Download as pdf or txt
You might also like
- Medicine Alaa Notes (All Files Merged) - Best Pro Choice-.Pdf-1Document120 pagesMedicine Alaa Notes (All Files Merged) - Best Pro Choice-.Pdf-1maimoona suleman100% (6)
- Adult Health Nursing McqsDocument27 pagesAdult Health Nursing McqsMuhammad Zeeshan100% (1)
- The Cholesterol Myths by Uffe RavnskovDocument26 pagesThe Cholesterol Myths by Uffe Ravnskov2361983No ratings yet
- Lipidaholics Anonymous Case 291 Can Losing Weight Worsen Lipids?Document14 pagesLipidaholics Anonymous Case 291 Can Losing Weight Worsen Lipids?Edmilson R. LimaNo ratings yet
- Dr. Bernstein'S Dr. Bernstein'SDocument11 pagesDr. Bernstein'S Dr. Bernstein'SManuel DíazNo ratings yet
- Lipid Disorders in The Elderly: GlossaryDocument4 pagesLipid Disorders in The Elderly: GlossaryAmelie AnsonNo ratings yet
- A Hyper - Emia A A PseudohyponatremiaDocument14 pagesA Hyper - Emia A A PseudohyponatremiaSrinivas PolikepatiNo ratings yet
- Cholesterol - Wed HarvardDocument7 pagesCholesterol - Wed HarvardNam NguyenHoangNo ratings yet
- Medical TerminologyDocument17 pagesMedical TerminologySofia Isabelle GarciaNo ratings yet
- Paper Work of High Cholesterol: English AssignmentDocument10 pagesPaper Work of High Cholesterol: English AssignmentVyeren VestalNo ratings yet
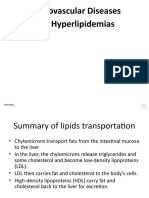
- Cardiovascular Diseases and Hyperlipidemias: Continuing.Document19 pagesCardiovascular Diseases and Hyperlipidemias: Continuing.Zai ZaiNo ratings yet
- HDL (Good) Cholesterol - HDL Stands For High-Density Lipoproteins. These AreDocument10 pagesHDL (Good) Cholesterol - HDL Stands For High-Density Lipoproteins. These ArenaliniNo ratings yet
- Diabetes Heart Disease and StrokeDocument12 pagesDiabetes Heart Disease and Strokerajasekaran_mNo ratings yet
- AtherosclerosisDocument51 pagesAtherosclerosisWilliam Wong100% (1)
- Causes of High Triglycerides and Their EffectsDocument1 pageCauses of High Triglycerides and Their EffectsRicardoBonoNo ratings yet
- Dislipidemias NiñosDocument7 pagesDislipidemias NiñosMarco Antonio Cervantes de JulianNo ratings yet
- Nutrition in Cardiovasular DiseaseDocument62 pagesNutrition in Cardiovasular DiseaseMalisa Fitri UmarNo ratings yet
- How Cholesterol WorksDocument7 pagesHow Cholesterol WorksVishal Kumar ShawNo ratings yet
- Lecture5-PracticalBiochemistry-LipidProfile 2Document41 pagesLecture5-PracticalBiochemistry-LipidProfile 2mhammadnjmaden45No ratings yet
- Fat and Its: Dietary Relation Heart Attacks and StrokesDocument5 pagesFat and Its: Dietary Relation Heart Attacks and StrokesNadhifah RahmawatiNo ratings yet
- Assignment Chem 1Document4 pagesAssignment Chem 1D AmanatNo ratings yet
- Chapter 8 (Laposata) - Blood Vessels (Lipids)Document14 pagesChapter 8 (Laposata) - Blood Vessels (Lipids)Wynna SegundoNo ratings yet
- 20 Questions On AtherosclerosisDocument5 pages20 Questions On AtherosclerosisPaul WestonNo ratings yet
- The Role of Lipids: PathogenesisDocument14 pagesThe Role of Lipids: PathogenesisironNo ratings yet
- Coronary Artery Diseas1Document3 pagesCoronary Artery Diseas1Stepyn SalvadorNo ratings yet
- Introduccion: Objetivo Marco Teorico Datos Generales Del Colesterol OrigenDocument3 pagesIntroduccion: Objetivo Marco Teorico Datos Generales Del Colesterol OrigenSusan ChinoNo ratings yet
- The Complete Guide to High Cholesterol: Symptoms, Risks, Treatments & CuresFrom EverandThe Complete Guide to High Cholesterol: Symptoms, Risks, Treatments & CuresNo ratings yet
- Screening and Management of DyslipidemiaDocument16 pagesScreening and Management of DyslipidemiaSakina GhaziNo ratings yet
- Positive Troponin Test: Lipid ProfileDocument4 pagesPositive Troponin Test: Lipid ProfileKyla Malapit GarvidaNo ratings yet
- Management of HyperlipidemiaDocument34 pagesManagement of HyperlipidemiaCarleta StanNo ratings yet
