Download as pdf or txt
You might also like
- Shortness of Breath: Checklist PMPF Checklist PMPFDocument1 pageShortness of Breath: Checklist PMPF Checklist PMPFanz_4191No ratings yet
- Varicose Case ProformaDocument2 pagesVaricose Case ProformaSneha Naulakha100% (1)
- Preoperative and Postoperative CareDocument13 pagesPreoperative and Postoperative Carefaithfabulous1_06100% (1)
- ParacentesisDocument18 pagesParacentesistsnim saadNo ratings yet
- Inp IV TherapyDocument7 pagesInp IV TherapyCorpus, Irene Zen P.No ratings yet
- Minimizing Bleeding: Late SignDocument12 pagesMinimizing Bleeding: Late SignMatth N. ErejerNo ratings yet
- Kidney 112ADocument3 pagesKidney 112ARalph Elvin MacanlalayNo ratings yet
- Respiratory Term 2Document13 pagesRespiratory Term 2Abegail QuintoNo ratings yet
- Iv TherapyDocument11 pagesIv TherapyMarinill SolimanNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiNo ratings yet
- NGT Nasogastric Tube Key Points: IndicationsDocument7 pagesNGT Nasogastric Tube Key Points: IndicationsHana ChanNo ratings yet
- Femoral EmbolectomyDocument13 pagesFemoral EmbolectomyAndrea Aji SanayaNo ratings yet
- Topic 2 - Blood CollectionDocument12 pagesTopic 2 - Blood CollectionKatelyn Muñoz FlorNo ratings yet
- Wardclasspptbt 120819085632 Phpapp01Document26 pagesWardclasspptbt 120819085632 Phpapp01Ryan-Jay AbolenciaNo ratings yet
- Kuliah EmergensiDocument66 pagesKuliah EmergensiRifqi RamdhaniNo ratings yet
- PVD and Hematologic Disorders.Document9 pagesPVD and Hematologic Disorders.nycaNo ratings yet
- Aubf Lec Week 15Document7 pagesAubf Lec Week 15Joanne RemolloNo ratings yet
- NCP HemothoraxDocument3 pagesNCP Hemothoraxroseonabreeze0% (2)
- Emergency Procedures Masterclass: Siamak Moayedi, MDDocument23 pagesEmergency Procedures Masterclass: Siamak Moayedi, MDCoding NinjaNo ratings yet
- Nursing Care of Patient On Dialysis 10Document17 pagesNursing Care of Patient On Dialysis 10Suji MerlineNo ratings yet
- Nursing Care Plan For DM PatientDocument10 pagesNursing Care Plan For DM PatientRainier Rhett Concha100% (5)
- 01 Pleural DiseasesDocument6 pages01 Pleural DiseasesahmedNo ratings yet
- Prelims - GMJ SL - Module 1 Fluids & Electrolytes: Lactated Ringers, D5 Water, Plain Normal SalineDocument3 pagesPrelims - GMJ SL - Module 1 Fluids & Electrolytes: Lactated Ringers, D5 Water, Plain Normal SalinejuiceNo ratings yet
- ATI Fluids, AcidBase, DietsDocument9 pagesATI Fluids, AcidBase, DietsBernardo AntonioNo ratings yet
- NCM 112 Finals Lab 2022Document14 pagesNCM 112 Finals Lab 2022micaelaborja24No ratings yet
- Blood Transfusion: 42 Days. Five DaysDocument5 pagesBlood Transfusion: 42 Days. Five DayskatsukagemaruNo ratings yet
- Parasitology - Finals LABDocument23 pagesParasitology - Finals LABjeffrey100% (1)
- Halo FemoralDocument3 pagesHalo FemoralJhiLy 사랑의 케빈 우No ratings yet
- Chest Tubes: Reason For UseDocument15 pagesChest Tubes: Reason For UseJack Keurig67% (3)
- Deiparine, Cyenel Nicole - Chap9Document5 pagesDeiparine, Cyenel Nicole - Chap9Cyenel DeiparineNo ratings yet
