Download as pdf or txt
You might also like
- Neurological AssessmentDocument10 pagesNeurological AssessmentKristine AlejandroNo ratings yet
- NPTE Sullivan EXAM BDocument131 pagesNPTE Sullivan EXAM BMarilia Farensena100% (1)
- NEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistDocument12 pagesNEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistMemer-alasadNo ratings yet
- Neuro Vital SignsDocument3 pagesNeuro Vital SignsKrissa Lei Pahang Razo100% (1)
- Neurological Exam Lecture NotesDocument26 pagesNeurological Exam Lecture NotesNaveen KovalNo ratings yet
- (Antoine Panaioti) Nietzsche and Buddhist PhilosopDocument259 pages(Antoine Panaioti) Nietzsche and Buddhist PhilosopFernando Lastlil100% (1)
- Police Log July 4, 2016Document12 pagesPolice Log July 4, 2016MansfieldMAPoliceNo ratings yet
- Glasgow Coma ScaleDocument3 pagesGlasgow Coma ScaleLanie Reyes de Guzman0% (1)
- Calculation of GcsDocument5 pagesCalculation of GcsGerald Limo Arap ChebiiNo ratings yet
- Glasgow Coma Scale Zen2Document7 pagesGlasgow Coma Scale Zen2Zen Firhan ShahabNo ratings yet
- Glasgow Coma ScaleDocument4 pagesGlasgow Coma ScaleYunita ManurungNo ratings yet
- Glasgow Coma ScaleDocument4 pagesGlasgow Coma ScaleSajo KappanNo ratings yet
- Glasgow Coma ScaleDocument47 pagesGlasgow Coma ScaleTripti Pun100% (1)
- Gcs ScoringDocument8 pagesGcs ScoringMichael Ian ReditoNo ratings yet
- Physical Assessment - Specifics On General ObservationsDocument14 pagesPhysical Assessment - Specifics On General ObservationsJennifer B. GarciaNo ratings yet
- Glasgow Coma ScaleDocument22 pagesGlasgow Coma Scaleshabatat2002No ratings yet
- Assessment of The Nervous System - FinalDocument76 pagesAssessment of The Nervous System - FinalRona Lucido100% (1)
- Cengher Et Al, 2018Document20 pagesCengher Et Al, 2018GokushimakNo ratings yet
- PROMPT FADING CengherBuddFarrellFienup2017Document19 pagesPROMPT FADING CengherBuddFarrellFienup2017BárbaraLaureanoNo ratings yet
- Responsiveness PSFS Vs RMDQ - ESJ2010Document8 pagesResponsiveness PSFS Vs RMDQ - ESJ2010Ju ChangNo ratings yet
- Cengher, Kim & Fienup, 2020Document22 pagesCengher, Kim & Fienup, 2020GokushimakNo ratings yet
- The Detailed Neurologic Examination in AdultsDocument21 pagesThe Detailed Neurologic Examination in AdultsLuisa FernandaNo ratings yet
- Noman Ahmed 1811190630 EXP - ReportDocument9 pagesNoman Ahmed 1811190630 EXP - ReportNayeem Rumman Julhash 1911185642No ratings yet
- Aggression and NoncomplianceDocument13 pagesAggression and NoncomplianceYaisel MartinNo ratings yet
- GCSDocument3 pagesGCSStevani NovitaNo ratings yet
- The Detailed Neurological Examination in Adults PDFDocument30 pagesThe Detailed Neurological Examination in Adults PDFOkenabirhieNo ratings yet
- Long Quiz RegodosDocument4 pagesLong Quiz RegodosIan Cyrus RegodosNo ratings yet
- Neuro Vital Signs Assessment Procedure and ChecklistDocument9 pagesNeuro Vital Signs Assessment Procedure and ChecklistJustine BayabosNo ratings yet
- Sazzadul1621595Exp ReportDocument18 pagesSazzadul1621595Exp ReportAsrafia Mim 1813026630No ratings yet
- Samj F: Neurolinguisic Programming in The Medical ConsultationDocument2 pagesSamj F: Neurolinguisic Programming in The Medical ConsultationndjokbestNo ratings yet
- The Single Most Important AssessmentDocument7 pagesThe Single Most Important Assessmenthellfire222No ratings yet
- Lab Act 2 SensoryDocument5 pagesLab Act 2 SensoryZgama AbdulrahmanNo ratings yet
- Glasgow Coma Scale GCSDocument7 pagesGlasgow Coma Scale GCSSSNo ratings yet
