
Advances in The Prevention and Management of Central Line Associated Bloodstream Infection
Advances in The Prevention and Management of Central Line Associated Bloodstream Infection
You might also like
- Cheat Sheet 1Document1 pageCheat Sheet 1Rick Frea100% (10)
- Amongst Ourselves PDFDocument252 pagesAmongst Ourselves PDFColin Khoo100% (3)
- New Insights in Dialysis Membrane BiocompatibilityDocument7 pagesNew Insights in Dialysis Membrane BiocompatibilityDani ursNo ratings yet
- Seminars in Dialysis - 2020 - Claudel - Anticoagulation in Hemodialysis A Narrative ReviewDocument14 pagesSeminars in Dialysis - 2020 - Claudel - Anticoagulation in Hemodialysis A Narrative ReviewAmanda SantosNo ratings yet
- The Role of Biological Agents in The Management of Large Vessel Vasculitis (LVV) : A Systematic Review and Meta-AnalysisDocument18 pagesThe Role of Biological Agents in The Management of Large Vessel Vasculitis (LVV) : A Systematic Review and Meta-Analysisanahh ramakNo ratings yet
- Assessment of Human Interleukin-24 Expression in Thalassemic Patients and Investigation of Current Prescription Pattern in ThalassemiaDocument11 pagesAssessment of Human Interleukin-24 Expression in Thalassemic Patients and Investigation of Current Prescription Pattern in ThalassemiaCurrents in Pharmaceutical Research (CPR)No ratings yet
- 1 s2.0 S246812451830055X MainDocument6 pages1 s2.0 S246812451830055X MainWindi LestariNo ratings yet
- Thromb2012 173124Document16 pagesThromb2012 173124Sasa SimicNo ratings yet
- Resistance To Infection of Long Term Cryopre - 2016 - The Journal of Thoracic AnDocument9 pagesResistance To Infection of Long Term Cryopre - 2016 - The Journal of Thoracic AnBintiNo ratings yet
- Design of Drug Like Hepsin Inhibitors Against Prostat - 2020 - Acta PharmaceuticDocument12 pagesDesign of Drug Like Hepsin Inhibitors Against Prostat - 2020 - Acta PharmaceuticMohammed Shuaib AhmedNo ratings yet
- 9515-Article Text-70471-1-10-20200725Document20 pages9515-Article Text-70471-1-10-20200725cristina_zaharia865440No ratings yet
- Acceso Vascular para RPTDocument10 pagesAcceso Vascular para RPTSergey ProskurinNo ratings yet
- Leukodepleted Blood Products - Deranged PhysiologyDocument4 pagesLeukodepleted Blood Products - Deranged Physiologyhnzzn2bymdNo ratings yet
- Recent Advances in The Development Of.1Document6 pagesRecent Advances in The Development Of.1Prince PatilNo ratings yet
- 15fri MamcarzResearchDocument19 pages15fri MamcarzResearchJoyce Perpetual DiasNo ratings yet
- eJHaem - 2021 - Nell - Thrombophagocytosis by Neutrophils As A Spurious Cause of ThrombocytopeniaDocument2 pageseJHaem - 2021 - Nell - Thrombophagocytosis by Neutrophils As A Spurious Cause of ThrombocytopeniaGonzalez ArturoNo ratings yet
- CREMJHIDDocument9 pagesCREMJHIDAnggy de RinconNo ratings yet
- Catéter Central y USDocument11 pagesCatéter Central y USfabio1595No ratings yet
- Tri Bler 2017Document10 pagesTri Bler 2017Thitapus DokbuaNo ratings yet
- Jurnal VaskularDocument5 pagesJurnal VaskulardrelvNo ratings yet
- D Dimer Preanalytical Analytical Postanalytical Variables and Clinical ApplicationsDocument31 pagesD Dimer Preanalytical Analytical Postanalytical Variables and Clinical ApplicationsfaizmundzirNo ratings yet
- Alloimmunization and Red Cellautoimmunization in Multitransfused Thalassemic of Indian OriginDocument5 pagesAlloimmunization and Red Cellautoimmunization in Multitransfused Thalassemic of Indian OriginFatimatuzzahra ShahabNo ratings yet
