
Srikantha 2009
Srikantha 2009
You might also like
- Neil v. Watson - The Mind's Machine - Foundations of Brain and Behavior-Sinauer AssociatesDocument622 pagesNeil v. Watson - The Mind's Machine - Foundations of Brain and Behavior-Sinauer AssociatesChumchum Kumar100% (12)
- BSBLDR511 Develop and Use Emotional IntelligenceDocument13 pagesBSBLDR511 Develop and Use Emotional IntelligenceLayla Correa da SilvaNo ratings yet
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- Short-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyDocument12 pagesShort-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyTJPRC PublicationsNo ratings yet
- SPIROMETRYDocument9 pagesSPIROMETRYaeyousefNo ratings yet
- Ijcp-5481 oDocument6 pagesIjcp-5481 oDebasis ChatterjeeNo ratings yet
- Adult Minimal-Change Disease: Clinical Characteristics, Treatment, and OutcomesDocument9 pagesAdult Minimal-Change Disease: Clinical Characteristics, Treatment, and OutcomesMutiara RizkyNo ratings yet
- Euro J of Neurology - 2023 - Doorn - European Academy of Neurology Peripheral Nerve Society Guideline On Diagnosis andDocument29 pagesEuro J of Neurology - 2023 - Doorn - European Academy of Neurology Peripheral Nerve Society Guideline On Diagnosis andjcr87No ratings yet
- Ijvm2014 531689 PDFDocument6 pagesIjvm2014 531689 PDFReka HariskianaNo ratings yet
- Lucas 2014Document8 pagesLucas 2014Prima YosiNo ratings yet
- Spirometry in Children: Clinical ReviewDocument9 pagesSpirometry in Children: Clinical ReviewMoonNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document4 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Riri KumalaNo ratings yet
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNo ratings yet
- Effect of Prednisolone During Defervescence in Dengue Haemorrhagic Fever: An Open Label Controlled StudyDocument4 pagesEffect of Prednisolone During Defervescence in Dengue Haemorrhagic Fever: An Open Label Controlled StudyFabiola StellaNo ratings yet
- Red Blood Cell Transfusion: Decision Making in Pediatric Intensive Care UnitsDocument7 pagesRed Blood Cell Transfusion: Decision Making in Pediatric Intensive Care UnitsIndra AjaNo ratings yet
- A Clinical Study of Tuberculous Cervical LymphadenDocument5 pagesA Clinical Study of Tuberculous Cervical LymphadenAgung DewanggaNo ratings yet
- Gupta 2013Document5 pagesGupta 2013Dhruv MahajanNo ratings yet
- Benign Paroxysmal Positional Vertigo: Opportunities SquanderedDocument8 pagesBenign Paroxysmal Positional Vertigo: Opportunities SquanderedNia UtariNo ratings yet
- Subglottic Stenosis in Granulomatosis With Polyangiitis: The Role of Laryngotracheal ResectionDocument5 pagesSubglottic Stenosis in Granulomatosis With Polyangiitis: The Role of Laryngotracheal ResectionSamNo ratings yet
- Splenectomy in Children With Chronic ITP: Long-Term Efficacy and Relation Between Its Outcome and Responses To Previous TreatmentsDocument4 pagesSplenectomy in Children With Chronic ITP: Long-Term Efficacy and Relation Between Its Outcome and Responses To Previous TreatmentsVladimir Henry Triguero RosalesNo ratings yet
- Management Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaDocument4 pagesManagement Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Operative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-AnalysisDocument9 pagesOperative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-Analysisyarianna2No ratings yet
- Lovastatin For The Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled TrialDocument9 pagesLovastatin For The Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled TrialBpmStfbNo ratings yet
- 12 11 PBDocument168 pages12 11 PBYS NateNo ratings yet
- Claudia Craven VENTRICULOMEGALY CLASSIFICATIONDocument17 pagesClaudia Craven VENTRICULOMEGALY CLASSIFICATIONGUI VINCENo ratings yet
