Download as pdf or txt
Case Report
Vulvar Carcinoma in Pregnant Women Aged Less than 40
Years: Case Report
Malihe Hasanzadeh1, Amir Zamiri-Akhlaghi2, Maryam Hassanpoor-Moghaddam3, Soodabeh
Shahidsales4
Abstract 1. Women Health Research center,
Dept. of Gynecology Oncology,
Background: Invasive squamous cell carcinoma of the vulva is primarily a
Mashhad University of Medical
disease of postmenopausal women and thus is rarely associated with Sciences, Mashhad, Iran
pregnancy. 2. Dept. of Gynecology Oncology,
Case: We have reported on a young woman under 40 years old with vulvar Faculty of medicine, Mashhad
carcinoma, which occurred during the pregnancy but optimal treatment was University of Medical Sciences,
delayed to the postpartum period. This 37-year-old woman was diagnosed with Mashhad, Iran
3x3 cm vulvar lesion, 2 weeks after cesarean section, subsequent biopsy 3. Dept. of Gynecology Oncology,
revealed squamous cell carcinoma. She had a history of an ulcer on her left Faculty of medicine, Mashhad Azad
labia minor at the third month of the pregnancy. She was treated by a modified University of Medical Sciences,
Mashhad, Iran
radical vulvectomy and bilateral groin lymphadenectomy. She did not receive
4. Solid Tumor Treatment Research
any additional treatments. Now after two years, she has had no recurrence of Center, Mashhad University of Medical
the disease. Sciences, Mashhad, Iran
Conclusion: This case emphasizes on the need to consider malignancy as a Corresponding Author:
differential diagnosis in vulvar lesions of pregnant young women. Soodabeh Shahidsales MD;
Assistant Professor of Radiation
Keywords: Vulvar Carcinoma; Pregnancy; Squamous Cell Carcinoma Oncology
Tel: (+98) 511 8461518
Please cite this article as: Hasanzadeh M, Zamiri Akhlaghi A, Hassanpoor Email: shahidsaless@mums.ac.ir
Received: 20 Jul. 2014
Moghaddam M, Shahidsales S. Vulvar Carcinoma in Pregnant Women Aged
Accepted: 1 Sep. 2014
Less Than 40 Years: Case Report. Iran J Cancer Prev. 2014; 7(3):175-8. Iran J Cancer Prev. 2014; 3:175-8
Introduction Management is individualized [5] and with the
Invasive squamous cell carcinoma of the vulva exception of pelvic surgery, most surgical
is primarily a disease of postmenopausal women and techniques that are used in non-pregnant patients are
thus is rarely associated with pregnancy [1]. While also safe for pregnant patients [6].
squamous cell carcinomas account for about 90% of All patients whose tumors demonstrate more
all primary vulvar malignancies, most squamous than 1 mm of stromal invasion require inguino-
carcinomas of the vulva occur on the labia majora femoral lymphadenectomy. It is clear that it is not
and minora (60%) [2]. necessary to perform a bilateral groin dissection if
Keratinizing types of vulvar carcinoma, which the primary lesion is unilateral and the ipsilateral
tend to be unifocal and occur predominantly in older lymph nodes are negative [7].
patients, are not related to HPV, and often are found Independent risk factors for recurrence include
in areas adjacent to the lichen sclerosisand squamous the size of the tumor, lympho-vascular space
hyperplasia. involvement, multifocality of the tumor, status of
Physician delay is a common problem in the surgical margin, and the presence of a concurrent
diagnosis of vulvar cancer, particularly if the lesion vulvar intraepithelial neoplasia [8]. In this article we
occurs in pregnancy; therefore, any suspicious presented other cases of vulvar carcinoma in the post
vulvar lesion detected during pregnancy should be natal period.
biopsied [3]. Diagnostic delay may occur when a
low suspicion of malignancy exists in the group of Case Report
younger patient, due to the confusion about A 37-year old Iranian woman (gravid 8, live 6,
symptoms following the physiologic changes of death 2) was referred to the Department of
pregnancy or if further investigation or treatment is Gynecologic Oncology at Ghaem Hospital, in
postponed until the post-natal period [4]. November 2009. She complained about a vulvar
lesion. Two weeks before, the patient had delivered,
Vol 7, No 3, Summer 2014
175
Hasanzadeh et al.
by cesarean section, a term infant with apgar scores
of 8 and 10 at one and five minutes, respectively.
