Download as docx, pdf, or txt
You might also like
- (Pocket Notebook) Wooin Ahn, Jai Radhakrishnan - Pocket Nephrology-LWW Wolters Kluwer (2019)Document695 pages(Pocket Notebook) Wooin Ahn, Jai Radhakrishnan - Pocket Nephrology-LWW Wolters Kluwer (2019)paul0004090% (10)
- DXR Harrelson SoapDocument4 pagesDXR Harrelson SoapAlexanderWarrenNo ratings yet
- Blood Administration and Transfusion Reactions QuizDocument5 pagesBlood Administration and Transfusion Reactions Quizremooheshmat100% (1)
- Nursing Care Plan Impaired Gas ExchangeDocument1 pageNursing Care Plan Impaired Gas ExchangeKarylle PetilNo ratings yet
- Transfusion Medicine QuestionsDocument31 pagesTransfusion Medicine QuestionsJhoanie Sanggoy Tauli100% (1)
- Blood Bank Practical Panel CasesDocument23 pagesBlood Bank Practical Panel CasesMiguel Vasquez0% (1)
- Handbook of Transfusion MedicineDocument96 pagesHandbook of Transfusion MedicineJoana Bessa83% (6)
- Massive Transfusion SummaryDocument1 pageMassive Transfusion Summarypaul00040No ratings yet
- Massive Transfusion ProtocolDocument5 pagesMassive Transfusion ProtocolArlette Araceli Barbosa IbarraNo ratings yet
- RBWH Critical BleedingDocument19 pagesRBWH Critical BleedingSean WingNo ratings yet
- ZSFG Blood Bank and Transfusion Service - Laboratory Manual 2020 - Pages VersionDocument18 pagesZSFG Blood Bank and Transfusion Service - Laboratory Manual 2020 - Pages VersionmarataningutukuNo ratings yet
- Blood Bank PracticalDocument24 pagesBlood Bank Practicalmoonfire2009No ratings yet
- Blood Transfusion and Conservation During SurgeryDocument86 pagesBlood Transfusion and Conservation During SurgeryajefolakemijohnNo ratings yet
- Local Media4071061158702283415Document7 pagesLocal Media4071061158702283415Haniya KhanNo ratings yet
- Blood Transfusion PolicyDocument6 pagesBlood Transfusion PolicyTanisha SinghNo ratings yet
- Blood Transfusion Guideline PDFDocument26 pagesBlood Transfusion Guideline PDFEmhemed Amer TabibNo ratings yet
- Blood TransfusionDocument36 pagesBlood TransfusionRhenzes HaraNo ratings yet
- Transfusion Medicine QuestionsDocument32 pagesTransfusion Medicine QuestionsMahmoud RamlawiNo ratings yet
- Transfusion MCQs and SAQsDocument3 pagesTransfusion MCQs and SAQsSaima IramNo ratings yet
- Blood Transfusion: A Clinician's ReferenceDocument32 pagesBlood Transfusion: A Clinician's Referenceلوريس أبو الفتوحNo ratings yet
- RN Tip Sheets Blood TransfusionDocument66 pagesRN Tip Sheets Blood TransfusionjjNo ratings yet
- Risk Analysis of Transfusion of Cryoprecipitate Without Consideration of ABO GroupDocument6 pagesRisk Analysis of Transfusion of Cryoprecipitate Without Consideration of ABO Groupmy accountNo ratings yet
- Blood Bank 3Document20 pagesBlood Bank 3moonfire2009100% (2)
- Hematological Conditions QUESTIONSDocument9 pagesHematological Conditions QUESTIONSCJ RelleveNo ratings yet
- Overview of Blood ComponentsDocument42 pagesOverview of Blood Componentsnashwaelsayedq2020No ratings yet
- TRF 14043Document10 pagesTRF 14043Ahmad ANo ratings yet
- Blood Bank ManualDocument29 pagesBlood Bank ManualMarice Ferrufino SchmidtNo ratings yet
- Blood Transfusion InstructionsDocument17 pagesBlood Transfusion InstructionsMuthuraj KasinathanNo ratings yet
