Download as pdf or txt
You might also like
- Cardiac/Cardiogenic Shock: Clinical Practice GuidelinesDocument3 pagesCardiac/Cardiogenic Shock: Clinical Practice GuidelinesAnonymous Yo0mStNo ratings yet
- TOTDocument19 pagesTOTKoj LozadaNo ratings yet
- Part 2 Exam Sample Q 2015Document194 pagesPart 2 Exam Sample Q 2015Abdul QuyyumNo ratings yet
- Hypertensive Emergencies: or How I Learned To Stop Worrying and Love LabetalolDocument31 pagesHypertensive Emergencies: or How I Learned To Stop Worrying and Love LabetalolNerissa AlvianaNo ratings yet
- IM CASE RTR - Myocardial InfarctionDocument47 pagesIM CASE RTR - Myocardial InfarctionTrisNo ratings yet
- How To Deal With Acute Dyspneu in ER: Acute Heart Failure OR Pulmonary Problem?Document36 pagesHow To Deal With Acute Dyspneu in ER: Acute Heart Failure OR Pulmonary Problem?tyasNo ratings yet
- Hypertensive Crises - Current ApproachDocument35 pagesHypertensive Crises - Current ApproachShre RanjithamNo ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- Crisis Hypertension: Dr. Isra Sukhraini NSTDocument21 pagesCrisis Hypertension: Dr. Isra Sukhraini NSTAndika SiswantaNo ratings yet
- Cardiac Content WyattDocument90 pagesCardiac Content WyattAnni BarbaNo ratings yet
- Syok KardiogenikDocument31 pagesSyok KardiogenikcantikarevieraNo ratings yet
- OxygenationDocument85 pagesOxygenationDemuel Dee L. BertoNo ratings yet
- 3 Hypertension Emergency and Urgency 2016Document31 pages3 Hypertension Emergency and Urgency 2016tyleree3No ratings yet
- Hypertension: Sahala Panggabean Bagian Ilmu Penyakit Dalam Fakultas Kedokteran Universitas Kristen IndonesiaDocument41 pagesHypertension: Sahala Panggabean Bagian Ilmu Penyakit Dalam Fakultas Kedokteran Universitas Kristen IndonesiaLeonardho Bayu WijayantoNo ratings yet
- Cerebrovascular Accidents: Stroke Versus TIADocument19 pagesCerebrovascular Accidents: Stroke Versus TIASagar ShahNo ratings yet
- CardioDocument9 pagesCardioVirgilio Reyes ManuelNo ratings yet
- Emergency Care For MO - Cardiac EmergenciesDocument64 pagesEmergency Care For MO - Cardiac Emergenciesdgdas4No ratings yet
- Hypertensive Crisis: - Alexter John C. Fajardo M.DDocument49 pagesHypertensive Crisis: - Alexter John C. Fajardo M.DAlexter John Cabalonga FajardoNo ratings yet
- HTN Emergency FinalDocument6 pagesHTN Emergency FinalMoad AlzaiimNo ratings yet
- Myocardial Infarctions: Medical Ward, 2022Document14 pagesMyocardial Infarctions: Medical Ward, 2022liahgibreNo ratings yet
- Management of Common Cases in Emergency MedicineDocument55 pagesManagement of Common Cases in Emergency MedicinemonpyitharNo ratings yet
- Acute HF-IAIDocument49 pagesAcute HF-IAIAndita ListyannisaNo ratings yet
- Crisis of Hypertension Revised 1Document57 pagesCrisis of Hypertension Revised 1keenmunir100% (4)
- Anti ArrhythmicsDocument32 pagesAnti ArrhythmicsdNo ratings yet
- Er FinalsDocument63 pagesEr FinalsNaren RaviNo ratings yet
- Hipertensi KrisisDocument30 pagesHipertensi KrisisLuthfan HakimNo ratings yet
- Jantung - Acute Heart FailureDocument32 pagesJantung - Acute Heart FailurefaradibaNo ratings yet