- 1 s2.0 S1109966623000210 MainDocument9 pages1 s2.0 S1109966623000210 Mainrafika triasaNo ratings yet
- 1 s2.0 S0142961220305378 MainDocument25 pages1 s2.0 S0142961220305378 MainWen-Yu SuNo ratings yet
- Periodontal Therapy Increases Neutrophil Extracellular Trap DegradationDocument10 pagesPeriodontal Therapy Increases Neutrophil Extracellular Trap DegradationElena NicuNo ratings yet
- Immunological Effects of A Single Hemodialysis TreatmentDocument14 pagesImmunological Effects of A Single Hemodialysis TreatmentBintiNo ratings yet
- A Novel Vitamin D Gene Therapy For Acute Myeloid LeukemiaDocument10 pagesA Novel Vitamin D Gene Therapy For Acute Myeloid Leukemiamelki hadisasmitaNo ratings yet
- Tangkapan Layar 2024-03-14 Pada 16.23.17Document12 pagesTangkapan Layar 2024-03-14 Pada 16.23.17Renaldo tegar Prasetyo.DNo ratings yet
- When and How To Use Direct Oral Anticoagulants in Patients With Advanced Chronic Liver Disease?Document6 pagesWhen and How To Use Direct Oral Anticoagulants in Patients With Advanced Chronic Liver Disease?Felipe SotoNo ratings yet
- 2 Dümichen2012Document6 pages2 Dümichen2012Sergio SampaioNo ratings yet
- Review: Management of Venous Port Systems in Oncology: A Review of Current EvidenceDocument7 pagesReview: Management of Venous Port Systems in Oncology: A Review of Current EvidenceLydia AmaliaNo ratings yet
- Therapeutic Plasma Exchange Protects Patients With Sepsis Associated Disseminated IntravascularDocument10 pagesTherapeutic Plasma Exchange Protects Patients With Sepsis Associated Disseminated IntravascularBhanu KumarNo ratings yet
- Uremia BleedinDocument17 pagesUremia BleedinNiswaNo ratings yet
- Nejmct1004810 2Document11 pagesNejmct1004810 2fathia1805No ratings yet
- Stenotrophomonas. Maltophilia - A Rare Cause of Bacteremia in A Patient of End Stage Renal Disease On Maintenance HemodialysisDocument3 pagesStenotrophomonas. Maltophilia - A Rare Cause of Bacteremia in A Patient of End Stage Renal Disease On Maintenance HemodialysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Clinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewDocument7 pagesClinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewIJAR JOURNALNo ratings yet
- DF Guidelines de Transfusao 2020 Advancesadv2019001143Document29 pagesDF Guidelines de Transfusao 2020 Advancesadv2019001143querominhaliberdadedevoltaNo ratings yet
- Antibiotic Lock Therapy: Review of Technique and Logistical ChallengesDocument21 pagesAntibiotic Lock Therapy: Review of Technique and Logistical ChallengesFacundo AlonsoNo ratings yet
- How I Use Platelet Transfusions - Blood 2022Document12 pagesHow I Use Platelet Transfusions - Blood 2022Jessica FloresNo ratings yet
- Mechanisms of Linezolid Resistance in Staphylococci and Enterococci Isolated From Two Teaching Hospitals in Shanghai, ChinaDocument15 pagesMechanisms of Linezolid Resistance in Staphylococci and Enterococci Isolated From Two Teaching Hospitals in Shanghai, Chinanadila oktaviaNo ratings yet
- Pediatric Hematology Oncology JournalDocument7 pagesPediatric Hematology Oncology JournalMuhammad SaeedNo ratings yet
- 1 s2.0 S2468124517300979 Main PDFDocument7 pages1 s2.0 S2468124517300979 Main PDFMuhammad SaeedNo ratings yet
