Download as pdf or txt
You might also like
- 194 Renal Replacement Therapy in Critical Care PDFDocument15 pages194 Renal Replacement Therapy in Critical Care PDFAndreeaIrinaHedes100% (1)
- Drug Study - NitroglycerinDocument2 pagesDrug Study - NitroglycerinKian Herrera100% (1)
- Paediatric Tolosa-Hunt Syndrome: The Need For Treatment Guidelines and Renewed CriteriaDocument2 pagesPaediatric Tolosa-Hunt Syndrome: The Need For Treatment Guidelines and Renewed CriteriaRakasiwi GalihNo ratings yet
- Relieving Symptoms of Meralgia Paresthetica Using Kinesio Taping - A Pilot StudyDocument3 pagesRelieving Symptoms of Meralgia Paresthetica Using Kinesio Taping - A Pilot StudyAdam MorrellNo ratings yet
- 10 17826-Cutf 203634-206098Document4 pages10 17826-Cutf 203634-206098alaawagdybv2No ratings yet
- A08d PDFDocument3 pagesA08d PDFok okNo ratings yet
- Torj 12 125Document4 pagesTorj 12 125Tya VenyNo ratings yet
- The Short-Term Efficacy of Laser Brace ADocument6 pagesThe Short-Term Efficacy of Laser Brace AHevin GokulNo ratings yet
- Paper 5Document8 pagesPaper 5Francisco Javier Luza RamosNo ratings yet
- Association of Myasthenia Gravis and Behçet's Disease: A CaseDocument4 pagesAssociation of Myasthenia Gravis and Behçet's Disease: A CaseTrần Văn ĐệNo ratings yet
- Pan 1Document3 pagesPan 1Mithun CbNo ratings yet
- Article 8Document4 pagesArticle 8umair muqriNo ratings yet
- 8Document1 page8Daniel GuevaraNo ratings yet
- Jms 21041483Document28 pagesJms 21041483Afra Eslis NoatoNo ratings yet
- Stadhouder PDFDocument7 pagesStadhouder PDFPramod N KNo ratings yet
- CaseDocument1 pageCasemuhammad rezaNo ratings yet
- BETPresentation DiabeticAmyotrophy (08!02!13)Document10 pagesBETPresentation DiabeticAmyotrophy (08!02!13)Nigel SparksNo ratings yet
- Kyphoplasty For Vertebral Augmentation in The Elderly With Osteoporotic Vertebral Compression Fractures: Scenarios and Review of Recent StudiesDocument8 pagesKyphoplasty For Vertebral Augmentation in The Elderly With Osteoporotic Vertebral Compression Fractures: Scenarios and Review of Recent StudiesnuwaboyNo ratings yet
- EpicondilteDocument7 pagesEpicondilteRicardo fariaNo ratings yet
- Short Term Efficacy of LLLT in Knee OA RBO 2011 InglDocument8 pagesShort Term Efficacy of LLLT in Knee OA RBO 2011 InglMichele GonçalvesNo ratings yet
- Acompanhamento de HD Por Tto ConservadorDocument7 pagesAcompanhamento de HD Por Tto ConservadorOctavio HoraNo ratings yet
- The Neurology of Eclampsia: Some Observations: Views and ReviewsDocument8 pagesThe Neurology of Eclampsia: Some Observations: Views and ReviewsFajar Rudy QimindraNo ratings yet
- Can Electromyography PredictDocument4 pagesCan Electromyography PredictLupita Sánchez PradoNo ratings yet
- Nonoperative or Surgical Treatment of Acute Achille's Tendon Rupture NEJM 2022Document12 pagesNonoperative or Surgical Treatment of Acute Achille's Tendon Rupture NEJM 2022Americo BarbosaNo ratings yet
- Nejm Achiles Surgery Vs NonDocument12 pagesNejm Achiles Surgery Vs NonShandy MahardikaNo ratings yet
- 1 s2.0 S1877065714004072 MainDocument1 page1 s2.0 S1877065714004072 MainGabriel Humberto Vásquez HerreraNo ratings yet
- 2503 6018 1 PBDocument10 pages2503 6018 1 PBFedericó SchëlzerNo ratings yet
- Editorial: ReferencesDocument5 pagesEditorial: ReferencesRekha RekzNo ratings yet
- Traning Schedule 2018Document5 pagesTraning Schedule 2018alvaedison00No ratings yet
- Vertebroplastia Evidencia 1 USADocument11 pagesVertebroplastia Evidencia 1 USAandres donnetNo ratings yet
- Idiopathic Anterior Interosseous Nerve Dysfunction: The PatientDocument2 pagesIdiopathic Anterior Interosseous Nerve Dysfunction: The Patientyahoozyswk1016No ratings yet
- Transforaminal Debridement With A Posterior Only.62Document6 pagesTransforaminal Debridement With A Posterior Only.62Jean Marcel Castelo VegaNo ratings yet
- E Vectiveness of Exercise in Patients With Osteoarthritis of Hip or Knee: Nine Months' Follow UpDocument8 pagesE Vectiveness of Exercise in Patients With Osteoarthritis of Hip or Knee: Nine Months' Follow UpRatih dwi rahmawatiNo ratings yet