She had a history of progressive itching on her
left labia minor of the vulva for 17 years and she had
tried different therapies for her itching.
A punch biopsy was taken 2 years ago by a
dermatologist and was diagnosedas vulvar squamous
hyperplasia.
At the third month of pregnancy she noticed an
ulcer on her left labia minor. She visited different
physicians, but they prescribed typical ointments and
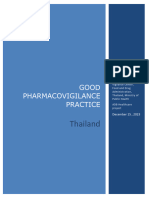
antibiotics. A physical examination revealed a 3x 3
cm lesion overlying the upper labia minor (Figure
1).
She did not have palpable bilateral inguinal
lymph nodes. After admission, she underwent a
vulvar biopsy and her pathologic report showed a
Figure 1. It shows ulcerative lesion of upper
large cell keratinizing micro-invasive squamous cell
carcinoma with an invasive depth of 3 mm (Figure labia minor.
2).
She had a normal chest X-ray and a full
sexually transmitted infection screen including HIV,
syphilis serology and hemophilusducrii cultures
were performed and were negative.
She was treated by a modified radical
vulvectomy and bilateral groin lymphadenectomy.
The size of the invasive SCC lesion was 3×3cm
with no lympho-vascularinvasion. All surgical
margins of the lesion (2cm) were free. The
pathologist reported a follicular hyperplasia in
lymph nodes. She was discharged with no additional
therapy. Two year later, she had no recurrence of the Figure 2. It shows histologic section of
disease. keratinizing micro-invasive squamous cell
carcinoma.
Discussion commonly reported [2]. In our patient, there was a
We have reported on a young woman under 40 history of pruritus for a long period.
years old with vulvar carcinoma, which occurred The patient often becomes aware of a lesion on
during the pregnancy. She was diagnosed during her vulva; but despite the superficial nature of the
pregnancy, and so optimal treatment was delayed to lesion, delays in seeking medical help are common.
the postpartum period. These findings underscore the need for patient and
Cancer of the vulva consists of 3 to 5% of all physician education with regard to the early
gynecologic malignancies [9], although it rarely diagnosis of carcinoma of the vulva and the
occurs in pregnancy [1]. importance of having a biopsy diagnosis before
Up to 2010, only 26 cases have been reported treating vulvar lesions.A biopsy of the vulva is a
as vulvar cancer during pregnancy, the latter case simple procedure that can be performed in the
was reported by Keskin [10]. Some case-reports are physician's office [3,4]. In our patient; there was a
summarized in table 1. delay in diagnosis from the first trimester of
The most common initial symptom of vulvar pregnancy to puerperium.
cancer is pruritus, which may be of a long duration. Invasive squamous cell carcinoma of the vulva
Vulvar pain, discharge, and bleeding are less involves the labia majora in about two thirds of
Iranian Journal of Cancer Prevention
176
Vulvar Carcinoma in Pregnant Women Aged Less …
Table1. Some of vulvar carcinoma case-reports in pregnancy
Title Publisher Case
Invasive squamous Eur J GynaecolOncol. 2008;29(4):399-401 In this article vulvar carcinoma was diagnosed in
carcinoma of the vulva three women less than 40 years old one which was
in women aged less than diagnosed in the third trimester of pregnancy. In the
40 years: report of two third patient was diagnosed during the last trimester
cases and a third case of pregnancy and she was treated by radical surgery
diagnosed during and postoperative radiotherapy, she had a recurrence
pregnancy in the inguinal at 36 months, and died of disease 12
months later
Invasive Vulvar Cancer Journal of Lower Genital Tract Disease: 2009 The literature available to date is limited to 26 case
in Pregnancy: Case V13(4) pp 264-268 reports.