- Lipids Disorders: Biochemistry InstructorsDocument22 pagesLipids Disorders: Biochemistry InstructorsShaira Elyze GabrielNo ratings yet
- Hyper Cholesterol Emi ADocument7 pagesHyper Cholesterol Emi AMohamed EssallaaNo ratings yet
- High Cholesterol - Causes, Symptoms & TreatmentsDocument3 pagesHigh Cholesterol - Causes, Symptoms & TreatmentsTonny WijayaNo ratings yet
- Diet Heart MythDocument23 pagesDiet Heart MythΚυριακίδης ΚώσταςNo ratings yet
- CHOLESTROLDocument16 pagesCHOLESTROLalirifan2100% (1)
- The No-hoax Cholesterol Management Book: Bust the cholesterol myth, get clarity to get natural protection for life by knowing how to control & lower down cholesterol via medicine, exercise & dietFrom EverandThe No-hoax Cholesterol Management Book: Bust the cholesterol myth, get clarity to get natural protection for life by knowing how to control & lower down cholesterol via medicine, exercise & dietRating: 5 out of 5 stars5/5 (1)
- Lipid Journal 2024Document31 pagesLipid Journal 2024Agustina SamudioNo ratings yet
- Disorders of Lipid Metabolism LectureDocument55 pagesDisorders of Lipid Metabolism LectureRichard SiahaanNo ratings yet
- How To Interpret Your Blood Test ResultsDocument23 pagesHow To Interpret Your Blood Test Resultstin1625100% (1)
- Medical Nutrition Therapy For Cardiovascular DiseaseDocument210 pagesMedical Nutrition Therapy For Cardiovascular DiseaseBok MatthewNo ratings yet
- Everything You Need To Know About High CholesterolDocument25 pagesEverything You Need To Know About High Cholesterolnidia rahmaNo ratings yet
- A Level Biology NotesDocument16 pagesA Level Biology Notesmohammed100% (5)
- Jurnal HyperlipidemiaDocument12 pagesJurnal HyperlipidemiaJo LenongNo ratings yet
- CVDs in ElderlyDocument30 pagesCVDs in ElderlyDr. Arti MuleyNo ratings yet
- Dietary Cholesterol and The Lack of Evidence in Cardiovascular DiseaseDocument5 pagesDietary Cholesterol and The Lack of Evidence in Cardiovascular DiseaseWa ode Windra ByoNo ratings yet
- Chapter-Xi Lipid Profile TestsDocument4 pagesChapter-Xi Lipid Profile TestssabrinaNo ratings yet
- MUCLecture 2022 21411961Document4 pagesMUCLecture 2022 21411961Nazar NabeelNo ratings yet
- Plasma Lipid and Coronary Heart DiseaseDocument6 pagesPlasma Lipid and Coronary Heart Diseaseukosam10No ratings yet
- Non Communicable Disease Prevention and ControlDocument36 pagesNon Communicable Disease Prevention and ControlElcid Pimentel100% (1)
- High Blood CholesterolDocument3 pagesHigh Blood Cholesterolthe dark knightNo ratings yet
- Profil Lipid Dan Risiko Penyakit Jantung Koroner Andi Surya AmalDocument5 pagesProfil Lipid Dan Risiko Penyakit Jantung Koroner Andi Surya AmalAyu Dewi SuwantiNo ratings yet
- Management Strategies For Patients/Clients: DyslipidemiaDocument7 pagesManagement Strategies For Patients/Clients: DyslipidemiaminkyaoNo ratings yet
- A Consumer's Guide To FatsDocument8 pagesA Consumer's Guide To FatschotrainNo ratings yet
- Type II DiabetesDocument3 pagesType II DiabetesBarna ClaudiuNo ratings yet
- DyslipidemiaDocument20 pagesDyslipidemiaapi-261438047No ratings yet
- On Heart DiseaseDocument4 pagesOn Heart DiseaseRoberto Arteaga-AriasNo ratings yet
- Lecture 1 Carbohydrate 1Document39 pagesLecture 1 Carbohydrate 1mer12sswNo ratings yet
- Cardiovascular DiseaseDocument8 pagesCardiovascular DiseasemaheentextilemillsNo ratings yet
- CholesterolDocument2 pagesCholesterolAmit AroraNo ratings yet
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 4Document10 pagesDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 4ArtackNo ratings yet
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 5Document10 pagesDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 5ArtackNo ratings yet
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 3Document10 pagesDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 3ArtackNo ratings yet