- Serum Thyroid-Stimulating Hormone Is An Independent Risk Factor of Recurrent Guillain-Barré SyndromeDocument41 pagesSerum Thyroid-Stimulating Hormone Is An Independent Risk Factor of Recurrent Guillain-Barré SyndromeDr NIVEDITHA CNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Clin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiDocument18 pagesClin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiJesus Salvador SerratoNo ratings yet
- Case Studies of Lower Respiratory Tract InfectionsDocument25 pagesCase Studies of Lower Respiratory Tract InfectionsMarianNo ratings yet
- Tourniquet TestingDocument6 pagesTourniquet TestingPatrick RamosNo ratings yet
- Tto Crup NatureDocument7 pagesTto Crup NatureCarolina Mora RuedaNo ratings yet
- Kwong 2012Document8 pagesKwong 2012Ke XuNo ratings yet
- To Study Hematological Profile in Covid-19 Patients in Relation With Prognosis and Outcome: - A Cross Sectional Observational StudyDocument7 pagesTo Study Hematological Profile in Covid-19 Patients in Relation With Prognosis and Outcome: - A Cross Sectional Observational StudyIJAR JOURNALNo ratings yet
- PESI Critical Care 2005Document6 pagesPESI Critical Care 2005Rocio Méndez FrancoNo ratings yet
- A Prospective Observational Study of Dengue Fever With Thrombocytopenia With Reference To TreatmentDocument6 pagesA Prospective Observational Study of Dengue Fever With Thrombocytopenia With Reference To Treatment-Tony Santoso Putra-No ratings yet
- Pediatric Hematology Oncology JournalDocument4 pagesPediatric Hematology Oncology JournalmitraNo ratings yet
- Long-Term Clinical Outcome of Fetal Cell Transplantation For Parkinson Disease Two Case ReportsDocument5 pagesLong-Term Clinical Outcome of Fetal Cell Transplantation For Parkinson Disease Two Case Reportsjust for download matterNo ratings yet
- Cerebral Venous Thrombosis: Clinical Predictors and Emerging TreatmentsDocument3 pagesCerebral Venous Thrombosis: Clinical Predictors and Emerging Treatmentschartreuse avonleaNo ratings yet
- Chest: Point/Counterpoint EditorialsDocument3 pagesChest: Point/Counterpoint Editorialsgiseladelarosa2006No ratings yet
- Comparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverDocument6 pagesComparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverFayza RihastaraNo ratings yet
- GBS PDTDocument8 pagesGBS PDTabdulkadirmunsyNo ratings yet
- VP Shunt For Meningitis TBDocument9 pagesVP Shunt For Meningitis TBNindi LizenNo ratings yet
- Emboli ParuDocument10 pagesEmboli Paruindry_purnamasariNo ratings yet
- 10.1007@s12098 020 03454 1Document6 pages10.1007@s12098 020 03454 1rayhantaswinNo ratings yet
- DIC in Abruptio 2Document5 pagesDIC in Abruptio 2HoneylynNo ratings yet
- Comparison of 3 Clinical Models For Predicting The Probability of Pulmonary EmbolismDocument8 pagesComparison of 3 Clinical Models For Predicting The Probability of Pulmonary EmbolismAlirio Rodrigo Bastidas GoyesNo ratings yet
- Fluctuaciones Relacionadas A Tratamiento GBDocument7 pagesFluctuaciones Relacionadas A Tratamiento GBOsvaldo CortésNo ratings yet
- Decompressive Hemicraniectomy and DuroplastyDocument5 pagesDecompressive Hemicraniectomy and DuroplastyAmy NilifdaNo ratings yet
- JHM 2112Document4 pagesJHM 2112senkonenNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Lung Ultrasound Dry WeightDocument16 pagesLung Ultrasound Dry WeightBhanu KumarNo ratings yet
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 pagesRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNo ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- Baca IniDocument9 pagesBaca IniRahmi Annisa MaharaniNo ratings yet
- Wetzel2020 Article Flow-regulatedVersusDifferentiDocument7 pagesWetzel2020 Article Flow-regulatedVersusDifferenticNo ratings yet
- Neurourology and Urodynamics - 2022 - Martin - Is Sacral Neuromodulation Effective in Patients With Parkinson S Disease ADocument7 pagesNeurourology and Urodynamics - 2022 - Martin - Is Sacral Neuromodulation Effective in Patients With Parkinson S Disease AElkin JNo ratings yet