- Oral Diseases - 2021 - Yang - 4sc 202 and Ink 128 Cooperate To Reverse The Epithelial To Mesenchymal Transition in OSCCDocument10 pagesOral Diseases - 2021 - Yang - 4sc 202 and Ink 128 Cooperate To Reverse The Epithelial To Mesenchymal Transition in OSCCLukas MendesNo ratings yet
- Leukemic Stem Cell Signatures IdentifyDocument16 pagesLeukemic Stem Cell Signatures Identifyniloufar rahbari100% (1)
- Longitudinal Hemodiafilter Performance in Modeled Continuous Renal Replacement TherapyDocument8 pagesLongitudinal Hemodiafilter Performance in Modeled Continuous Renal Replacement TherapyNguyễn Đức LongNo ratings yet
- Tissue Factor Positive NeutrophilsDocument35 pagesTissue Factor Positive NeutrophilsIwan kustiawanNo ratings yet
- Ascorbic Acid Vs Calcitriol in Influencing Monocyte Chemoattractant Protein-1 Nitric Oxide Superoxide Dismutase As Markers of Endothelial DysfunctiDocument7 pagesAscorbic Acid Vs Calcitriol in Influencing Monocyte Chemoattractant Protein-1 Nitric Oxide Superoxide Dismutase As Markers of Endothelial Dysfunctikuliahpagiku02No ratings yet
- Ehad 123Document12 pagesEhad 123Daiane GonçalvesNo ratings yet
- Deep Venous Thrombosis 2022. ANNALSDocument20 pagesDeep Venous Thrombosis 2022. ANNALSErnesto LainezNo ratings yet
- Red Cell Membrane Disorders: Structure Meets FunctionDocument37 pagesRed Cell Membrane Disorders: Structure Meets Functiondr.Adhonia NelsonNo ratings yet
- Thalassemia: Alan R. Cohen, Renzo Galanello, Dudley J. Pennell, Melody J. Cunningham, and Elliott VichinskyDocument21 pagesThalassemia: Alan R. Cohen, Renzo Galanello, Dudley J. Pennell, Melody J. Cunningham, and Elliott VichinskysmileyginaaNo ratings yet
- Safety and Efficacy Therapy New CombinationDocument11 pagesSafety and Efficacy Therapy New CombinationFalisha Belvia KairinNo ratings yet
- Clinical Review: Blood Purifi Cation For SepsisDocument10 pagesClinical Review: Blood Purifi Cation For SepsisVlady78No ratings yet
- AnnMaxillofacSurg11175-8428373 232443Document5 pagesAnnMaxillofacSurg11175-8428373 232443Wilson WijayaNo ratings yet
- 1 s2.0 S0925443923001850 MainDocument11 pages1 s2.0 S0925443923001850 Mainviventius yoshuaNo ratings yet
- A Comparison of Red Cell Rejuvenation Versus Mechanical Washing For The Prevention of Transfusion-Associated Organ Injury in SwineDocument11 pagesA Comparison of Red Cell Rejuvenation Versus Mechanical Washing For The Prevention of Transfusion-Associated Organ Injury in Swinealfrilia0843No ratings yet
- Blood Cell - An Overview of Studies in Hematology PDFDocument360 pagesBlood Cell - An Overview of Studies in Hematology PDFnaresh sharmaNo ratings yet
- Management of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHDocument10 pagesManagement of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHCarlos Enrique Almonte MarínNo ratings yet
- HHS Public AccessDocument16 pagesHHS Public AccessFerry HartonoNo ratings yet
- Tumor MicroenvironmentFrom EverandTumor MicroenvironmentDietmar W. SiemannNo ratings yet
- International Association of Pediatric Dentistry - Children 0-2 Years of AgeDocument14 pagesInternational Association of Pediatric Dentistry - Children 0-2 Years of AgeMafe SalazarNo ratings yet
- Questions MCQDocument16 pagesQuestions MCQBijay Kumar MahatoNo ratings yet
- Dental Students Knowledge of Ergonomic Postural Requirements and Their Application DuringDocument5 pagesDental Students Knowledge of Ergonomic Postural Requirements and Their Application DuringVinska AndriasNo ratings yet
- DLL - Science 5 - Q2 - W4Document5 pagesDLL - Science 5 - Q2 - W4angeline saldoNo ratings yet
