Download as pdf or txt
You might also like
- Life Sciences Grade 10 Revision Material Term 2 - 2023Document28 pagesLife Sciences Grade 10 Revision Material Term 2 - 2023Linati Dawedi100% (1)
- Ricketts 1968Document18 pagesRicketts 1968Claudia Gamboa FerrerNo ratings yet
- Open Bite MalocclusionDocument71 pagesOpen Bite MalocclusionMohsen Saeed Ozaibi100% (2)
- 11-Lip Morphology A Factor Leading To BimaxillaryDocument7 pages11-Lip Morphology A Factor Leading To BimaxillaryJunaid Israr - OrthodonticsNo ratings yet
- Primary Correction of The Unilateral Cleft Lip Nasal Deformity: Achieving The ExcellenceDocument6 pagesPrimary Correction of The Unilateral Cleft Lip Nasal Deformity: Achieving The ExcellenceDesrainy InhardiniNo ratings yet
- Burstone PDFDocument23 pagesBurstone PDFJulio Ugás ZapataNo ratings yet
- Lip Posture and Its Signi Ficance Treatment Plannin G: Indiamapoli., IndDocument20 pagesLip Posture and Its Signi Ficance Treatment Plannin G: Indiamapoli., IndYeraldin EspañaNo ratings yet
- Lec 3 Intra Oral ExaminationDocument6 pagesLec 3 Intra Oral ExaminationMohammed JaberNo ratings yet
- 2015 Cleft Lip and Palate An Evidence-Based ReviewDocument16 pages2015 Cleft Lip and Palate An Evidence-Based ReviewDimitris RodriguezNo ratings yet
- Clinicalevaluationand Anatomicvariationofthe Oralcavity: Sunday O. Akintoye,, Mel MupparapuDocument13 pagesClinicalevaluationand Anatomicvariationofthe Oralcavity: Sunday O. Akintoye,, Mel Mupparapudira firliandaNo ratings yet
- Biomechanics of Open Bite TreatmentDocument40 pagesBiomechanics of Open Bite TreatmentMaitreye PriyadarshiniNo ratings yet
- Orthodontics 1. Clinical ExaminationDocument8 pagesOrthodontics 1. Clinical Examinationmonica896No ratings yet
- Cleft Lip and Palate An Evidence Based Review PDFDocument16 pagesCleft Lip and Palate An Evidence Based Review PDFariskaNo ratings yet
- Cleft Lip and PalateDocument5 pagesCleft Lip and Palatemremini413No ratings yet
- Queilo ComplementarDocument12 pagesQueilo ComplementarRoger Zambrana FloresNo ratings yet
- Goudy .Cleft RhinoplastyDocument20 pagesGoudy .Cleft RhinoplastyRamyar SalimiNo ratings yet
- Class II MalocclusionDocument192 pagesClass II Malocclusionyounisismail935No ratings yet
- Lip Reconstruction: Learning ObjectivesDocument8 pagesLip Reconstruction: Learning Objectivesalinutza_childNo ratings yet
- The Significance of Anatomic Landmarks in Complete Denture ServiceDocument4 pagesThe Significance of Anatomic Landmarks in Complete Denture ServiceJoshua ValdezNo ratings yet
- KH17 240404 090122Document11 pagesKH17 240404 090122Mai ThúyNo ratings yet
- CheiloplastywenaDocument30 pagesCheiloplastywenaRowena AbanteNo ratings yet
- Article Anterior Open BiteDocument6 pagesArticle Anterior Open BiteDrRudra Chakraborty100% (1)
- Oral Conditions Affecting Infants and Children: SectionDocument6 pagesOral Conditions Affecting Infants and Children: SectionsafiraplNo ratings yet
- The International Journal of Orthodontia.: Malocclusion and Mouth-Breathing.Document4 pagesThe International Journal of Orthodontia.: Malocclusion and Mouth-Breathing.SankhyaNo ratings yet
- Neville's Atlas of Oral Pathology - TEXTODocument488 pagesNeville's Atlas of Oral Pathology - TEXTOgagandeep singh100% (1)
- Flossophy Forsyth: N e W S L e T T e RDocument4 pagesFlossophy Forsyth: N e W S L e T T e RAnthony LiNo ratings yet
- Is It Possible To Define The Ideal Lips?: È Possibile Definire Le Labbra Ideali?Document6 pagesIs It Possible To Define The Ideal Lips?: È Possibile Definire Le Labbra Ideali?juanypatoNo ratings yet
- Unit 4: Class Ii: Jandel de Guzman Jamaica Faith Ramon Mesho Abdullah Hassan WadaDocument45 pagesUnit 4: Class Ii: Jandel de Guzman Jamaica Faith Ramon Mesho Abdullah Hassan Wadajamaica faith ramonNo ratings yet