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 2Document10 pagesDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars (PDFDrive) - 2ArtackNo ratings yet
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars 1Document10 pagesDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars 1Artack67% (3)
- Genetic Disorders: Recessive Disorders (Homozygous) Description Cases Per Birth Sickle Cell Disease (SCD)Document18 pagesGenetic Disorders: Recessive Disorders (Homozygous) Description Cases Per Birth Sickle Cell Disease (SCD)tango0385100% (1)
- Diabetes Prediction and Classification Using AI Based TechniquesDocument42 pagesDiabetes Prediction and Classification Using AI Based TechniquesNayana SNo ratings yet
- Update On Insulin Therapy For Type 2 DiabetesDocument9 pagesUpdate On Insulin Therapy For Type 2 DiabetesRIKANo ratings yet
- PEd 95 GallenoDocument2 pagesPEd 95 GallenoflgallenoNo ratings yet
- CHAPTER 6: Health Awareness NSTPDocument40 pagesCHAPTER 6: Health Awareness NSTPMarcilla Grace DellosaNo ratings yet
- Endocrine SystemDocument12 pagesEndocrine SystemChelsea GulfanNo ratings yet
- DocxDocument34 pagesDocxHoa LuuNo ratings yet
- Plant-Based Antidiabetic Nanoformulations: The Emerging Paradigm For EDocument44 pagesPlant-Based Antidiabetic Nanoformulations: The Emerging Paradigm For EAlyna AlynaNo ratings yet
- Chapter 2 Lesson 1 and 2Document14 pagesChapter 2 Lesson 1 and 22C1 - YABES, JenniferNo ratings yet
- The Food Timing DietDocument218 pagesThe Food Timing DietEdgar PeixotoNo ratings yet
- Keto DietDocument100 pagesKeto Dietmillie1971No ratings yet
- Defense of Low Fat (Devils Advocate by Minger)Document64 pagesDefense of Low Fat (Devils Advocate by Minger)simasNo ratings yet
- Pathologic Conditios of Endocrine Disorder.Document42 pagesPathologic Conditios of Endocrine Disorder.ramoli1988No ratings yet
- Thesis ADocument66 pagesThesis AMary Angelie Baguin100% (1)
- Running Head: CHILDHOOD OBESITY 1Document8 pagesRunning Head: CHILDHOOD OBESITY 1VirginiaNo ratings yet
- Effect of Vijaysar On Prediabetes Condition - A Review: Dr. Swapnil Padate and Dr. Renu P. RaokhandeDocument8 pagesEffect of Vijaysar On Prediabetes Condition - A Review: Dr. Swapnil Padate and Dr. Renu P. RaokhandeMOHAMMAD OVAISNo ratings yet
- Antidiabetic Effect of Syzygium Cumini L. Seed On Type 2 Diabetic RatsDocument8 pagesAntidiabetic Effect of Syzygium Cumini L. Seed On Type 2 Diabetic RatsLavanya Priya Sathyan100% (1)
- Fructose Is A MonosaccharideDocument10 pagesFructose Is A MonosaccharideUbaid ur RahmanNo ratings yet
- Intro To Medtech Clinical Chemistry ReviewerDocument11 pagesIntro To Medtech Clinical Chemistry Reviewerjesanndei100% (1)
- NCP - Case StudyDocument3 pagesNCP - Case StudyMary Joan Faye GarridoNo ratings yet
- CA Bar - Feb 2017 PDFDocument64 pagesCA Bar - Feb 2017 PDFTrial UserNo ratings yet
- Semi Final Exam in LeadershipDocument6 pagesSemi Final Exam in LeadershipJessa Mae JabegueroNo ratings yet
- Running Stuff 2018/2019Document103 pagesRunning Stuff 2018/2019Andrew Richard ThompsonNo ratings yet
- Ramadan Guide For DiabetesDocument9 pagesRamadan Guide For DiabetesUjwal TickooNo ratings yet
- Secretion of Bile and The Role of Bile Acids in DigestionDocument8 pagesSecretion of Bile and The Role of Bile Acids in DigestionMarianne Kristelle NonanNo ratings yet
- NUR100 Sherpath CH 45 Nutrition ImbalanceDocument4 pagesNUR100 Sherpath CH 45 Nutrition Imbalancecaloy2345caloyNo ratings yet
- (03241750 - Acta Medica Bulgarica) Trace Elements and Vitamin D in Gestational DiabetesDocument5 pages(03241750 - Acta Medica Bulgarica) Trace Elements and Vitamin D in Gestational DiabetesTeodorNo ratings yet
- Too Much Phosphate in The Blood Is Known As HyperphosphatemiaDocument7 pagesToo Much Phosphate in The Blood Is Known As HyperphosphatemiaKen ZiNo ratings yet