- Mental Status ExaminationDocument10 pagesMental Status Examinationlatasha deshmukhNo ratings yet
- NEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistDocument12 pagesNEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistANA DelafuenteNo ratings yet
- Behavioral Models of Impulsivity in Relation To ADHD: Translation Between Clinical and Preclinical StudiesDocument17 pagesBehavioral Models of Impulsivity in Relation To ADHD: Translation Between Clinical and Preclinical StudiesJose EscobarNo ratings yet
- Chapter 3, 4 and 5 PsyechDocument96 pagesChapter 3, 4 and 5 Psyechfanos hinika100% (1)
- Systematic Observation in Clinical PsychologyDocument4 pagesSystematic Observation in Clinical PsychologyVaniladie AliaNo ratings yet
- Neurology 1 Standardised Assessment Checklists Kim Miller 2002Document7 pagesNeurology 1 Standardised Assessment Checklists Kim Miller 2002Pramuk Muk MahanamaNo ratings yet
- MMT RedefinedDocument14 pagesMMT RedefinedAllan MutiibwaNo ratings yet
- Description of The StrategyDocument7 pagesDescription of The Strategyiulia9gavrisNo ratings yet
- Using The Glasgow Coma Scale For Patient AssessmentDocument7 pagesUsing The Glasgow Coma Scale For Patient AssessmentJasmin Dela TorreNo ratings yet
- 6507 Assignment 2Document19 pages6507 Assignment 2Hollywood MoviesNo ratings yet
- Neuro Assessment: The Single Most Important AssessmentDocument10 pagesNeuro Assessment: The Single Most Important AssessmentpapadaadNo ratings yet
- Goal Planning and Neurorehabilitation: The Wolfson Neurorehabilitation Centre ApproachDocument13 pagesGoal Planning and Neurorehabilitation: The Wolfson Neurorehabilitation Centre ApproachMiguelySusy Ramos-RojasNo ratings yet
- Glasgow Coma Scale GCSDocument4 pagesGlasgow Coma Scale GCScardiacanesthesiaNo ratings yet
- Student Name:: Ayesha AdreesDocument20 pagesStudent Name:: Ayesha AdreesAyesha AishNo ratings yet
- Chapter 8Document30 pagesChapter 8Karla CarazoNo ratings yet
- Proprioception Assessment - 2022Document1 pageProprioception Assessment - 2022micaela coetzeeNo ratings yet
- B. Learning TheoriesDocument71 pagesB. Learning TheorieschristianarcigaixNo ratings yet
- Comparing Skill Acquisition Under Varying Onsets of DifferentialDocument20 pagesComparing Skill Acquisition Under Varying Onsets of DifferentialElse12No ratings yet
- Psych 314 TermsDocument5 pagesPsych 314 TermsJoseph LiuNo ratings yet
- Monitoring and Recording Patients Neurological ObservationsDocument7 pagesMonitoring and Recording Patients Neurological Observationsyen2xxNo ratings yet
- Chapter 22Document9 pagesChapter 22Jenna SolomonNo ratings yet
- Behaviour and Cognitive Therapies Assignment 1: Vanshika Garg Maclp 4B (148) Respondent (Document14 pagesBehaviour and Cognitive Therapies Assignment 1: Vanshika Garg Maclp 4B (148) Respondent (veryNo ratings yet
- SGRQ Manual March 2022Document14 pagesSGRQ Manual March 2022LiAnna LiAnnaNo ratings yet
- The Detailed Neurologic Examination in Adults - UpToDateDocument41 pagesThe Detailed Neurologic Examination in Adults - UpToDateLucero ContrerasNo ratings yet
- Brain Injury Paper 2004Document16 pagesBrain Injury Paper 2004pamagu80No ratings yet
- Neurological AssessmentDocument61 pagesNeurological AssessmentSamantha SunglaoNo ratings yet
- Class: 4-C of Nursing Aprillia Nurul (201502082) Destiana P. (201502086)Document12 pagesClass: 4-C of Nursing Aprillia Nurul (201502082) Destiana P. (201502086)APRILIA NURULNo ratings yet
- Detailed Neurologic Examination in Adults - UpToDateDocument34 pagesDetailed Neurologic Examination in Adults - UpToDatejrneurology2014No ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- 2019 JC2 H2 Physics Anderson Serangoon Junior CollegeDocument90 pages2019 JC2 H2 Physics Anderson Serangoon Junior Collegeeternal vorceNo ratings yet
- 10.4 Diagnostic Based in Vibrations AnalysisDocument35 pages10.4 Diagnostic Based in Vibrations AnalysisgabrielNo ratings yet
- 36 - 4 - New York - 08-91 - 1478Document8 pages36 - 4 - New York - 08-91 - 1478Ovo OjasNo ratings yet
- M8 Sensor UGuide 96-00001 REV H 073117Document50 pagesM8 Sensor UGuide 96-00001 REV H 073117Ashish KundapurNo ratings yet
- PROGRAMA DE INGLES 11°jeDocument14 pagesPROGRAMA DE INGLES 11°jeJoséNo ratings yet
- User's ManualDocument42 pagesUser's ManualSupriya ManojNo ratings yet
- Seal of History Our Inheritance in The Great Seal of USDocument207 pagesSeal of History Our Inheritance in The Great Seal of USAlfred E. NewmanNo ratings yet
- IET Biometrics - 2022 - Sun - Breast Mass Classification Based On Supervised Contrastive Learning and Multi ViewDocument13 pagesIET Biometrics - 2022 - Sun - Breast Mass Classification Based On Supervised Contrastive Learning and Multi ViewMaha MasNo ratings yet
- Zero Gravity Chairs - ErgoQuest Zero Gravity Chairs and WorkstationsDocument6 pagesZero Gravity Chairs - ErgoQuest Zero Gravity Chairs and Workstationsnitouch3564No ratings yet
- Bodie Investments 12e IM CH27Document3 pagesBodie Investments 12e IM CH27lexon_kbNo ratings yet
- Definition of The CaribbeanDocument2 pagesDefinition of The CaribbeanBrianna AllenNo ratings yet
- Warrant: Catherine Lynn JarveyDocument4 pagesWarrant: Catherine Lynn JarveyLeigh EganNo ratings yet
- 'RAUP IOM-Aug06Document35 pages'RAUP IOM-Aug06Ngô Khắc ToảnNo ratings yet
- C10 CBSEPhy QueDocument4 pagesC10 CBSEPhy QueGeneric nameNo ratings yet
- XXDocument9 pagesXXAnjanasbagapur AnjanaNo ratings yet
- NANO-REX Lubricant AdditiveDocument8 pagesNANO-REX Lubricant AdditiveProject Sales CorpNo ratings yet
- ICC300 Cabinet Datasheet V01 20130609Document1 pageICC300 Cabinet Datasheet V01 20130609Krishna ManandharNo ratings yet
- Precos Souza CruzDocument12 pagesPrecos Souza CruzPablo ToazzaNo ratings yet
- DT 900 Pro X: FeaturesDocument1 pageDT 900 Pro X: FeaturestristonNo ratings yet
- SWP 04 Lifting OperationDocument4 pagesSWP 04 Lifting Operationমমিন মানবNo ratings yet
- Quiz - Lab Safety and ApparatusDocument1 pageQuiz - Lab Safety and ApparatusJohn Kristoffer RoblezaNo ratings yet
- Led Music Controller InsructionsDocument2 pagesLed Music Controller InsructionsArnaldoloNo ratings yet
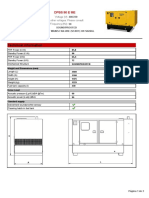
- Technical Information: Dpbs 90 E MeDocument3 pagesTechnical Information: Dpbs 90 E MeЛулу ТраедNo ratings yet
- WEF DibiDocument130 pagesWEF DibimanuelNo ratings yet
- Abe 424 Farm Structures and Environmental ControlDocument42 pagesAbe 424 Farm Structures and Environmental ControlAmabi SilasNo ratings yet
- JKSSB Class IV (28 Feb 2021) EnglishDocument12 pagesJKSSB Class IV (28 Feb 2021) Englishmirziya711No ratings yet
- PPC Researched PointersDocument4 pagesPPC Researched PointershitmonNo ratings yet
- Very-Low-Speed Variable-Structure Control of Sensor Less Axial Flux Permanent Magnet Synchronous Motor Using An Advanced Rotor Flux ConceptDocument9 pagesVery-Low-Speed Variable-Structure Control of Sensor Less Axial Flux Permanent Magnet Synchronous Motor Using An Advanced Rotor Flux ConceptDEBARATI DAMNo ratings yet