Report and Current
Literature Review
vulvar carcinoma in
pregnancy :A CASE Medical Journal of the Islamic Republic of Iran A 28-year-old Afghan woman during pregnancy
REPORT ISSN:1016 -1430 Vol 19, Num. 2,2005, pp. presented with a vulvar squamous cell carcinoma.
185-187 The patient was treated with local excision then a
cesarean section in her 36th week of pregnancy. She
underwent modified radical vulvectomy with
bilateral inguinal lymphadenectomyfour weeks after
cesarean. Because of positive groin lymph node, she
also underwent radiation therapy. She is alive
without invasive cancer 7 months after diagnosis.
Case Report http://dx.doi.org/10.1016/j.ygyno.2004.07.018, A 36-year-old woman presented with a tender mass
Recurrent vulvar How to Cite or Link Using DOI Cited by in anterior to the left labium major, that biopsy
carcinoma in pregnancy Scopus (7) revealed to be invasive squamous cell carcinoma. In
the 23rd week of the pregnancy, she underwent a
modified radical vulvectomy and bilateral
inguinofemoral lymphadenectomy. Eleven weeks
later, she had severe vulvar intraepithelial neoplasia
(VIN III) with a small focus of invasive squamous
cell carcinoma. A radical local excision was
performed at 9 weeks postpartum.
Pregnancy-associated J Reprod Med, 45 (2000), pp. 659–661 The pregnant woman, HIV negative, presented with
invasive squamous cell vulvar pain. She had delivered a term infant three
carcinoma of the vulva months earlier at another institution and was
in a 28-year-old, HIV- diagnosed with squamous cell carcinoma of the
negative woman. A case vulva at that time but treated with delay. The patient
report underwent examination under anesthesia with
bilateral inguinal lymph node dissection, cone
biopsy, radical vulvectomy and excision of perianal
lesions.
Squamous cell Gynecol Oncol, 41 (1991), pp. 74–77 Two women presented with Vulvar carcinoma
carcinoma of the vulva during pregnancy are reported. The first patient was
inpregnancy treated by radical vulvectomy 2 weeks after
cesarean; the second case despite underwent radical
vulvectomy, died of disseminated cancer and
postoperative radiation therapy. Only 12 cases of
invasive squamous cell vulvar cancer during
pregnancy have been previously reported.
patients [2]. Location of the lesion in our patient was Vulvar SCC in young women may occur in
in the labia minor. association with or without predisposing factors that
Vol 7, No 3, Summer 2014
177
Hasanzadeh et al.
include age [11], cigarette smoking and venereal Authors’ Contribution
diseases, while chronic dermatitis is a risk factor for Maliheh Hasanzadeh wrote the case report. Zamiri
vulvar cancer [12]. Akhlaghi and Hassanpoor Moghaddam contributed
Keratinizing types of vulvar carcinoma tend to to the literature review, discussion and patient
be unifocal, and are not related to HPV, and often follow up. Soodabeh shahidsales contributed to
are found in areas adjacent to lichen sclerosis and write and final edit of the paper.
squamous hyperplasia. Our patient had a history of
chronic dermatitis for 17 years and she had a biopsy
two years ago that revealed concordant squamous References
1. Palmer JE, Tidy JA. Pregnancy following vulvar
hyperplasia.
squamous cell carcinoma: a report of two cases. J
Because no series of a meaningful size has been Gynecol Oncol. 2009; 20(4):254-6.
reported, management is individualized [5] 2. Rock JA, Thompson JD. Te lende’s Operative
according to the clinical stage and depth of invasion. Gynecology. 10th ed. Philadelphia: Lippincott-Raven;
Our patient received standard surgical treatment and 2008.
she did not require any postoperative treatment 3. Ghaemmaghami F, Hasanzadeh M. Good fetal
because she did not have any risk factors for outcome of pregnancies with gynecologic cancer
recurrence, for example no lympho-vascular conditions: cases and literature review. Int J Gynecol
invasion, unifocality of the tumor, free surgical Cancer. 2006; 16( Suppl 1):225-30
margin, and no presence of concurrent vulvar 4. Palmer JE, Vatish M, Tidy J. Squamous Cell
Vulvar Carcinoma and Pregnancy– A Review.
intraepithelial neoplasia.
European Oncology. 2010; 6(2):47–52
Moreover, the single most important prognostic 5. Ogunleye D, Lewin SN, Huettner P, Herzog TJ.
factor is lymph node status. This patient did not have Recurrent vulvar carcinoma in pregnancy. Gynecol
any lymph node involvement; therefore, she did not Oncol. 2004; 95(2):400-1.
receive any additional treatments after the surgery. 6. Amant F, Van Calsteren K, Vergote I,
Ottevanger N. Gynecologic oncology in pregnancy. Crit
Conclusion Rev Oncol Hematol. 2008; 67(3):187-95.
7. Berek JS. Novaks Gynecology. 14th ed.
A careful inspection of the vulva should be a
Lippincott Williams and Wilkins, 2007.
part of every gynecologic examination in pregnancy. 8. Preti M, Ronco G, Ghiringhello B, Micheletti L.
This case emphasizes on the need to consider Recurrent squamous cell carcinoma of the vulva:
malignancy as a differential diagnosis in vulvar clinicopathologic determinants identifying low risk
lesions of young women. We must consider biopsies patients. Cancer. 2000; 88(8):1869-76.
for all suspicious vulvar lesions, even in young and 9. 9- Sturgeon SR, Brinton LA, Devesa SS,
pregnant women. Early and thorough diagnosis with KurmanR J. In situ and invasive vulvar cancer incidence
subsequent appropriate definitive treatment cannot trends (1973 to 1987). Am J Obstet Gynecol. 1992 May;
be overemphasized. 166(5):1482-5.
10. Keskin N, Iyibozkurt AC, Topuz S, Saliholu Y,
Bengisu E, Berkman S. Invasive squamous carcinoma
Acknowledgment of the vulva in women aged less than 40 years: report of
The authors would like to thank Mrs. two cases and a third case diagnosed during pregnancy.
Moshtaghi who edited this paper. Eur J GynaecolOncol. 2008; 29(4):399-401.
11. Bakour SH, Jaleel H, Weaver JB, Kehoe S,
Radcliffe KW. Vulvar carcinoma presenting during
Conflict of Interest pregnancy, associated with recurrent bone marrow
The authors have no Conflict of interest in this hypoplasia: a case report and literature review. Gynecol
article. Oncol. 2002 Nov; 87(2):207-9.
12. Ciszko B, Pochwałowski M, St Gabryś M. Risk
factors and clinical characteristic patients with vulvar
cancer. Ginekol Pol. 2006; 77(12):914-21.
Iranian Journal of Cancer Prevention
178
You might also like
- Iggy Med Surg Test Bank Chapter 005Document19 pagesIggy Med Surg Test Bank Chapter 005Tracy Bartell80% (10)
- Reproductive Tract MalignanciesDocument30 pagesReproductive Tract Malignanciesjeelani saima100% (3)
- Nov 2017 Infantile Spasms WebinarDocument22 pagesNov 2017 Infantile Spasms WebinartetiNo ratings yet
- UntitledDocument12 pagesUntitledapi-241264935100% (1)
- Types of Medication OrdersDocument2 pagesTypes of Medication OrdersAndrei Caraiman67% (3)
- Embryonal Rhabdomyosarcoma of The Uterine Cervix: Two Cases Report and Literature ReviewDocument7 pagesEmbryonal Rhabdomyosarcoma of The Uterine Cervix: Two Cases Report and Literature ReviewPhn StanleyNo ratings yet
- OBGYN Invasive Cervical Cancer ArticleDocument7 pagesOBGYN Invasive Cervical Cancer ArticleVanessa HermioneNo ratings yet
- Uterine Carcinosarcoma A Rare and Challenging CancerDocument3 pagesUterine Carcinosarcoma A Rare and Challenging CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intl J Gynecology Obste - 2021 - Adams - Cancer of The Vagina 2021 Update 2Document9 pagesIntl J Gynecology Obste - 2021 - Adams - Cancer of The Vagina 2021 Update 2mintunlananobgynNo ratings yet
- Intl J Gynecology Obste - 2021 - AdamsDocument9 pagesIntl J Gynecology Obste - 2021 - AdamsKalaivathanan VathananNo ratings yet
- Vulvar Squamous Cell Carcinoma Revealed by PruritusDocument5 pagesVulvar Squamous Cell Carcinoma Revealed by PruritusIJAR JOURNALNo ratings yet
- Journal On CancerDocument5 pagesJournal On CancerChriz LechNo ratings yet
- Intl J Gynecology Obste - 2018 - Adams - Cancer of The VaginaDocument8 pagesIntl J Gynecology Obste - 2018 - Adams - Cancer of The VaginaBattleAppleNo ratings yet
- ONCOLOGICAL GYNECOLOGY - Malignant Tumors of The Vagina and Modalities of TreatmentDocument9 pagesONCOLOGICAL GYNECOLOGY - Malignant Tumors of The Vagina and Modalities of TreatmentVesna AntovskaNo ratings yet
- Of Endometrial CancerDocument6 pagesOf Endometrial CancerNashat SaadiNo ratings yet
- Cancer de Vulva Revision 2021Document12 pagesCancer de Vulva Revision 2021torresgaliciajesusNo ratings yet
- 2 - Cancer of The Vagina 2021 UpdateDocument9 pages2 - Cancer of The Vagina 2021 UpdateMarcell InfanteNo ratings yet
- Mucinous TumorsDocument9 pagesMucinous TumorsBadiu ElenaNo ratings yet
- Group Health EducationDocument20 pagesGroup Health EducationBrijesh Yadav100% (1)
- An Are PortDocument18 pagesAn Are PortKirsten NVNo ratings yet
- en Dome Trial CarcinomaDocument31 pagesen Dome Trial Carcinomadr_asalehNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerDebabrata SatapathyNo ratings yet
- Malignant Disease of The Vulva and VaginaDocument28 pagesMalignant Disease of The Vulva and Vaginahacker ammerNo ratings yet
- Cancer of The Vulva: 2021 Update: Alexander B. Olawaiye - Mauricio A. Cuello - Linda J. RogersDocument12 pagesCancer of The Vulva: 2021 Update: Alexander B. Olawaiye - Mauricio A. Cuello - Linda J. Rogersrg2fpgqnc8No ratings yet
- Lesson Plan On Cervical Cancer Vaccines: Mini ProjectDocument11 pagesLesson Plan On Cervical Cancer Vaccines: Mini ProjectGargi MPNo ratings yet
- Summary of Data: Cervical Cancer and ScreeningDocument10 pagesSummary of Data: Cervical Cancer and Screeningpalomazul007No ratings yet
- FIGO 2018 - Cervical CADocument15 pagesFIGO 2018 - Cervical CAJP RecioNo ratings yet
- Endometrial CancerDocument34 pagesEndometrial Canceryadnyeshpatil02No ratings yet
- Figo 2012 VaginaDocument3 pagesFigo 2012 VaginaEunike_oisNo ratings yet
- Intl J Gynecology Obste - 2021 - OlawaiyeDocument12 pagesIntl J Gynecology Obste - 2021 - OlawaiyeKalaivathanan VathananNo ratings yet
- Vulval Cancer GuidelineDocument9 pagesVulval Cancer GuidelineayubahriNo ratings yet
- Figo 2018Document15 pagesFigo 2018EJ CMNo ratings yet
- Tumor PayudaraDocument53 pagesTumor PayudaraBeivyNo ratings yet
- Clitoral Carcinoma in 30 Yr Lady: A Case ReportDocument3 pagesClitoral Carcinoma in 30 Yr Lady: A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- G. Yagci, S. Cetiner, M. Dede, O. GunhanDocument3 pagesG. Yagci, S. Cetiner, M. Dede, O. GunhanAnonymous pNIzA5No ratings yet
- Reviewon Cervical CancerDocument7 pagesReviewon Cervical CancerAlmas TNo ratings yet
- Cervical Cancer - A Global Health CrisisDocument9 pagesCervical Cancer - A Global Health Crisispb.nakulaNo ratings yet
- Uterine Body Carcinoma - DRJDocument35 pagesUterine Body Carcinoma - DRJJyoti MishraNo ratings yet
- Cervical CancerDocument28 pagesCervical CancerAmlan jyoti thanapatiNo ratings yet
- Primary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportDocument4 pagesPrimary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportBastiaanNo ratings yet
- En Dome Trial CancerDocument2 pagesEn Dome Trial CancerJaymeeNo ratings yet
- 4491 FullDocument4 pages4491 FullindojagoNo ratings yet
- Gynaecological CancersDocument4 pagesGynaecological CancerssdfNo ratings yet
- Matsuo 等。 - 2017 - Risk of metachronous ovarian cancer after ovarian 的副本Document18 pagesMatsuo 等。 - 2017 - Risk of metachronous ovarian cancer after ovarian 的副本Jing WangNo ratings yet
- Management of Borderline Ovarian Tumors - RCOGDocument6 pagesManagement of Borderline Ovarian Tumors - RCOGYossi Agung AriosenoNo ratings yet
- Primary Ovarian Malignant Mixed Mullerian Tumour: A Case ReportDocument7 pagesPrimary Ovarian Malignant Mixed Mullerian Tumour: A Case ReportIJAR JOURNALNo ratings yet
- Medical SchoolDocument39 pagesMedical SchoolHart ElettNo ratings yet
- Pathologic Types: o o o oDocument2 pagesPathologic Types: o o o orexzordNo ratings yet
- Breast Carcinoma in Axillary Tail of Spence: A Rare Case ReportDocument4 pagesBreast Carcinoma in Axillary Tail of Spence: A Rare Case Reportrajesh domakuntiNo ratings yet
- Research Article Ant Colony Optimization-Enabled CNN Deep Learning Technique For Accurate Detection of Cervical CancerDocument9 pagesResearch Article Ant Colony Optimization-Enabled CNN Deep Learning Technique For Accurate Detection of Cervical CancerFilip PajićNo ratings yet
- Kondiloma AkuminataDocument4 pagesKondiloma AkuminataIntan PermataNo ratings yet
- Naspub Ca VulvaDocument8 pagesNaspub Ca VulvaLisa Raihan LutfiaNo ratings yet
- 37-06 Hussein M. OdeibatDocument5 pages37-06 Hussein M. OdeibatgilnifNo ratings yet
- Didelphys Uterus With Cervical Cancer What About Herlyn-Werner-Wunderlich Syndrome A Case Report and Review of Literature!Document3 pagesDidelphys Uterus With Cervical Cancer What About Herlyn-Werner-Wunderlich Syndrome A Case Report and Review of Literature!International Journal of Innovative Science and Research TechnologyNo ratings yet
- Cervical CancerDocument7 pagesCervical CancerChristine Joy Clemente BerjaNo ratings yet
- Carcinoma EndometriumDocument45 pagesCarcinoma EndometriumSapna SNo ratings yet
- Female CancersDocument7 pagesFemale CancersRaymund IdicaNo ratings yet
- Rare Case of Radiotherapy Induced Angiosarcoma RIAS A - 2024 - International JDocument4 pagesRare Case of Radiotherapy Induced Angiosarcoma RIAS A - 2024 - International JRonald QuezadaNo ratings yet
- CAembarazoDocument6 pagesCAembarazoMary VeraNo ratings yet
- Uterine Sarcomas: Nomonde Mbatani - Alexander B. Olawaiye - Jaime PratDocument8 pagesUterine Sarcomas: Nomonde Mbatani - Alexander B. Olawaiye - Jaime PratMarco Julcamoro AsencioNo ratings yet
- Yufi NakalDocument13 pagesYufi NakalPantas Saroha SiburianNo ratings yet
- VV CancersDocument38 pagesVV CancersAzadovNo ratings yet
- Diagnosis and Treatment of Cervical Cancer in Pregnant WomenDocument6 pagesDiagnosis and Treatment of Cervical Cancer in Pregnant WomenSofi PiñaNo ratings yet
- Breast Disease: Diagnosis and Pathology, Volume 1From EverandBreast Disease: Diagnosis and Pathology, Volume 1Adnan AydinerNo ratings yet