- Kansal 2018Document1 pageKansal 2018Sheena Mae MansinadesNo ratings yet
- 1 s2.0 S074152140290621X MainDocument6 pages1 s2.0 S074152140290621X Main1751010307No ratings yet
- GBS European Guidelines 2023Document29 pagesGBS European Guidelines 2023Saurabh AgrawalNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Abdominal Acupuncture For DepressionDocument35 pagesAbdominal Acupuncture For DepressionAGNESE YOLOTZIN OLIVERA TORO REYESNo ratings yet
- Cannabis Legal Regulatory Update April June 2019Document19 pagesCannabis Legal Regulatory Update April June 2019stonerhinoNo ratings yet
- Research in Primary Dental Care 1 PDFDocument4 pagesResearch in Primary Dental Care 1 PDFMARIA NAENo ratings yet
- الإجازات المرضية - منصة صحةDocument2 pagesالإجازات المرضية - منصة صحةShatha miNo ratings yet
- Region of Waterloo Job DescriptionDocument4 pagesRegion of Waterloo Job Descriptionbeth aguirreNo ratings yet
- Ebsco Fulltext 2024 03 20Document17 pagesEbsco Fulltext 2024 03 20api-733905896No ratings yet
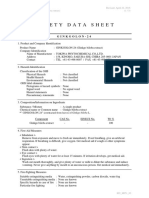
- MSDS GINKGOLON-24 (Ginkgo Biloba Ext)Document3 pagesMSDS GINKGOLON-24 (Ginkgo Biloba Ext)Selviani Dwi MuryantiNo ratings yet
- 2-NBDG As A Fluorescent Indicator For Direct Glucose Uptake MeasurementDocument9 pages2-NBDG As A Fluorescent Indicator For Direct Glucose Uptake MeasurementPili CárdenasNo ratings yet
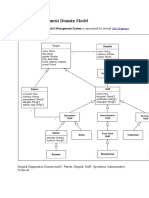
- Hospital Management Domain ModelDocument4 pagesHospital Management Domain Modelvinod kapateNo ratings yet
- PD Lesson 5 Coping With Stress in Middle and Late AdolescenceDocument16 pagesPD Lesson 5 Coping With Stress in Middle and Late AdolescenceEL FuentesNo ratings yet
- Developmental DelayDocument79 pagesDevelopmental DelayNaveen KumarNo ratings yet
- Glycolic Acid SdsDocument11 pagesGlycolic Acid SdsJuthi RahmanNo ratings yet
- Cardio DrugsDocument58 pagesCardio DrugsMARIA ROWENA VIA J. LUCENANo ratings yet
- Management Is Nothing More Than Motivating Other People GHEORGHE MDocument6 pagesManagement Is Nothing More Than Motivating Other People GHEORGHE MCristina PaliuNo ratings yet
- Buntis Congress Report 2021Document24 pagesBuntis Congress Report 2021Giselle ArenasNo ratings yet
- Antibiotic Prophylaxis OrthoDocument4 pagesAntibiotic Prophylaxis OrthoDonNo ratings yet
- Prosthesis For Long Span Kennedy's Class III Partially Edentulous Condition: A Case ReportDocument5 pagesProsthesis For Long Span Kennedy's Class III Partially Edentulous Condition: A Case ReportRiana WidiantyNo ratings yet
- HMB342 Course Syllabus Summer 2020Document5 pagesHMB342 Course Syllabus Summer 2020WangNo ratings yet
- Lifting Plan: Table of ContentDocument11 pagesLifting Plan: Table of ContentkhurramNo ratings yet
- ICN Framework of Disaster NursingDocument18 pagesICN Framework of Disaster NursingKRIZIA ANE A. SULONG100% (1)
- Element - 45 - 978-Design ReportDocument15 pagesElement - 45 - 978-Design ReportLeeNo ratings yet
- Product: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedDocument12 pagesProduct: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedSumon Das DasNo ratings yet
- Disability and Life Writing: Reports From The Nineteenth-Century AsylumDocument19 pagesDisability and Life Writing: Reports From The Nineteenth-Century AsylumHS22D001 MalavikaNo ratings yet
- UNIV144 Questions 2Document8 pagesUNIV144 Questions 2Clinton SmaugNo ratings yet
- Resume Igd Rsud PareDocument66 pagesResume Igd Rsud PareIqbalRazifNo ratings yet
- Pediatric Community Acquired PneumoniaDocument24 pagesPediatric Community Acquired PneumoniaJames Lagamayo JavierNo ratings yet
- PARENT AWARENESS SEMINAR-hand OutsDocument2 pagesPARENT AWARENESS SEMINAR-hand OutsLADY ANN GRACE LAGASNo ratings yet
- CPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sDocument2 pagesCPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sRacquel SolivenNo ratings yet
























































