- Blood Transfusion On Dialysis Guidelines Aug 2017 PDFDocument5 pagesBlood Transfusion On Dialysis Guidelines Aug 2017 PDFYolanda IrawatiNo ratings yet
- Blood Transfusion SLPDocument10 pagesBlood Transfusion SLPLovesehun OhNo ratings yet
- Blood Transfusion Protocols in NeonatesDocument12 pagesBlood Transfusion Protocols in NeonatesSupriya M A SuppiNo ratings yet
- Laboratory Unit 2Document6 pagesLaboratory Unit 2Mushy_ayaNo ratings yet
- CMQCC - Transfusion in Obstetric HemorrhageDocument10 pagesCMQCC - Transfusion in Obstetric HemorrhageBerri RahmadhoniNo ratings yet
- 77 Nursing Diagnosis Handbook An Evidence Based Guide To PlanningDocument12 pages77 Nursing Diagnosis Handbook An Evidence Based Guide To Planningbenson wambuaNo ratings yet
- 2.8 Investigation of Transfusion ReactionDocument8 pages2.8 Investigation of Transfusion ReactionBALAJINo ratings yet
- Solution Manual For Fundamentals of Nursing 9th by PotterDocument36 pagesSolution Manual For Fundamentals of Nursing 9th by Potterforraydicky3l3zzx100% (29)
- Full Download PDF of Solution Manual For Fundamentals of Nursing, 9th by Potter All ChapterDocument42 pagesFull Download PDF of Solution Manual For Fundamentals of Nursing, 9th by Potter All Chapterkemehnavio100% (3)
- Neonatal Exchange Transfusion (Neonatal)Document8 pagesNeonatal Exchange Transfusion (Neonatal)Muhammad ShahbazNo ratings yet
- Psychologie Cours de Communication Psychologie Team Conflits PNL atDocument4 pagesPsychologie Cours de Communication Psychologie Team Conflits PNL atGilbertmichyNo ratings yet
- Aa AmericanDocument17 pagesAa AmericanJimmy LaboratoristaNo ratings yet
- 2007 JulyAug Plasma TransfusionDocument9 pages2007 JulyAug Plasma TransfusionDR.RAJESWARI SUBRAMANIYANNo ratings yet
- BloodDocument11 pagesBloodMohamad YusriNo ratings yet
- Immunohematology QuizletDocument28 pagesImmunohematology QuizletReizel GaasNo ratings yet
- Case AnalysisDocument1 pageCase AnalysisKatrina Jude ElleNo ratings yet
- BT Quiz - 1 PDFDocument2 pagesBT Quiz - 1 PDFMonica JubaneNo ratings yet
- Solution Manual For Fundamentals of Nursing 9th by PotterDocument19 pagesSolution Manual For Fundamentals of Nursing 9th by PotterEarl Thibeau100% (36)
- Pocket Guide On Red Cells 2012Document8 pagesPocket Guide On Red Cells 2012Dave OrlandoNo ratings yet
- Unit 5 Blood TransfusionDocument10 pagesUnit 5 Blood TransfusionMarianne Gonzales-HerreraNo ratings yet
- Eval ExamDocument3 pagesEval ExamDwayne WadeNo ratings yet
- Massive Transfusion - StatPearls - NCBI BookshelfDocument6 pagesMassive Transfusion - StatPearls - NCBI Bookshelfsadam sodomNo ratings yet
- Exchange Transfusion Guidelines 2019Document8 pagesExchange Transfusion Guidelines 2019Dr AhmedNo ratings yet
- Update and Utilization of Component Therapy in Blood TransfusionsDocument6 pagesUpdate and Utilization of Component Therapy in Blood TransfusionsMerhan FoudaNo ratings yet
- Blood Transfusion (3) - 123Document44 pagesBlood Transfusion (3) - 123AjeeshNo ratings yet
- Blood and Blood Products Therapy PolicyDocument3 pagesBlood and Blood Products Therapy PolicymarataningutukuNo ratings yet