- Abstract BookDocument168 pagesAbstract BookPawanKaushikNo ratings yet
- Skin Cancer Detection Using Digital Image Processing and Implementation Using ANN and ABCD FeaturesDocument6 pagesSkin Cancer Detection Using Digital Image Processing and Implementation Using ANN and ABCD FeaturesEditor IJTSRDNo ratings yet
- 2.blood Flow, Metabolism, Ventilation and PerfusionDocument49 pages2.blood Flow, Metabolism, Ventilation and PerfusionEbin EbenezerNo ratings yet
- Patients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaDocument18 pagesPatients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaNurul pattyNo ratings yet
- Edit Dafpus TK 1-1Document3 pagesEdit Dafpus TK 1-1annewidiatmoNo ratings yet
- Preoperative Preparation: Department Anesthesiology & Reanimation Medical Faculty Lampung UniversityDocument60 pagesPreoperative Preparation: Department Anesthesiology & Reanimation Medical Faculty Lampung UniversityDesty ArianiNo ratings yet
- Malocclusion (2nd Concept Map)Document4 pagesMalocclusion (2nd Concept Map)Stephanie Joy EscalaNo ratings yet
- Obesity ProjectDocument92 pagesObesity ProjectAjay Pal Natt100% (1)
- 239 910 1 PB PDFDocument133 pages239 910 1 PB PDFEres TriasaNo ratings yet
- 1 Childhood Nephrotic Syndrome - Diagnosis and ManagementDocument52 pages1 Childhood Nephrotic Syndrome - Diagnosis and ManagementNilupul Niwantha100% (1)
- Ineffective AIRWAY CLEARANCE RT Retained Mucus Secretions AEB The (+) Crackles On Both Lower Lung Field.Document2 pagesIneffective AIRWAY CLEARANCE RT Retained Mucus Secretions AEB The (+) Crackles On Both Lower Lung Field.Senyorita KHaye0% (1)
- Care Plan-Otitis NewDocument33 pagesCare Plan-Otitis NewSUNIL KUMARNo ratings yet
- Kekhususan Bab XI - Bab IV Sistem Digestif Dan Endokrin Dengan Kode AsteriknyaDocument3 pagesKekhususan Bab XI - Bab IV Sistem Digestif Dan Endokrin Dengan Kode Asteriknyaarachis arumawatiNo ratings yet
- Ventriculo UnicoDocument19 pagesVentriculo UnicoDavid MartínezNo ratings yet
- Bacteriophage - Structure, Replication, Uses - Microbe OnlineDocument12 pagesBacteriophage - Structure, Replication, Uses - Microbe OnlineAll in oneNo ratings yet
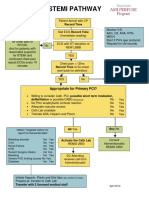
- Stemi Pathway: Record TimeDocument2 pagesStemi Pathway: Record TimeOlga Jadha CasmiraNo ratings yet
- 2017 Field Guide For Diagnosis Prevention and Control of Diseases of Shrimp and Finfish in Brackishwater AquacultureDocument40 pages2017 Field Guide For Diagnosis Prevention and Control of Diseases of Shrimp and Finfish in Brackishwater AquaculturerambabuNo ratings yet
- NCM 109 MCN Semifinals Gestational ConditionsDocument6 pagesNCM 109 MCN Semifinals Gestational ConditionsQUEZON, BRITNEY KIM E.No ratings yet
- Seminar On Rheumatic Heart Disease: by Zerihun GetachewDocument37 pagesSeminar On Rheumatic Heart Disease: by Zerihun GetachewZerihun Getachew ShiferawNo ratings yet
- Hospice and Palliative Care in IndiaDocument9 pagesHospice and Palliative Care in IndiaArunpv001No ratings yet
- AIIMS Jodhpur & RishikeshDocument30 pagesAIIMS Jodhpur & Rishikeshshubham vermaNo ratings yet
- Name: Subject: Date:: Surname 1Document3 pagesName: Subject: Date:: Surname 1mutua daveNo ratings yet
- Modified French OsteotomyDocument5 pagesModified French OsteotomyKaustubh KeskarNo ratings yet
- Complete Syllabus of Class XI & XII: Botany (Medical)Document6 pagesComplete Syllabus of Class XI & XII: Botany (Medical)Abhijeet ParkhiNo ratings yet























































































Download as pdf or txt
You might also like
- Cheat Sheet 1Document1 pageCheat Sheet 1Rick Frea100% (10)
- Amongst Ourselves PDFDocument252 pagesAmongst Ourselves PDFColin Khoo100% (3)
- New Insights in Dialysis Membrane BiocompatibilityDocument7 pagesNew Insights in Dialysis Membrane BiocompatibilityDani ursNo ratings yet
- Seminars in Dialysis - 2020 - Claudel - Anticoagulation in Hemodialysis A Narrative ReviewDocument14 pagesSeminars in Dialysis - 2020 - Claudel - Anticoagulation in Hemodialysis A Narrative ReviewAmanda SantosNo ratings yet
- The Role of Biological Agents in The Management of Large Vessel Vasculitis (LVV) : A Systematic Review and Meta-AnalysisDocument18 pagesThe Role of Biological Agents in The Management of Large Vessel Vasculitis (LVV) : A Systematic Review and Meta-Analysisanahh ramakNo ratings yet
- Assessment of Human Interleukin-24 Expression in Thalassemic Patients and Investigation of Current Prescription Pattern in ThalassemiaDocument11 pagesAssessment of Human Interleukin-24 Expression in Thalassemic Patients and Investigation of Current Prescription Pattern in ThalassemiaCurrents in Pharmaceutical Research (CPR)No ratings yet
- 1 s2.0 S246812451830055X MainDocument6 pages1 s2.0 S246812451830055X MainWindi LestariNo ratings yet
- Thromb2012 173124Document16 pagesThromb2012 173124Sasa SimicNo ratings yet
- Resistance To Infection of Long Term Cryopre - 2016 - The Journal of Thoracic AnDocument9 pagesResistance To Infection of Long Term Cryopre - 2016 - The Journal of Thoracic AnBintiNo ratings yet
- Design of Drug Like Hepsin Inhibitors Against Prostat - 2020 - Acta PharmaceuticDocument12 pagesDesign of Drug Like Hepsin Inhibitors Against Prostat - 2020 - Acta PharmaceuticMohammed Shuaib AhmedNo ratings yet
- 9515-Article Text-70471-1-10-20200725Document20 pages9515-Article Text-70471-1-10-20200725cristina_zaharia865440No ratings yet
- Acceso Vascular para RPTDocument10 pagesAcceso Vascular para RPTSergey ProskurinNo ratings yet
- Leukodepleted Blood Products - Deranged PhysiologyDocument4 pagesLeukodepleted Blood Products - Deranged Physiologyhnzzn2bymdNo ratings yet
- Recent Advances in The Development Of.1Document6 pagesRecent Advances in The Development Of.1Prince PatilNo ratings yet
- 15fri MamcarzResearchDocument19 pages15fri MamcarzResearchJoyce Perpetual DiasNo ratings yet
- eJHaem - 2021 - Nell - Thrombophagocytosis by Neutrophils As A Spurious Cause of ThrombocytopeniaDocument2 pageseJHaem - 2021 - Nell - Thrombophagocytosis by Neutrophils As A Spurious Cause of ThrombocytopeniaGonzalez ArturoNo ratings yet
- CREMJHIDDocument9 pagesCREMJHIDAnggy de RinconNo ratings yet
- Catéter Central y USDocument11 pagesCatéter Central y USfabio1595No ratings yet
- Tri Bler 2017Document10 pagesTri Bler 2017Thitapus DokbuaNo ratings yet
- Jurnal VaskularDocument5 pagesJurnal VaskulardrelvNo ratings yet
- D Dimer Preanalytical Analytical Postanalytical Variables and Clinical ApplicationsDocument31 pagesD Dimer Preanalytical Analytical Postanalytical Variables and Clinical ApplicationsfaizmundzirNo ratings yet
- Alloimmunization and Red Cellautoimmunization in Multitransfused Thalassemic of Indian OriginDocument5 pagesAlloimmunization and Red Cellautoimmunization in Multitransfused Thalassemic of Indian OriginFatimatuzzahra ShahabNo ratings yet
- 1 s2.0 S1109966623000210 MainDocument9 pages1 s2.0 S1109966623000210 Mainrafika triasaNo ratings yet
- 1 s2.0 S0142961220305378 MainDocument25 pages1 s2.0 S0142961220305378 MainWen-Yu SuNo ratings yet
- Periodontal Therapy Increases Neutrophil Extracellular Trap DegradationDocument10 pagesPeriodontal Therapy Increases Neutrophil Extracellular Trap DegradationElena NicuNo ratings yet
- Immunological Effects of A Single Hemodialysis TreatmentDocument14 pagesImmunological Effects of A Single Hemodialysis TreatmentBintiNo ratings yet
- A Novel Vitamin D Gene Therapy For Acute Myeloid LeukemiaDocument10 pagesA Novel Vitamin D Gene Therapy For Acute Myeloid Leukemiamelki hadisasmitaNo ratings yet
- Tangkapan Layar 2024-03-14 Pada 16.23.17Document12 pagesTangkapan Layar 2024-03-14 Pada 16.23.17Renaldo tegar Prasetyo.DNo ratings yet
- When and How To Use Direct Oral Anticoagulants in Patients With Advanced Chronic Liver Disease?Document6 pagesWhen and How To Use Direct Oral Anticoagulants in Patients With Advanced Chronic Liver Disease?Felipe SotoNo ratings yet
- 2 Dümichen2012Document6 pages2 Dümichen2012Sergio SampaioNo ratings yet
- Review: Management of Venous Port Systems in Oncology: A Review of Current EvidenceDocument7 pagesReview: Management of Venous Port Systems in Oncology: A Review of Current EvidenceLydia AmaliaNo ratings yet
- Therapeutic Plasma Exchange Protects Patients With Sepsis Associated Disseminated IntravascularDocument10 pagesTherapeutic Plasma Exchange Protects Patients With Sepsis Associated Disseminated IntravascularBhanu KumarNo ratings yet
- Uremia BleedinDocument17 pagesUremia BleedinNiswaNo ratings yet
- Nejmct1004810 2Document11 pagesNejmct1004810 2fathia1805No ratings yet
- Stenotrophomonas. Maltophilia - A Rare Cause of Bacteremia in A Patient of End Stage Renal Disease On Maintenance HemodialysisDocument3 pagesStenotrophomonas. Maltophilia - A Rare Cause of Bacteremia in A Patient of End Stage Renal Disease On Maintenance HemodialysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Clinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewDocument7 pagesClinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewIJAR JOURNALNo ratings yet
- DF Guidelines de Transfusao 2020 Advancesadv2019001143Document29 pagesDF Guidelines de Transfusao 2020 Advancesadv2019001143querominhaliberdadedevoltaNo ratings yet
- Antibiotic Lock Therapy: Review of Technique and Logistical ChallengesDocument21 pagesAntibiotic Lock Therapy: Review of Technique and Logistical ChallengesFacundo AlonsoNo ratings yet
- How I Use Platelet Transfusions - Blood 2022Document12 pagesHow I Use Platelet Transfusions - Blood 2022Jessica FloresNo ratings yet
- Mechanisms of Linezolid Resistance in Staphylococci and Enterococci Isolated From Two Teaching Hospitals in Shanghai, ChinaDocument15 pagesMechanisms of Linezolid Resistance in Staphylococci and Enterococci Isolated From Two Teaching Hospitals in Shanghai, Chinanadila oktaviaNo ratings yet
- Pediatric Hematology Oncology JournalDocument7 pagesPediatric Hematology Oncology JournalMuhammad SaeedNo ratings yet
- 1 s2.0 S2468124517300979 Main PDFDocument7 pages1 s2.0 S2468124517300979 Main PDFMuhammad SaeedNo ratings yet
- Oral Diseases - 2021 - Yang - 4sc 202 and Ink 128 Cooperate To Reverse The Epithelial To Mesenchymal Transition in OSCCDocument10 pagesOral Diseases - 2021 - Yang - 4sc 202 and Ink 128 Cooperate To Reverse The Epithelial To Mesenchymal Transition in OSCCLukas MendesNo ratings yet
- Leukemic Stem Cell Signatures IdentifyDocument16 pagesLeukemic Stem Cell Signatures Identifyniloufar rahbari100% (1)
- Longitudinal Hemodiafilter Performance in Modeled Continuous Renal Replacement TherapyDocument8 pagesLongitudinal Hemodiafilter Performance in Modeled Continuous Renal Replacement TherapyNguyễn Đức LongNo ratings yet
- Tissue Factor Positive NeutrophilsDocument35 pagesTissue Factor Positive NeutrophilsIwan kustiawanNo ratings yet
- Ascorbic Acid Vs Calcitriol in Influencing Monocyte Chemoattractant Protein-1 Nitric Oxide Superoxide Dismutase As Markers of Endothelial DysfunctiDocument7 pagesAscorbic Acid Vs Calcitriol in Influencing Monocyte Chemoattractant Protein-1 Nitric Oxide Superoxide Dismutase As Markers of Endothelial Dysfunctikuliahpagiku02No ratings yet
- Ehad 123Document12 pagesEhad 123Daiane GonçalvesNo ratings yet
- Deep Venous Thrombosis 2022. ANNALSDocument20 pagesDeep Venous Thrombosis 2022. ANNALSErnesto LainezNo ratings yet
- Red Cell Membrane Disorders: Structure Meets FunctionDocument37 pagesRed Cell Membrane Disorders: Structure Meets Functiondr.Adhonia NelsonNo ratings yet
- Thalassemia: Alan R. Cohen, Renzo Galanello, Dudley J. Pennell, Melody J. Cunningham, and Elliott VichinskyDocument21 pagesThalassemia: Alan R. Cohen, Renzo Galanello, Dudley J. Pennell, Melody J. Cunningham, and Elliott VichinskysmileyginaaNo ratings yet
- Safety and Efficacy Therapy New CombinationDocument11 pagesSafety and Efficacy Therapy New CombinationFalisha Belvia KairinNo ratings yet
- Clinical Review: Blood Purifi Cation For SepsisDocument10 pagesClinical Review: Blood Purifi Cation For SepsisVlady78No ratings yet
- AnnMaxillofacSurg11175-8428373 232443Document5 pagesAnnMaxillofacSurg11175-8428373 232443Wilson WijayaNo ratings yet
- 1 s2.0 S0925443923001850 MainDocument11 pages1 s2.0 S0925443923001850 Mainviventius yoshuaNo ratings yet
- A Comparison of Red Cell Rejuvenation Versus Mechanical Washing For The Prevention of Transfusion-Associated Organ Injury in SwineDocument11 pagesA Comparison of Red Cell Rejuvenation Versus Mechanical Washing For The Prevention of Transfusion-Associated Organ Injury in Swinealfrilia0843No ratings yet
- Blood Cell - An Overview of Studies in Hematology PDFDocument360 pagesBlood Cell - An Overview of Studies in Hematology PDFnaresh sharmaNo ratings yet
- Management of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHDocument10 pagesManagement of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHCarlos Enrique Almonte MarínNo ratings yet
- HHS Public AccessDocument16 pagesHHS Public AccessFerry HartonoNo ratings yet
- Tumor MicroenvironmentFrom EverandTumor MicroenvironmentDietmar W. SiemannNo ratings yet
- International Association of Pediatric Dentistry - Children 0-2 Years of AgeDocument14 pagesInternational Association of Pediatric Dentistry - Children 0-2 Years of AgeMafe SalazarNo ratings yet
- Questions MCQDocument16 pagesQuestions MCQBijay Kumar MahatoNo ratings yet
- Dental Students Knowledge of Ergonomic Postural Requirements and Their Application DuringDocument5 pagesDental Students Knowledge of Ergonomic Postural Requirements and Their Application DuringVinska AndriasNo ratings yet
- DLL - Science 5 - Q2 - W4Document5 pagesDLL - Science 5 - Q2 - W4angeline saldoNo ratings yet
- Abstract BookDocument168 pagesAbstract BookPawanKaushikNo ratings yet
- Skin Cancer Detection Using Digital Image Processing and Implementation Using ANN and ABCD FeaturesDocument6 pagesSkin Cancer Detection Using Digital Image Processing and Implementation Using ANN and ABCD FeaturesEditor IJTSRDNo ratings yet
- 2.blood Flow, Metabolism, Ventilation and PerfusionDocument49 pages2.blood Flow, Metabolism, Ventilation and PerfusionEbin EbenezerNo ratings yet
- Patients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaDocument18 pagesPatients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaNurul pattyNo ratings yet
- Edit Dafpus TK 1-1Document3 pagesEdit Dafpus TK 1-1annewidiatmoNo ratings yet
- Preoperative Preparation: Department Anesthesiology & Reanimation Medical Faculty Lampung UniversityDocument60 pagesPreoperative Preparation: Department Anesthesiology & Reanimation Medical Faculty Lampung UniversityDesty ArianiNo ratings yet
- Malocclusion (2nd Concept Map)Document4 pagesMalocclusion (2nd Concept Map)Stephanie Joy EscalaNo ratings yet
- Obesity ProjectDocument92 pagesObesity ProjectAjay Pal Natt100% (1)
- 239 910 1 PB PDFDocument133 pages239 910 1 PB PDFEres TriasaNo ratings yet
- 1 Childhood Nephrotic Syndrome - Diagnosis and ManagementDocument52 pages1 Childhood Nephrotic Syndrome - Diagnosis and ManagementNilupul Niwantha100% (1)
- Ineffective AIRWAY CLEARANCE RT Retained Mucus Secretions AEB The (+) Crackles On Both Lower Lung Field.Document2 pagesIneffective AIRWAY CLEARANCE RT Retained Mucus Secretions AEB The (+) Crackles On Both Lower Lung Field.Senyorita KHaye0% (1)
- Care Plan-Otitis NewDocument33 pagesCare Plan-Otitis NewSUNIL KUMARNo ratings yet
- Kekhususan Bab XI - Bab IV Sistem Digestif Dan Endokrin Dengan Kode AsteriknyaDocument3 pagesKekhususan Bab XI - Bab IV Sistem Digestif Dan Endokrin Dengan Kode Asteriknyaarachis arumawatiNo ratings yet
- Ventriculo UnicoDocument19 pagesVentriculo UnicoDavid MartínezNo ratings yet
- Bacteriophage - Structure, Replication, Uses - Microbe OnlineDocument12 pagesBacteriophage - Structure, Replication, Uses - Microbe OnlineAll in oneNo ratings yet
- Stemi Pathway: Record TimeDocument2 pagesStemi Pathway: Record TimeOlga Jadha CasmiraNo ratings yet
- 2017 Field Guide For Diagnosis Prevention and Control of Diseases of Shrimp and Finfish in Brackishwater AquacultureDocument40 pages2017 Field Guide For Diagnosis Prevention and Control of Diseases of Shrimp and Finfish in Brackishwater AquaculturerambabuNo ratings yet
- NCM 109 MCN Semifinals Gestational ConditionsDocument6 pagesNCM 109 MCN Semifinals Gestational ConditionsQUEZON, BRITNEY KIM E.No ratings yet
- Seminar On Rheumatic Heart Disease: by Zerihun GetachewDocument37 pagesSeminar On Rheumatic Heart Disease: by Zerihun GetachewZerihun Getachew ShiferawNo ratings yet
- Hospice and Palliative Care in IndiaDocument9 pagesHospice and Palliative Care in IndiaArunpv001No ratings yet
- AIIMS Jodhpur & RishikeshDocument30 pagesAIIMS Jodhpur & Rishikeshshubham vermaNo ratings yet
- Name: Subject: Date:: Surname 1Document3 pagesName: Subject: Date:: Surname 1mutua daveNo ratings yet
- Modified French OsteotomyDocument5 pagesModified French OsteotomyKaustubh KeskarNo ratings yet
- Complete Syllabus of Class XI & XII: Botany (Medical)Document6 pagesComplete Syllabus of Class XI & XII: Botany (Medical)Abhijeet ParkhiNo ratings yet