Download as pdf or txt
You might also like
- Iilt File 13Document23 pagesIilt File 13Rosmin AnsuNo ratings yet
- Urn Uvci 01 Ro M4q6dre9p31zge888lnv705oygk8w2#xDocument2 pagesUrn Uvci 01 Ro M4q6dre9p31zge888lnv705oygk8w2#xFlorian BodnariuNo ratings yet
- Clinical Observership Application Clinical NutritionDocument4 pagesClinical Observership Application Clinical Nutritionkhalidbushra635No ratings yet
- Reading VaccineImmunizationDocument13 pagesReading VaccineImmunizationelztly4694No ratings yet
- Pre-Registration Nursing Information For Prospective StudentsDocument4 pagesPre-Registration Nursing Information For Prospective StudentsbthangarajNo ratings yet
- Appendix 6 Undertaking - Declaration FormDocument1 pageAppendix 6 Undertaking - Declaration FormAr AsifNo ratings yet
- Copia de Copia de Copia de MILUMBE KATOWA Daily JournalDocument23 pagesCopia de Copia de Copia de MILUMBE KATOWA Daily JournalDania SheehamaNo ratings yet
- Comonly Used Spanish Patient FormsDocument40 pagesComonly Used Spanish Patient FormsCarlos VargasNo ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- Timeout PosterDocument2 pagesTimeout Posterapi-138096780100% (1)
- Memorandum: Faculty of DentistryDocument3 pagesMemorandum: Faculty of Dentistryabhinav guptaNo ratings yet
- Information Package-Nursing Practicum I STUDENTDocument36 pagesInformation Package-Nursing Practicum I STUDENTPui Pui LamNo ratings yet
- Handout 2Document4 pagesHandout 2Marius BuysNo ratings yet
- Medical Record FormDocument4 pagesMedical Record FormДария КоваленкоNo ratings yet
- DR Lim Meng Lang Manual TemplateDocument25 pagesDR Lim Meng Lang Manual TemplatedrtshNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- Occupational Safety 6Document15 pagesOccupational Safety 6Amal ElnashartyNo ratings yet
- Occupational Health QuestionnaireDocument13 pagesOccupational Health QuestionnaireMohamed HafezNo ratings yet
- Blood Borne Pathogens PolicyDocument8 pagesBlood Borne Pathogens PolicyChris KristoffersonNo ratings yet
- RACHEL TOÑADA Untitled DocumentDocument5 pagesRACHEL TOÑADA Untitled DocumentGem HimenaceNo ratings yet
- Hepatitis B GuianceDocument6 pagesHepatitis B GuiancePiran FarnoNo ratings yet
- Abaclinicaltrialofvaccine 181119065907Document34 pagesAbaclinicaltrialofvaccine 181119065907vũ đình dũngNo ratings yet
- In - Patient Service Ward 1Document12 pagesIn - Patient Service Ward 1mitchNo ratings yet
- COVID-19 (Coronavirus) Exposure Questionnaire For Health Care WorkersDocument3 pagesCOVID-19 (Coronavirus) Exposure Questionnaire For Health Care WorkersDixit SushmithaNo ratings yet
- Tuberculosis NclexDocument3 pagesTuberculosis NclexMarinill SolimanNo ratings yet
- Clinical Objectives GuidelinesDocument11 pagesClinical Objectives GuidelinesprowritttersNo ratings yet
- Admission and DischargeDocument14 pagesAdmission and DischargeDaryl Adrian Recaido100% (1)
- 01CIM 01 - Clinical Pathway Managing TB CasesDocument10 pages01CIM 01 - Clinical Pathway Managing TB Casesyin sNo ratings yet
- Protocol Hospital NurseDocument8 pagesProtocol Hospital NurseDeepak patelNo ratings yet
- Communicable Disease Nursing Clinical FocusDocument2 pagesCommunicable Disease Nursing Clinical Focusrceponelas1127No ratings yet
- NCP Patient 3 Cervical CADocument8 pagesNCP Patient 3 Cervical CAFatima LabaoNo ratings yet