Download as pdf or txt
You might also like
- Neil v. Watson - The Mind's Machine - Foundations of Brain and Behavior-Sinauer AssociatesDocument622 pagesNeil v. Watson - The Mind's Machine - Foundations of Brain and Behavior-Sinauer AssociatesChumchum Kumar100% (12)
- BSBLDR511 Develop and Use Emotional IntelligenceDocument13 pagesBSBLDR511 Develop and Use Emotional IntelligenceLayla Correa da SilvaNo ratings yet
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- Short-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyDocument12 pagesShort-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyTJPRC PublicationsNo ratings yet
- SPIROMETRYDocument9 pagesSPIROMETRYaeyousefNo ratings yet
- Ijcp-5481 oDocument6 pagesIjcp-5481 oDebasis ChatterjeeNo ratings yet
- Adult Minimal-Change Disease: Clinical Characteristics, Treatment, and OutcomesDocument9 pagesAdult Minimal-Change Disease: Clinical Characteristics, Treatment, and OutcomesMutiara RizkyNo ratings yet
- Euro J of Neurology - 2023 - Doorn - European Academy of Neurology Peripheral Nerve Society Guideline On Diagnosis andDocument29 pagesEuro J of Neurology - 2023 - Doorn - European Academy of Neurology Peripheral Nerve Society Guideline On Diagnosis andjcr87No ratings yet
- Ijvm2014 531689 PDFDocument6 pagesIjvm2014 531689 PDFReka HariskianaNo ratings yet
- Lucas 2014Document8 pagesLucas 2014Prima YosiNo ratings yet
- Spirometry in Children: Clinical ReviewDocument9 pagesSpirometry in Children: Clinical ReviewMoonNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document4 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Riri KumalaNo ratings yet
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNo ratings yet
- Effect of Prednisolone During Defervescence in Dengue Haemorrhagic Fever: An Open Label Controlled StudyDocument4 pagesEffect of Prednisolone During Defervescence in Dengue Haemorrhagic Fever: An Open Label Controlled StudyFabiola StellaNo ratings yet
- Red Blood Cell Transfusion: Decision Making in Pediatric Intensive Care UnitsDocument7 pagesRed Blood Cell Transfusion: Decision Making in Pediatric Intensive Care UnitsIndra AjaNo ratings yet
- A Clinical Study of Tuberculous Cervical LymphadenDocument5 pagesA Clinical Study of Tuberculous Cervical LymphadenAgung DewanggaNo ratings yet
- Gupta 2013Document5 pagesGupta 2013Dhruv MahajanNo ratings yet
- Benign Paroxysmal Positional Vertigo: Opportunities SquanderedDocument8 pagesBenign Paroxysmal Positional Vertigo: Opportunities SquanderedNia UtariNo ratings yet
- Subglottic Stenosis in Granulomatosis With Polyangiitis: The Role of Laryngotracheal ResectionDocument5 pagesSubglottic Stenosis in Granulomatosis With Polyangiitis: The Role of Laryngotracheal ResectionSamNo ratings yet
- Splenectomy in Children With Chronic ITP: Long-Term Efficacy and Relation Between Its Outcome and Responses To Previous TreatmentsDocument4 pagesSplenectomy in Children With Chronic ITP: Long-Term Efficacy and Relation Between Its Outcome and Responses To Previous TreatmentsVladimir Henry Triguero RosalesNo ratings yet
- Management Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaDocument4 pagesManagement Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Operative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-AnalysisDocument9 pagesOperative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-Analysisyarianna2No ratings yet
- Lovastatin For The Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled TrialDocument9 pagesLovastatin For The Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled TrialBpmStfbNo ratings yet
- 12 11 PBDocument168 pages12 11 PBYS NateNo ratings yet
- Claudia Craven VENTRICULOMEGALY CLASSIFICATIONDocument17 pagesClaudia Craven VENTRICULOMEGALY CLASSIFICATIONGUI VINCENo ratings yet