- DIALYSISDocument21 pagesDIALYSISEadrian ReyesNo ratings yet
- Varicose Veins-1Document39 pagesVaricose Veins-1Shruti KandulaNo ratings yet
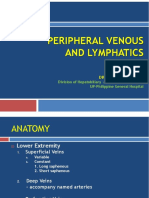
- Peripheral Venous and LymphaticsDocument34 pagesPeripheral Venous and LymphaticsRea Dominique CabanillaNo ratings yet
- What Is Colonoscopy?Document4 pagesWhat Is Colonoscopy?Angel DamoNo ratings yet
- Vascular SystemDocument33 pagesVascular SystemCarl Elexer Cuyugan Ano100% (3)
- Pathophysiology: Risk FactorsDocument4 pagesPathophysiology: Risk FactorsEdson John DemayoNo ratings yet
- Transfusion ReactionsDocument1 pageTransfusion ReactionsAc Karl Aquino TañedoNo ratings yet
- Blood CollectionDocument3 pagesBlood CollectionMary Joy HersaliaNo ratings yet
- DROWNING (Doc A)Document4 pagesDROWNING (Doc A)gayleteguichan19No ratings yet
- Renal Replacement TherapyDocument11 pagesRenal Replacement TherapyZahra AlaradiNo ratings yet
- Fluid and ElectrolytesDocument21 pagesFluid and ElectrolytesKc Cabanilla LizardoNo ratings yet
- AneurysmDocument3 pagesAneurysmMa. Aira Jean PedroNo ratings yet
- Hemolytic Transfusion ReactionDocument3 pagesHemolytic Transfusion ReactionAinin SofiyaNo ratings yet
- Reviewer RenalDocument13 pagesReviewer Renalsean blaze100% (1)
- Piles ManagementDocument68 pagesPiles ManagementDrAkhand Pratap Singh Baghel100% (2)
- Cardiovascular Dysfuntion Version 2Document10 pagesCardiovascular Dysfuntion Version 2Jhasseryne Orias SanchezNo ratings yet
- Demonstration ON Haemodialysis: Submitted ToDocument46 pagesDemonstration ON Haemodialysis: Submitted ToAbirajanNo ratings yet
- Oral Surgery 4 PDFDocument149 pagesOral Surgery 4 PDFZARI DANIELLE TORRESNo ratings yet
- Assessment Diagnosis Planning Intervention-Rationale Evaluation Fluid Volume Excess Related ToDocument3 pagesAssessment Diagnosis Planning Intervention-Rationale Evaluation Fluid Volume Excess Related ToJen BallesterosNo ratings yet
- AscitesDocument5 pagesAscitesmohamed mowafeyNo ratings yet
- 4.3 LP 5 Hypovolemic Shock - PPSXDocument40 pages4.3 LP 5 Hypovolemic Shock - PPSXCamelia A. ParuschiNo ratings yet
- DVT & Varicose VeinsDocument30 pagesDVT & Varicose VeinsMargaret Xaira Rubio MercadoNo ratings yet
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDocument4 pagesAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- MCN PihDocument4 pagesMCN PihBSN 1-N CASTRO, RicciNo ratings yet
- Presentation 25Document12 pagesPresentation 25K v Ranga saiNo ratings yet
- Pre-Analytical Consideration in PhlebotomyDocument3 pagesPre-Analytical Consideration in PhlebotomyJacinta Malamion100% (1)
- Assisting in Intravenous InfusionDocument4 pagesAssisting in Intravenous InfusionEloise Pateño33% (3)
- Unit 1 AnswerDocument22 pagesUnit 1 Answerii Dr3slNo ratings yet
- Etextbook For Principles of Anatomy and Physiology 2Nd Asia Pacific Edition Full Chapter PDFDocument53 pagesEtextbook For Principles of Anatomy and Physiology 2Nd Asia Pacific Edition Full Chapter PDFchanndmoz100% (5)
- Complications of Myocardial InfarctionDocument50 pagesComplications of Myocardial InfarctionAli Baker Algelane50% (2)