- Transfusion PediatricaDocument25 pagesTransfusion PediatricaelvanNo ratings yet
- Blood TransfusionDocument52 pagesBlood TransfusionAnonymous GC8uMx375% (4)
- SOP Blood Administration EngDocument4 pagesSOP Blood Administration EngEmhemed Amer Tabib100% (2)
- Massive Blood Loss in AdultsDocument16 pagesMassive Blood Loss in AdultsPurwadi SujalmoNo ratings yet
- Quizlet BB CiullaDocument37 pagesQuizlet BB Ciullarollenas61No ratings yet
- Massive TransfusionDocument3 pagesMassive Transfusionthd3rNo ratings yet
- Blood Blood CnenonateDocument17 pagesBlood Blood CnenonateSomendra Mohan ShuklaNo ratings yet
- نقابة التمريض الفلسطينية 12Document7 pagesنقابة التمريض الفلسطينية 12Amoon Abo AlrubNo ratings yet
- Practical Transfusion Medicine for the Small Animal PractitionerFrom EverandPractical Transfusion Medicine for the Small Animal PractitionerNo ratings yet
- Gornik Et Al 2024 2024 Acc Aha Aacvpr Apma Abc Scai SVM SVN Svs Sir Vess Guideline For The Management of LowerDocument108 pagesGornik Et Al 2024 2024 Acc Aha Aacvpr Apma Abc Scai SVM SVN Svs Sir Vess Guideline For The Management of Lowerpaul00040No ratings yet
- 2023 Guideline ISHLT MCS10YearUpdateDocument222 pages2023 Guideline ISHLT MCS10YearUpdatepaul00040No ratings yet
- 1 s2.0 S0894731723006223 MainDocument52 pages1 s2.0 S0894731723006223 Mainpaul00040No ratings yet
- PIIS0894731723006235Document45 pagesPIIS0894731723006235paul00040No ratings yet
- Olfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized StudyDocument7 pagesOlfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized Studypaul00040No ratings yet
- Long-Term Results After Physiologic Repair For Congenitally Corrected Transposition of The Great ArteriesDocument7 pagesLong-Term Results After Physiologic Repair For Congenitally Corrected Transposition of The Great Arteriespaul00040No ratings yet
- Circinterventions 120 010154Document12 pagesCircinterventions 120 010154paul00040No ratings yet
- Nelson's Pediatric Antimicrobial PDFDocument331 pagesNelson's Pediatric Antimicrobial PDFMADHANKUMAR MANICKAVELNo ratings yet
- The Long-Term Outcomes of Physiologic Repair For Cctga (Congenitally Corrected Transposition of The Great Arteries)Document6 pagesThe Long-Term Outcomes of Physiologic Repair For Cctga (Congenitally Corrected Transposition of The Great Arteries)paul00040No ratings yet
- Congenital Heart Disease and Adolescence (2016, Springer International Publishing)Document235 pagesCongenital Heart Disease and Adolescence (2016, Springer International Publishing)paul00040No ratings yet
- Long-Term Outcome in Congenitally Corrected Transposition of The Great ArteriesDocument7 pagesLong-Term Outcome in Congenitally Corrected Transposition of The Great Arteriespaul00040No ratings yet
- Deepika Thacker, Jack Rychik (Auth.), Robert. E Shaddy (Eds.) - Heart Failure in Congenital Heart Disease - From Fetus To Adult (2011, Springer-Verlag London)Document187 pagesDeepika Thacker, Jack Rychik (Auth.), Robert. E Shaddy (Eds.) - Heart Failure in Congenital Heart Disease - From Fetus To Adult (2011, Springer-Verlag London)paul00040No ratings yet
- Mehta Et Al-2018-American Journal of TransplantationDocument8 pagesMehta Et Al-2018-American Journal of Transplantationpaul00040No ratings yet
- Lgner 2017Document8 pagesLgner 2017paul00040No ratings yet
- Easily Missed Radiologic InjuriesDocument61 pagesEasily Missed Radiologic Injuriespaul00040No ratings yet
- pg1-33 of Pneumothorax Case StudyDocument36 pagespg1-33 of Pneumothorax Case StudyikemasNo ratings yet
- ch19 Studyoutline Respiratory-SystemDocument16 pagesch19 Studyoutline Respiratory-SystemElvin MoletaNo ratings yet
- 1 3 1 Autopsy Report and Information On The Human Body SystemsDocument3 pages1 3 1 Autopsy Report and Information On The Human Body Systemsapi-242853684No ratings yet
- Kuliah Umum TransfusiDocument54 pagesKuliah Umum TransfusiAnton TriyadiNo ratings yet
- DMLT Hematology Old PaperDocument2 pagesDMLT Hematology Old Papermandawa786No ratings yet
- Glandular EpitheliumDocument5 pagesGlandular EpitheliumNakuru SandwichNo ratings yet
- Ch2reviews of Related LiteraturesDocument9 pagesCh2reviews of Related LiteraturesIvan BuenaviaNo ratings yet
- Gaseous Exchange QDocument4 pagesGaseous Exchange QDenisNo ratings yet
- Summary of ImmunopathologyDocument2 pagesSummary of Immunopathologyavi yadavNo ratings yet
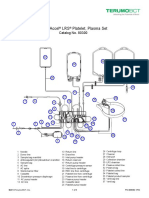
- Trima Accel LRS Platelet, Plasma Set: Catalog No. 80300Document10 pagesTrima Accel LRS Platelet, Plasma Set: Catalog No. 80300Suneo HonekawaNo ratings yet
- Digestive LPDocument7 pagesDigestive LPAlleen Joy SolivioNo ratings yet
- Sarabjit SeminarDocument290 pagesSarabjit SeminarparmeshoriNo ratings yet
- Mouse DissectionDocument6 pagesMouse DissectionMauricio F. VillamarNo ratings yet
- 11 Effects of Sleep Deprivation On Your BodyDocument1 page11 Effects of Sleep Deprivation On Your Bodydayna mooreNo ratings yet
- PMLS2 EsentialsDocument38 pagesPMLS2 EsentialsKen Novero100% (1)
- Human Body DR MellaliDocument20 pagesHuman Body DR MellaliSarah MellaliNo ratings yet
- Hematologic System Practice QuestionsDocument3 pagesHematologic System Practice QuestionsJoslyn GrossNo ratings yet
- Lesson Plan Simple FormDocument2 pagesLesson Plan Simple FormShaNe BesaresNo ratings yet
- Vocabularies: Bahasa InggrisDocument5 pagesVocabularies: Bahasa Inggrisnadia aufaNo ratings yet
- (Ofi) Respiratory SystemDocument12 pages(Ofi) Respiratory SystemPimpamNo ratings yet
- MTV1000 - PNEUMACARE (Eng) PDFDocument2 pagesMTV1000 - PNEUMACARE (Eng) PDFNhật LongNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory Systemshahirah77No ratings yet
- PPT Bedah DigestifDocument28 pagesPPT Bedah DigestifFatima Rima AndiniNo ratings yet
- Blood Basics: 1. What Makes Up The Blood in Our Bodies?Document2 pagesBlood Basics: 1. What Makes Up The Blood in Our Bodies?Jessica StewartNo ratings yet
- Facts Statistics Awareness Video Clip Related Topics Citation Discussion PrintDocument6 pagesFacts Statistics Awareness Video Clip Related Topics Citation Discussion PrintprasadNo ratings yet
- Blood Transfusion ScienceDocument23 pagesBlood Transfusion Sciencedorsa koraeiNo ratings yet
- Total WBC and RBC CountDocument18 pagesTotal WBC and RBC CountEnamul HaqueNo ratings yet
- Basic First Aid and BLS Reviewer Batch PDFDocument21 pagesBasic First Aid and BLS Reviewer Batch PDFDana Leen GonzalesNo ratings yet