- Serum Thyroid-Stimulating Hormone Is An Independent Risk Factor of Recurrent Guillain-Barré SyndromeDocument41 pagesSerum Thyroid-Stimulating Hormone Is An Independent Risk Factor of Recurrent Guillain-Barré SyndromeDr NIVEDITHA CNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Clin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiDocument18 pagesClin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiJesus Salvador SerratoNo ratings yet
- Case Studies of Lower Respiratory Tract InfectionsDocument25 pagesCase Studies of Lower Respiratory Tract InfectionsMarianNo ratings yet
- Tourniquet TestingDocument6 pagesTourniquet TestingPatrick RamosNo ratings yet
- Tto Crup NatureDocument7 pagesTto Crup NatureCarolina Mora RuedaNo ratings yet
- Kwong 2012Document8 pagesKwong 2012Ke XuNo ratings yet
- To Study Hematological Profile in Covid-19 Patients in Relation With Prognosis and Outcome: - A Cross Sectional Observational StudyDocument7 pagesTo Study Hematological Profile in Covid-19 Patients in Relation With Prognosis and Outcome: - A Cross Sectional Observational StudyIJAR JOURNALNo ratings yet
- PESI Critical Care 2005Document6 pagesPESI Critical Care 2005Rocio Méndez FrancoNo ratings yet
- A Prospective Observational Study of Dengue Fever With Thrombocytopenia With Reference To TreatmentDocument6 pagesA Prospective Observational Study of Dengue Fever With Thrombocytopenia With Reference To Treatment-Tony Santoso Putra-No ratings yet
- Pediatric Hematology Oncology JournalDocument4 pagesPediatric Hematology Oncology JournalmitraNo ratings yet
- Long-Term Clinical Outcome of Fetal Cell Transplantation For Parkinson Disease Two Case ReportsDocument5 pagesLong-Term Clinical Outcome of Fetal Cell Transplantation For Parkinson Disease Two Case Reportsjust for download matterNo ratings yet
- Cerebral Venous Thrombosis: Clinical Predictors and Emerging TreatmentsDocument3 pagesCerebral Venous Thrombosis: Clinical Predictors and Emerging Treatmentschartreuse avonleaNo ratings yet
- Chest: Point/Counterpoint EditorialsDocument3 pagesChest: Point/Counterpoint Editorialsgiseladelarosa2006No ratings yet
- Comparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverDocument6 pagesComparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverFayza RihastaraNo ratings yet
- GBS PDTDocument8 pagesGBS PDTabdulkadirmunsyNo ratings yet
- VP Shunt For Meningitis TBDocument9 pagesVP Shunt For Meningitis TBNindi LizenNo ratings yet
- Emboli ParuDocument10 pagesEmboli Paruindry_purnamasariNo ratings yet
- 10.1007@s12098 020 03454 1Document6 pages10.1007@s12098 020 03454 1rayhantaswinNo ratings yet
- DIC in Abruptio 2Document5 pagesDIC in Abruptio 2HoneylynNo ratings yet
- Comparison of 3 Clinical Models For Predicting The Probability of Pulmonary EmbolismDocument8 pagesComparison of 3 Clinical Models For Predicting The Probability of Pulmonary EmbolismAlirio Rodrigo Bastidas GoyesNo ratings yet
- Fluctuaciones Relacionadas A Tratamiento GBDocument7 pagesFluctuaciones Relacionadas A Tratamiento GBOsvaldo CortésNo ratings yet
- Decompressive Hemicraniectomy and DuroplastyDocument5 pagesDecompressive Hemicraniectomy and DuroplastyAmy NilifdaNo ratings yet
- JHM 2112Document4 pagesJHM 2112senkonenNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Lung Ultrasound Dry WeightDocument16 pagesLung Ultrasound Dry WeightBhanu KumarNo ratings yet
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 pagesRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNo ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- Baca IniDocument9 pagesBaca IniRahmi Annisa MaharaniNo ratings yet
- Wetzel2020 Article Flow-regulatedVersusDifferentiDocument7 pagesWetzel2020 Article Flow-regulatedVersusDifferenticNo ratings yet
- Neurourology and Urodynamics - 2022 - Martin - Is Sacral Neuromodulation Effective in Patients With Parkinson S Disease ADocument7 pagesNeurourology and Urodynamics - 2022 - Martin - Is Sacral Neuromodulation Effective in Patients With Parkinson S Disease AElkin JNo ratings yet