- Cardiac Emergencies: and How To Deal With ThemDocument62 pagesCardiac Emergencies: and How To Deal With ThemNaddia AyuNo ratings yet
- Acute Coronary Syndrome EditedDocument38 pagesAcute Coronary Syndrome EditedSurgicalgownNo ratings yet
- DR Philip Swales - GIM 22 MayDocument34 pagesDR Philip Swales - GIM 22 MaySathvika BNo ratings yet
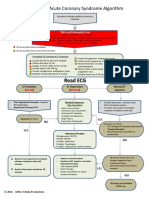
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction Algorithmjitendra magarNo ratings yet
- ACS - Dr. BennyDocument45 pagesACS - Dr. Bennyutari rahmaNo ratings yet
- Women Guideline FixDocument24 pagesWomen Guideline FixAndika SiswantaNo ratings yet
- Hypertensive CrisisDocument17 pagesHypertensive CrisisRaymund Christopher Dela PeñaNo ratings yet
- Acute Coronary Syndrome: Case PresentationDocument4 pagesAcute Coronary Syndrome: Case PresentationJunathan L. DelgadoNo ratings yet
- HPN CRISIS WordDocument9 pagesHPN CRISIS WordChaudhary AbhishekNo ratings yet
- Coronary Artery Disease: Aleson Claire A. Llanes, MDDocument94 pagesCoronary Artery Disease: Aleson Claire A. Llanes, MDFly LlanesNo ratings yet
- Homologous Blood Trasfusion Practice ShortsDocument23 pagesHomologous Blood Trasfusion Practice ShortsdrprasadingleyNo ratings yet
- Emergency Hypertension (Herbesser Injection)Document18 pagesEmergency Hypertension (Herbesser Injection)suho exoNo ratings yet
- Hypertensive Krisis 23-10-18Document23 pagesHypertensive Krisis 23-10-18Shone NamNo ratings yet
- Pcol Cover To CoverDocument214 pagesPcol Cover To CoverJec OcampoNo ratings yet
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- Crisis of Hypertension Revised 1Document57 pagesCrisis of Hypertension Revised 1Ratna Puspa RahayuNo ratings yet
- ACS (Dr. Thamrin 2015)Document43 pagesACS (Dr. Thamrin 2015)ok sogatenNo ratings yet
- Lecture - 2 Advanced Cardiac Life SupportDocument28 pagesLecture - 2 Advanced Cardiac Life SupportJixon GeorgeNo ratings yet
- HypertensionDocument34 pagesHypertensionThảo MyNo ratings yet
- Cardiac AnesthesiologyDocument48 pagesCardiac AnesthesiologyNiaNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction AlgorithmHan OWNo ratings yet
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki Hartawan100% (1)
- Hipertensi 2019Document82 pagesHipertensi 2019Nadia AaqilahNo ratings yet
- How I Manage DiureticsDocument31 pagesHow I Manage DiureticsNish ShahNo ratings yet
- UntitledDocument8 pagesUntitledabhijithmvNo ratings yet
- 10.15 Edrian Zulkarnain - ShockDocument42 pages10.15 Edrian Zulkarnain - ShockBintang UbamnataNo ratings yet
- JNC ViiiDocument45 pagesJNC ViiiNurul F AzzahraNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- High Yield Surgery Compatible Version PDFDocument20 pagesHigh Yield Surgery Compatible Version PDFSurgery CSC1No ratings yet
- Penatalaksanaan Penyulit Gagal JantungDocument17 pagesPenatalaksanaan Penyulit Gagal JantungarumNo ratings yet
- Blood Transfusion and Conservation: Dr. T.C. KriplaniDocument45 pagesBlood Transfusion and Conservation: Dr. T.C. KriplaniParvathy R NairNo ratings yet
- High Yield Surgery Compatible Version-2Document20 pagesHigh Yield Surgery Compatible Version-2zoozsuhai2No ratings yet
- HeartFailure Nursing FIK 2014Document101 pagesHeartFailure Nursing FIK 2014Putri NurlaeliNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Nidana Panchaka 1-7Document73 pagesNidana Panchaka 1-7Sreeja Mohandas100% (1)
- Osce ReviewerDocument119 pagesOsce Reviewerchiaruuh tNo ratings yet
- Apovian 2016Document10 pagesApovian 2016Sandy PranadaNo ratings yet
- Epidemiology and Current Status of Al-Lergic Rhinitis and Asthma in Thailand - ARIA Asia-Pacific Workshop ReportDocument8 pagesEpidemiology and Current Status of Al-Lergic Rhinitis and Asthma in Thailand - ARIA Asia-Pacific Workshop ReportThadchai SuwanwarangkoolNo ratings yet
- Must Know BloodbankingDocument25 pagesMust Know BloodbankingMaybelline TanNo ratings yet
- College FormularyDocument142 pagesCollege FormularymarcuscainedNo ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet
- Antipyretic-Analgesic and Anti-Inflammatory Drugs (Nsaids)Document43 pagesAntipyretic-Analgesic and Anti-Inflammatory Drugs (Nsaids)Ritu ShewaniNo ratings yet
- NURS325 05 Antepartum ComplicationDocument81 pagesNURS325 05 Antepartum ComplicationaliNo ratings yet
- G Friends Forensic Toxi SpecialDocument51 pagesG Friends Forensic Toxi SpecialAdam ZaaadNo ratings yet
- Wa0002.Document26 pagesWa0002.Sreeja ReddyNo ratings yet
- Influence of Micronutrients On Brain FunctionDocument25 pagesInfluence of Micronutrients On Brain FunctionAyesha UmerNo ratings yet
- Cases Elog BookDocument13 pagesCases Elog BookFaryal UfaqNo ratings yet
- Cme (Tdhi)Document64 pagesCme (Tdhi)OB-Gyne TDHINo ratings yet
- Lecture 6 LungsDocument14 pagesLecture 6 LungsOsama MalikNo ratings yet
- ProgeriaDocument1 pageProgeria_gabbbbbyy k :)100% (3)
- Allergic Fungal Rhinosinusitis: Clinical Commentary ReviewDocument6 pagesAllergic Fungal Rhinosinusitis: Clinical Commentary ReviewPutri YunandaNo ratings yet
- Arrhythmias: Domina Petric, MDDocument22 pagesArrhythmias: Domina Petric, MDMwaba PeterNo ratings yet
- Gastric CarcinomaDocument30 pagesGastric Carcinomaapi-19641337100% (1)
- Cholinesterase Inhibitors From Plants Po PDFDocument17 pagesCholinesterase Inhibitors From Plants Po PDFVenkateswar RaoNo ratings yet
- HypotoniaDocument45 pagesHypotoniaاثير اااNo ratings yet
- Urine Physical Sediment1819Document23 pagesUrine Physical Sediment1819Anas ShwbkNo ratings yet
- MycosesDocument2 pagesMycosesMadabout MusicNo ratings yet
- C CRN Exam HandbookDocument42 pagesC CRN Exam HandbookFitz JaminitNo ratings yet
- Flfghfuid Elefghgfhctrolytes Cheat SheetDocument1 pageFlfghfuid Elefghgfhctrolytes Cheat SheetRăzvan RoșcaNo ratings yet
- TR-SENSES MercadoDocument174 pagesTR-SENSES MercadoroseNo ratings yet
- Claas Mowers Disco 3600 F Disco 3500 FRC Assembly Instruction FR de en RuDocument23 pagesClaas Mowers Disco 3600 F Disco 3500 FRC Assembly Instruction FR de en Rumarkrush140898asj100% (91)
- Magnetic Resonance Spectroscopy and Its Clinical Applications: A ReviewDocument21 pagesMagnetic Resonance Spectroscopy and Its Clinical Applications: A Reviewale saenzNo ratings yet