- History and Physical Treatment / Management: Page 2 of 5Document1 pageHistory and Physical Treatment / Management: Page 2 of 5Adliah ZahiraNo ratings yet
- Ortho - Application-As-A-GdpDocument8 pagesOrtho - Application-As-A-Gdprajesh kumarNo ratings yet
- Cleft ReviewDocument4 pagesCleft ReviewAileen Delos Santos-GarciaNo ratings yet
- 10 - Altered Passive Eruption - The Undiagnosed EntityDocument4 pages10 - Altered Passive Eruption - The Undiagnosed EntityStefanie Lais Kreutz RosaNo ratings yet
- Bilateral Lip Repair FISHERDocument12 pagesBilateral Lip Repair FISHERKatherine Victoria Glass AllenNo ratings yet
- Correction of Ant Openbite Very Important PaperDocument18 pagesCorrection of Ant Openbite Very Important PaperMahdi ZakeriNo ratings yet
- Lec 13Document7 pagesLec 13Dr NisrinNo ratings yet
- A To Z Orthodontics Vol 5 Soft Tissue Morphology1Document23 pagesA To Z Orthodontics Vol 5 Soft Tissue Morphology1Ishtiaq HasanNo ratings yet
- Shaye CleftLipandPalateDocument17 pagesShaye CleftLipandPalatenurlatifahNo ratings yet
- Cleft Lip and PalateDocument5 pagesCleft Lip and PalateChristopher Ivan Herrera MontielNo ratings yet
- Cleft Lip and PalateDocument83 pagesCleft Lip and Palategracy davidNo ratings yet
- Cleft Lip & Cleft Palate FinalDocument39 pagesCleft Lip & Cleft Palate FinalHARINI LAKSHMI TUMULURINo ratings yet
- Incisal BiteDocument101 pagesIncisal Bitehaidar ALhlaichiNo ratings yet
- Huge Lymphangioma of The Tongue: A Case ReportDocument3 pagesHuge Lymphangioma of The Tongue: A Case ReportFaheem AhmedNo ratings yet
- Congenital MalformationsDocument20 pagesCongenital Malformationsapi-19500641No ratings yet
- Open Bite, A Review of Etiology and Manageme PDFDocument8 pagesOpen Bite, A Review of Etiology and Manageme PDFVieussens JoffreyNo ratings yet
- Cleft Lip, Cleft Palate, and Velopharyngeal.36Document19 pagesCleft Lip, Cleft Palate, and Velopharyngeal.36Jimmy Mejía Cirujano PlásticoNo ratings yet
- A Case Report: Combination Between Millard Technique and Paranasal Flap in Unilateral Cleft Lip and PalateDocument4 pagesA Case Report: Combination Between Millard Technique and Paranasal Flap in Unilateral Cleft Lip and PalateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Taping Cleft LipDocument9 pagesTaping Cleft LipfransiskalilieNo ratings yet
- Current Concept in Alveolar Cleft ManagementDocument9 pagesCurrent Concept in Alveolar Cleft ManagementYukianesaNo ratings yet
- The Prodtdontic Management of Cleft Palate: Maxillofacial Prosthetics Dental ImplantsDocument6 pagesThe Prodtdontic Management of Cleft Palate: Maxillofacial Prosthetics Dental ImplantsShraddha AgarwalNo ratings yet
- Cleft Lip Andpalate SurgeryDocument4 pagesCleft Lip Andpalate Surgerydr.rrajesh92No ratings yet
- Oral Dysfunction As A Cause of MalocclusionDocument6 pagesOral Dysfunction As A Cause of MalocclusionJULIA SANFURGO VILLARROELNo ratings yet
- 2015 Surgical Treatment of AnkyloglossiaDocument5 pages2015 Surgical Treatment of AnkyloglossiaDimitris RodriguezNo ratings yet
- Gorman 1967Document7 pagesGorman 1967jennifercampa2017No ratings yet
- AnkyloglossiaDocument5 pagesAnkyloglossiaLjubomirErdoglijaNo ratings yet
- Aetiology Diagnosis and Treatment of AnkyloglossiaDocument5 pagesAetiology Diagnosis and Treatment of AnkyloglossiaNaufal WahyuNo ratings yet
- Correction of Secondary Cleft Lip DeformitiesDocument11 pagesCorrection of Secondary Cleft Lip DeformitiesTraventure 2000No ratings yet
- Obh 5 PDFDocument7 pagesObh 5 PDFFajrul AkmalNo ratings yet
- Mollaoglu 2000Document8 pagesMollaoglu 2000MilenaNo ratings yet
- Functional Examination: Textbook of OrthodonticsDocument3 pagesFunctional Examination: Textbook of OrthodonticsndranNo ratings yet