- Immunization Requirement - Student Health Center - The University of UtahDocument2 pagesImmunization Requirement - Student Health Center - The University of Utahmithun916No ratings yet
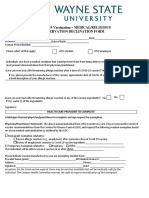
- WAYNE STATE U Covid Vaccine Declination FormDocument3 pagesWAYNE STATE U Covid Vaccine Declination FormWXYZ-TV Channel 7 DetroitNo ratings yet
- Hospital Checklist Ebola PreparednessDocument6 pagesHospital Checklist Ebola PreparednessMark ReinhardtNo ratings yet
- Post Exposure Prophylaxis: Hepatitis B, Hepatitis C and HivDocument10 pagesPost Exposure Prophylaxis: Hepatitis B, Hepatitis C and HivQaiser ZamanNo ratings yet
- 101 Essential SkillsDocument11 pages101 Essential SkillsMindy PhillipsNo ratings yet
- Quality OrientationDocument89 pagesQuality OrientationahamedsahibNo ratings yet
- MBBSInterns Log BookDocument67 pagesMBBSInterns Log Bookvibhor pathakNo ratings yet
- 491 - Mandatory Covid-19 Vaccination or Testing and Face CoveringsDocument7 pages491 - Mandatory Covid-19 Vaccination or Testing and Face CoveringsJoe BowenNo ratings yet
- Learning Module NUMBER 8 Healthcare StatisticsDocument19 pagesLearning Module NUMBER 8 Healthcare StatisticsDanyNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Student Orientation ChecklistDocument2 pagesStudent Orientation ChecklistRazor11111No ratings yet
- Inflammation ReviewerDocument17 pagesInflammation ReviewerAinee MeuvinNo ratings yet
- Observers Less Than 10 Days Do Not Receive Outlook CredentialsDocument4 pagesObservers Less Than 10 Days Do Not Receive Outlook CredentialsGeovy YépezNo ratings yet
- Notice of Conditional Acceptance For Wearing A Mask v3Document4 pagesNotice of Conditional Acceptance For Wearing A Mask v3liz knightNo ratings yet
- Policy On Employee Workplace Safety: 1.0 PurposeDocument29 pagesPolicy On Employee Workplace Safety: 1.0 PurposeSallauddin TuhinNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Annex C. Self-Assessment ToolDocument18 pagesAnnex C. Self-Assessment ToolivylantapeNo ratings yet
- A Case Study On Typhoid FeverDocument29 pagesA Case Study On Typhoid FeverGino Al Ballano Borinaga100% (2)
- Dictation Discharge Summary TemplateDocument19 pagesDictation Discharge Summary TemplateBobby ReddyNo ratings yet
- Immunization Forms - DentistryDocument5 pagesImmunization Forms - DentistryMmr LoansNo ratings yet
- FSSAI Vaccination Form - Tybar 2.5mlDocument2 pagesFSSAI Vaccination Form - Tybar 2.5mlanandsivNo ratings yet
- Req AnswersDocument4 pagesReq AnswersANDREW DEL ROSARIONo ratings yet
- Vaccination Against Covid-19: Basic InformationDocument46 pagesVaccination Against Covid-19: Basic InformationSubhashish DasNo ratings yet
- New Hire Medical Checklist 4.27.12Document6 pagesNew Hire Medical Checklist 4.27.12Mark Aaron WilsonNo ratings yet
- Immunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationDocument7 pagesImmunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationShubham TrivediNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- 1 - Appendix - A - Student Onboarding Consent FormDocument2 pages1 - Appendix - A - Student Onboarding Consent FormAshish KumarNo ratings yet
- Gena Family PlanningDocument14 pagesGena Family PlanningRuffa Jane Bangay RivasNo ratings yet