- Early Embryology Week OneDocument14 pagesEarly Embryology Week OnelukesqueNo ratings yet
- Krok 1 - 2015 (Physiology)Document28 pagesKrok 1 - 2015 (Physiology)mayna ynaNo ratings yet
- A Case Study On The Concept of OxygenationDocument4 pagesA Case Study On The Concept of OxygenationCecil Bhang-i Cacay - PabloNo ratings yet
- Gastrointestinal System: Chapter EighteenDocument32 pagesGastrointestinal System: Chapter Eighteenhayascent hilarioNo ratings yet
- Exercise in DiabetesDocument77 pagesExercise in DiabetesAkshay BangadNo ratings yet
- CABGDocument41 pagesCABGJasmin Jacob100% (2)
- Anaesthetic Concern For One Lung Ventilation: By-Dr - Bhushan Kinge, M.D. Ims - Bhu, VaranasiDocument57 pagesAnaesthetic Concern For One Lung Ventilation: By-Dr - Bhushan Kinge, M.D. Ims - Bhu, VaranasifaisalnaseemkhanNo ratings yet
- Procedural Sedation and AnalgesiaDocument30 pagesProcedural Sedation and AnalgesiashoibyNo ratings yet
- Asphyxial DeathDocument9 pagesAsphyxial DeathBismah TariqNo ratings yet
- Distal LM TrifurcationDocument62 pagesDistal LM TrifurcationSebastian ChandraNo ratings yet
- Evaluation of Segmental Myocardial Work in The Left VentricleDocument4 pagesEvaluation of Segmental Myocardial Work in The Left Ventricleme1921No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
- Ses 12 Principles of Newborn Adaption To The Extra-Uterine LifeDocument25 pagesSes 12 Principles of Newborn Adaption To The Extra-Uterine Lifelandegre KNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- Biology Paper 3 TZ2 HLDocument13 pagesBiology Paper 3 TZ2 HL56ch5k5p7nNo ratings yet
- Diabetes Algorithm Executive SummaryDocument30 pagesDiabetes Algorithm Executive SummaryLuis Alberto Alvarez AnkassNo ratings yet
- GL236 DM Guideline Moh enDocument38 pagesGL236 DM Guideline Moh enLa Minor ChannelNo ratings yet
- SOAL NO BaruDocument16 pagesSOAL NO Barukautsar abiyogaNo ratings yet
- Thoracic WallDocument12 pagesThoracic WallZainab NaffeeNo ratings yet
- Tube FeedingDocument34 pagesTube FeedingHalima IliyasuNo ratings yet
- Health Equipments 2018Document109 pagesHealth Equipments 2018Rajat Agarwal100% (1)
- PA - Coursepack DAY 1Document352 pagesPA - Coursepack DAY 1Elly NuñezNo ratings yet
- Case Studies On Cardiovascular DiseasesDocument43 pagesCase Studies On Cardiovascular DiseasesClarise Barcenal BrionesNo ratings yet
- Textbook Surgery of The Inferior Vena Cava A Multidisciplinary Approach 1St Edition Daniel Azoulay Ebook All Chapter PDFDocument53 pagesTextbook Surgery of The Inferior Vena Cava A Multidisciplinary Approach 1St Edition Daniel Azoulay Ebook All Chapter PDFisabel.simpon861100% (4)
- Chronic Adolescent Marijuana Use As A Risk Factor For Physical and Mental Health Problems in Young Adult MenDocument14 pagesChronic Adolescent Marijuana Use As A Risk Factor For Physical and Mental Health Problems in Young Adult MenLeonardo Esteban Lizama OrdenesNo ratings yet
- Lutembacher's Syndrome - A Case ReportDocument2 pagesLutembacher's Syndrome - A Case ReportInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet