ratings yet
- Applied Pharmacology For The Dental Hygienist 8th Edition Haveles Test BankDocument35 pagesApplied Pharmacology For The Dental Hygienist 8th Edition Haveles Test Bankatop.remiped25zad100% (30)
- Occlusal Radiography + Exposure & Technique ErrorsDocument7 pagesOcclusal Radiography + Exposure & Technique ErrorsSawsan Z. Jwaied0% (1)
- Preventive Dental MaterialDocument69 pagesPreventive Dental Materialnadia yasmin100% (1)
- MainDocument112 pagesMainShana ShirinNo ratings yet
- Comparing The Pulp/tooth Area Ratio and Dentin Thickness of Mandibular First Molars in Different Age Groups: A Cone Beam Computed Tomography StudyDocument6 pagesComparing The Pulp/tooth Area Ratio and Dentin Thickness of Mandibular First Molars in Different Age Groups: A Cone Beam Computed Tomography Studydinon25No ratings yet
- Attitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional StudyDocument9 pagesAttitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional Studyasem sardyNo ratings yet
- 1985 Australian Orthodontic Journal, MelbourneDocument19 pages1985 Australian Orthodontic Journal, MelbourneMariyamNo ratings yet
- Theracal Future of Pulp Capping ????: Original Research ArticleDocument5 pagesTheracal Future of Pulp Capping ????: Original Research Articleكاظم عبد الحسينNo ratings yet
- JPID Vol 02 Issue 03 Article06Document5 pagesJPID Vol 02 Issue 03 Article06Suma 123No ratings yet