- NHA Phlebotomy Exam 2022-2023: Study Guide with 400 Practice Questions and Answers for National Healthcareer Association Certified Phlebotomy Technician ExaminationFrom EverandNHA Phlebotomy Exam 2022-2023: Study Guide with 400 Practice Questions and Answers for National Healthcareer Association Certified Phlebotomy Technician ExaminationNo ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- Urn Uvci 01 Ro Vpg0x4ykm29zerrmydn81lwo7q6er3#5Document2 pagesUrn Uvci 01 Ro Vpg0x4ykm29zerrmydn81lwo7q6er3#5Leka PeterNo ratings yet
- Non-Priority: This Is Not A Boarding CardDocument2 pagesNon-Priority: This Is Not A Boarding CardHa My PhamNo ratings yet
- ImmunisationDocument29 pagesImmunisationOjambo FlaviaNo ratings yet
- Expanded Program On ImmunizationDocument17 pagesExpanded Program On ImmunizationAmor MarzNo ratings yet
- Data Belum Vaksin Dosis 2 Kec - PadanganDocument3,330 pagesData Belum Vaksin Dosis 2 Kec - Padangansisrute padanganNo ratings yet
- CertificateDocument1 pageCertificateKavinNo ratings yet
- Classification of Psychiatric DisordersDocument64 pagesClassification of Psychiatric Disordersdrkadiyala2100% (1)
- Immunization EPI Huda 201212Document5 pagesImmunization EPI Huda 201212Aerish TupazNo ratings yet
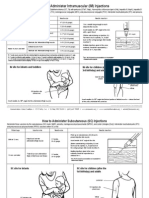
- I/M Injection Sites Acording To AgeDocument2 pagesI/M Injection Sites Acording To Ageman0billiNo ratings yet
- Overview of Immunization and EPI in Ghana StduDocument56 pagesOverview of Immunization and EPI in Ghana StduMawuliNo ratings yet
- Maternal and Neonatal Immunization Field Guide: For Latin America and The CaribbeanDocument94 pagesMaternal and Neonatal Immunization Field Guide: For Latin America and The Caribbeanmrizky ihsanNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsMuhammad AimanNo ratings yet
- How We Conquered SmallpoxDocument4 pagesHow We Conquered SmallpoxNadir BaghdadNo ratings yet
- Vas JEMDocument91 pagesVas JEMJeM LobiLabNo ratings yet
- Carteira Nacional de Vacinação DigitalDocument1 pageCarteira Nacional de Vacinação Digitalluizsergio229No ratings yet
- Promote Safe Sex and ContraceptivesDocument3 pagesPromote Safe Sex and ContraceptivesCalvin YusopNo ratings yet
- CertificateDocument1 pageCertificatechinni kumarNo ratings yet
- Complete List of Vaccines 2016Document8 pagesComplete List of Vaccines 2016Evangelist Michelle Leavy-BreunigNo ratings yet
- Travel Zoo Bangladesh LTD: 3 Star PackageDocument2 pagesTravel Zoo Bangladesh LTD: 3 Star PackageRafan HussainNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsBiraj DasNo ratings yet
- Health Teaching Plan SampleDocument4 pagesHealth Teaching Plan SampleLicha Javier100% (1)
- SC 96032864Document8 pagesSC 96032864Anonymous TESWhmTgNo ratings yet
- AsahiDocument18 pagesAsahiBkk SmkprimakesesiNo ratings yet
- PANRE and PANCE Review PsychologyDocument35 pagesPANRE and PANCE Review PsychologyThe Physician Assistant LifeNo ratings yet
- HepB Provider Tipsheet 508Document2 pagesHepB Provider Tipsheet 508Jamshaid AhmedNo ratings yet
- Immunisation and Under 5 CardDocument31 pagesImmunisation and Under 5 CardStephen AngelNo ratings yet
- Vaccines and AntiserumsDocument2 pagesVaccines and AntiserumsAbdhan DjauhariNo ratings yet
- Daftar Pustaka: Affect Disord. 2003 73 (1-2) :123-31Document2 pagesDaftar Pustaka: Affect Disord. 2003 73 (1-2) :123-31Jumria Tandi PanggaloNo ratings yet
- Differential DiagnosisDocument31 pagesDifferential DiagnosisYugi Supriatna100% (1)