- KMU CHN-LLL Final 2022Document20 pagesKMU CHN-LLL Final 2022AamirNo ratings yet
- Introduction - Case PresentationDocument16 pagesIntroduction - Case PresentationcherylNo ratings yet
- CMR ArtifactDocument51 pagesCMR ArtifactAdel SALLAMNo ratings yet
- Acumed ClavicleDocument6 pagesAcumed Claviclesiddig7No ratings yet
- Coduri DiagnosticDocument19 pagesCoduri Diagnosticivascuroxana294100% (1)
- Thailand: Good Pharmacovigilance PracticeDocument111 pagesThailand: Good Pharmacovigilance Practicepare.jittmunNo ratings yet
- Compilation of Formula: Clinical ChemistryDocument4 pagesCompilation of Formula: Clinical ChemistryJillan MarieNo ratings yet
- Esophageal Web FinalDocument1 pageEsophageal Web FinaladilNo ratings yet
- Systemic and Local Applications of Steroids in Endodontics: An Update ReviewDocument8 pagesSystemic and Local Applications of Steroids in Endodontics: An Update ReviewJorge OrbeNo ratings yet
- A Case of Atypical Course of Femoral HerniaDocument2 pagesA Case of Atypical Course of Femoral HerniaKamal GpNo ratings yet
- Ch.1 Hospital Organization and FunctionDocument25 pagesCh.1 Hospital Organization and Functionbeverly abanNo ratings yet
- Fecal Calprotectin in IBDDocument34 pagesFecal Calprotectin in IBDNathania Nadia Budiman100% (1)
- Nasopharyngeal AngiofibromaDocument15 pagesNasopharyngeal AngiofibromaSiddiqur Rahman AkashNo ratings yet
- CAE Healthcare: Your Worldwide Training Partner of ChoiceDocument39 pagesCAE Healthcare: Your Worldwide Training Partner of Choicejfrías_2No ratings yet
- S59 - LPL - Tilak Nagar 4B/13, Near Metro Pillar No.494, Tilak N AGAR, NEW DELHI - 110018 DelhiDocument4 pagesS59 - LPL - Tilak Nagar 4B/13, Near Metro Pillar No.494, Tilak N AGAR, NEW DELHI - 110018 DelhiAyushNo ratings yet
- Clinical Trials in Korea - Why KoreaDocument9 pagesClinical Trials in Korea - Why KoreaTony LowNo ratings yet
- Fokus Portable ImmunoDocument2 pagesFokus Portable Immunodanang setiawanNo ratings yet
- Real Feasibility Fasmo Skin Protectant - BalocaDocument6 pagesReal Feasibility Fasmo Skin Protectant - BalocaVincent Jay BalocaNo ratings yet
- Day 4 L2Document90 pagesDay 4 L2yousif.05001467No ratings yet
- Pedendo Proceedings Book Foutput Ok 2019 Permasalahan Dalam Skrining Hipotiroid Kongenital DiDocument186 pagesPedendo Proceedings Book Foutput Ok 2019 Permasalahan Dalam Skrining Hipotiroid Kongenital DiDamar Prasetya, Sp.ANo ratings yet
- Week 13 Documentation Related To Client CareDocument87 pagesWeek 13 Documentation Related To Client Care8rvgjxf92kNo ratings yet
- Regenerative Medicine, An Issue of Physical MedicineBook (The Clinics - Orthopedics) - Santos F. MartinezDocument646 pagesRegenerative Medicine, An Issue of Physical MedicineBook (The Clinics - Orthopedics) - Santos F. MartinezChung Tze YangNo ratings yet
- LungSEEK - 3D Selective Kernel Residual Network For Pulmonary Nodule DiagnosisDocument14 pagesLungSEEK - 3D Selective Kernel Residual Network For Pulmonary Nodule DiagnosisRonald BbosaNo ratings yet
- Drug StudyDocument14 pagesDrug StudyJho Ocampo NungayNo ratings yet
- Y Bocs Information SampleDocument2 pagesY Bocs Information SampledevNo ratings yet
- Nelec2 Week 8Document8 pagesNelec2 Week 8Michelle MallareNo ratings yet