- Kansal 2018Document1 pageKansal 2018Sheena Mae MansinadesNo ratings yet
- 1 s2.0 S074152140290621X MainDocument6 pages1 s2.0 S074152140290621X Main1751010307No ratings yet
- GBS European Guidelines 2023Document29 pagesGBS European Guidelines 2023Saurabh AgrawalNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Abdominal Acupuncture For DepressionDocument35 pagesAbdominal Acupuncture For DepressionAGNESE YOLOTZIN OLIVERA TORO REYESNo ratings yet
- Cannabis Legal Regulatory Update April June 2019Document19 pagesCannabis Legal Regulatory Update April June 2019stonerhinoNo ratings yet
- Research in Primary Dental Care 1 PDFDocument4 pagesResearch in Primary Dental Care 1 PDFMARIA NAENo ratings yet
- الإجازات المرضية - منصة صحةDocument2 pagesالإجازات المرضية - منصة صحةShatha miNo ratings yet
- Region of Waterloo Job DescriptionDocument4 pagesRegion of Waterloo Job Descriptionbeth aguirreNo ratings yet
- Ebsco Fulltext 2024 03 20Document17 pagesEbsco Fulltext 2024 03 20api-733905896No ratings yet
- MSDS GINKGOLON-24 (Ginkgo Biloba Ext)Document3 pagesMSDS GINKGOLON-24 (Ginkgo Biloba Ext)Selviani Dwi MuryantiNo ratings yet
- 2-NBDG As A Fluorescent Indicator For Direct Glucose Uptake MeasurementDocument9 pages2-NBDG As A Fluorescent Indicator For Direct Glucose Uptake MeasurementPili CárdenasNo ratings yet
- Hospital Management Domain ModelDocument4 pagesHospital Management Domain Modelvinod kapateNo ratings yet
- PD Lesson 5 Coping With Stress in Middle and Late AdolescenceDocument16 pagesPD Lesson 5 Coping With Stress in Middle and Late AdolescenceEL FuentesNo ratings yet
- Developmental DelayDocument79 pagesDevelopmental DelayNaveen KumarNo ratings yet
- Glycolic Acid SdsDocument11 pagesGlycolic Acid SdsJuthi RahmanNo ratings yet
- Cardio DrugsDocument58 pagesCardio DrugsMARIA ROWENA VIA J. LUCENANo ratings yet
- Management Is Nothing More Than Motivating Other People GHEORGHE MDocument6 pagesManagement Is Nothing More Than Motivating Other People GHEORGHE MCristina PaliuNo ratings yet
- Buntis Congress Report 2021Document24 pagesBuntis Congress Report 2021Giselle ArenasNo ratings yet
- Antibiotic Prophylaxis OrthoDocument4 pagesAntibiotic Prophylaxis OrthoDonNo ratings yet
- Prosthesis For Long Span Kennedy's Class III Partially Edentulous Condition: A Case ReportDocument5 pagesProsthesis For Long Span Kennedy's Class III Partially Edentulous Condition: A Case ReportRiana WidiantyNo ratings yet
- HMB342 Course Syllabus Summer 2020Document5 pagesHMB342 Course Syllabus Summer 2020WangNo ratings yet
- Lifting Plan: Table of ContentDocument11 pagesLifting Plan: Table of ContentkhurramNo ratings yet
- ICN Framework of Disaster NursingDocument18 pagesICN Framework of Disaster NursingKRIZIA ANE A. SULONG100% (1)
- Element - 45 - 978-Design ReportDocument15 pagesElement - 45 - 978-Design ReportLeeNo ratings yet
- Product: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedDocument12 pagesProduct: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedSumon Das DasNo ratings yet
- Disability and Life Writing: Reports From The Nineteenth-Century AsylumDocument19 pagesDisability and Life Writing: Reports From The Nineteenth-Century AsylumHS22D001 MalavikaNo ratings yet
- UNIV144 Questions 2Document8 pagesUNIV144 Questions 2Clinton SmaugNo ratings yet
- Resume Igd Rsud PareDocument66 pagesResume Igd Rsud PareIqbalRazifNo ratings yet
- Pediatric Community Acquired PneumoniaDocument24 pagesPediatric Community Acquired PneumoniaJames Lagamayo JavierNo ratings yet
- PARENT AWARENESS SEMINAR-hand OutsDocument2 pagesPARENT AWARENESS SEMINAR-hand OutsLADY ANN GRACE LAGASNo ratings yet
- CPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sDocument2 pagesCPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sRacquel SolivenNo ratings yet