- Cleft LectDocument76 pagesCleft LectDiandra Puspa WidyasariNo ratings yet
- Infographics III Blood Smear 27 07 2020Document1 pageInfographics III Blood Smear 27 07 2020MARIA AUBREY GOLIATNo ratings yet
- Cerebellum-Rr - 1 (Anatomy, Physiology, Biochemistry)Document215 pagesCerebellum-Rr - 1 (Anatomy, Physiology, Biochemistry)REACT ATTRACTSNo ratings yet
- Bone Growth and Factors That Associated With It1234Document7 pagesBone Growth and Factors That Associated With It1234Amanuel TarekegnNo ratings yet
- Effects of Rearing Temperature On HematologicalDocument5 pagesEffects of Rearing Temperature On HematologicalBlagojaNo ratings yet
- Full Ebook of Urinalysis and Body Fluids 7Th Edition Susan King Strasinger Da Mtascp Online PDF All ChapterDocument69 pagesFull Ebook of Urinalysis and Body Fluids 7Th Edition Susan King Strasinger Da Mtascp Online PDF All ChapteraamrizalezNo ratings yet
- Script - Sailent Feature of Insects OrderDocument14 pagesScript - Sailent Feature of Insects OrderKapil Kumar Sharma100% (1)
- Endocrine - FRCEM SuccessDocument110 pagesEndocrine - FRCEM SuccessskNo ratings yet
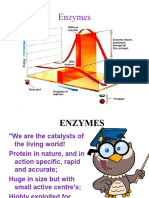
- EnzymeDocument80 pagesEnzymeGosa MohammedNo ratings yet
- Creatine Kinase: Store at 2-8ºCDocument4 pagesCreatine Kinase: Store at 2-8ºCLaboratorios HerliNo ratings yet
- Excellence in OrthodonticsDocument22 pagesExcellence in OrthodonticsAkram AlsharaeeNo ratings yet
- Chesmistry Trulab Pro Line LOT 89711 310-11-2024Document22 pagesChesmistry Trulab Pro Line LOT 89711 310-11-2024seksi sspk sarprasNo ratings yet
- Echanical Sphyxia: HapterDocument16 pagesEchanical Sphyxia: HapterJRNo ratings yet
- Six The Musical ScriptDocument32 pagesSix The Musical ScriptMaya SzirNo ratings yet
- 1st Quarter - Physical EducationDocument57 pages1st Quarter - Physical EducationJasmine Sinohin BagasinaNo ratings yet
- Basic BiomechanicsDocument54 pagesBasic BiomechanicsStevenDanielNo ratings yet
- Chapter 8 - Social Vision at The Interse - 2016 - Neuroimaging Personality SocDocument28 pagesChapter 8 - Social Vision at The Interse - 2016 - Neuroimaging Personality Socmi_shareNo ratings yet
- In - A Randomized Split Face Histomorphologic Study Comparing A Volumetric Calcium Hydroxylapatite and A Hyaluronic Acid Based Dermal FillerDocument6 pagesIn - A Randomized Split Face Histomorphologic Study Comparing A Volumetric Calcium Hydroxylapatite and A Hyaluronic Acid Based Dermal FillerFrancisco BotelhoNo ratings yet
- 1regional BlockDocument150 pages1regional BlockLilija SöderholmNo ratings yet
- Oralhisto FinalsDocument27 pagesOralhisto FinalsShiina MashiroNo ratings yet
- Importance of BiochemistryDocument5 pagesImportance of BiochemistryDICKSONNo ratings yet
- Group 5 Dissecting ActivityDocument10 pagesGroup 5 Dissecting Activityvincentelijah2911No ratings yet
- Approach To A Child With Anemia: Moderator - Dr. Vinod Kumari Ma'amDocument22 pagesApproach To A Child With Anemia: Moderator - Dr. Vinod Kumari Ma'amMedicine 0786No ratings yet
- Anemia During PregnancyDocument39 pagesAnemia During PregnancyBhawna JoshiNo ratings yet
- Respiration (Multiple Choice)Document27 pagesRespiration (Multiple Choice)mohamed Aita100% (1)
- PdfText - 2023-06-01T222329.740Document8 pagesPdfText - 2023-06-01T222329.740Rahul NemadeNo ratings yet
- Stoichiometry of Cell Growth and Product FormationDocument2 pagesStoichiometry of Cell Growth and Product Formationmneilg0% (1)
- Ijms 23 04115Document17 pagesIjms 23 04115Alejandra Fernández BastidasNo ratings yet
- OCR AS-Level Biology June 2023 Mark Scheme 1Document23 pagesOCR AS-Level Biology June 2023 Mark Scheme 1FatimaNo ratings yet
- Assessment of The Skin Hair and NailsDocument19 pagesAssessment of The Skin Hair and NailsBaniwas Marie AgnesNo ratings yet