- Survival in Nonocclusive Mesenteric IschemiaDocument7 pagesSurvival in Nonocclusive Mesenteric IschemiaArun JoyNo ratings yet
- Ultrasound Therapy CTADocument5 pagesUltrasound Therapy CTAmitchNo ratings yet
- Herniated Lumbar Intervertebral DiskDocument10 pagesHerniated Lumbar Intervertebral DiskRoberto López MataNo ratings yet
- 10 1179@0886963413z 0000000002Document7 pages10 1179@0886963413z 0000000002hilderhNo ratings yet
- DOR - FENOL - Chemical Ablation of Genicular Nerve With Phenol For Pain Relief in Patients With Knee Osteoarthritis A Prospective Study - CompressedDocument7 pagesDOR - FENOL - Chemical Ablation of Genicular Nerve With Phenol For Pain Relief in Patients With Knee Osteoarthritis A Prospective Study - CompressedGustavo FredericoNo ratings yet
- 2013 Knee Prolotherapy RCTDocument9 pages2013 Knee Prolotherapy RCTReyn JohnsonNo ratings yet
- ArchRheumatol 33 418Document6 pagesArchRheumatol 33 418qwerty hrNo ratings yet
- 19 - Capítulo 4.2 - 2-Zhang e Colaboradores 2022Document13 pages19 - Capítulo 4.2 - 2-Zhang e Colaboradores 2022CharleneNo ratings yet
- D Aso 81-86Document7 pagesD Aso 81-86Academecian groupNo ratings yet
- Osteoporoza Tranzitorie Vs AVNDocument6 pagesOsteoporoza Tranzitorie Vs AVNVlad RakoczyNo ratings yet
- 71a, Woman, Low Back PainDocument4 pages71a, Woman, Low Back PainGabriel MouraNo ratings yet
- Commentary: The Optic Neuritis Treatment TrialDocument2 pagesCommentary: The Optic Neuritis Treatment TrialEmmanuel Zótico Orellana JiménezNo ratings yet
- Ilter 2015Document8 pagesIlter 2015Ahmad Awaludin TaslimNo ratings yet
- Piriformis Syndrome Long-Term Follow-Up in Patients Treated With Percutaneous Injection of Anesthetic and Corticosteroid Under CT GuidanceDocument8 pagesPiriformis Syndrome Long-Term Follow-Up in Patients Treated With Percutaneous Injection of Anesthetic and Corticosteroid Under CT GuidanceJessica EscobarNo ratings yet
- FRIDMAN - Achilles - Tendinopathies PDFDocument3 pagesFRIDMAN - Achilles - Tendinopathies PDFadalberto torrealbaNo ratings yet
- Magnetic Field Osteitis PubisDocument4 pagesMagnetic Field Osteitis PubisPeter DunnNo ratings yet
- Tens HNPDocument6 pagesTens HNPUniquaNo ratings yet
- Clinical StudyDocument8 pagesClinical Studylilis pratiwiNo ratings yet
- Debilidad Neuromuscular Adquirida y Movilizacion Temprana en UTIDocument14 pagesDebilidad Neuromuscular Adquirida y Movilizacion Temprana en UTILucho FelicevichNo ratings yet
- The Diagnosis and Treatment of The Cervical VertigoDocument5 pagesThe Diagnosis and Treatment of The Cervical VertigoDjumadi AkbarNo ratings yet
- APS Therapy Research DocumentsDocument60 pagesAPS Therapy Research Documentsherbs6No ratings yet
- 2014 - Auricular Acupressure Helps Improve Sleep Quality For Severe Insomnia in Maintenance Hemodialysis Patients A Pilot StudyDocument8 pages2014 - Auricular Acupressure Helps Improve Sleep Quality For Severe Insomnia in Maintenance Hemodialysis Patients A Pilot StudyJoão PauloNo ratings yet
- 1 s2.0 S0003999319303892 MainDocument8 pages1 s2.0 S0003999319303892 MainRizkyrafiqoh afdinNo ratings yet
- PNF Ombro 04Document10 pagesPNF Ombro 04Isaias AlmeidaNo ratings yet
- Bertolotti's SyndromeDocument14 pagesBertolotti's SyndromeSanjeev Pal YadavNo ratings yet
- Jurnal 8 PDFDocument7 pagesJurnal 8 PDFAmorrita Puspita RatuNo ratings yet
- Buck Reapir EPLDocument7 pagesBuck Reapir EPLMacaGumucioNo ratings yet
- US GastricDocument4 pagesUS Gastrictomlawson88No ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Mifepristone Polymorph With Enhanced Solubility, Dissolution and Oral BioavailabilityDocument7 pagesMifepristone Polymorph With Enhanced Solubility, Dissolution and Oral BioavailabilityStefania ArdeleanuNo ratings yet
- Literature Review of Momordica CharantiaDocument7 pagesLiterature Review of Momordica Charantiavvomvqwgf100% (1)
- Establishing The Onset of Action of Intranasal CorticosteroidsDocument10 pagesEstablishing The Onset of Action of Intranasal CorticosteroidsKevin de KievNo ratings yet
- BMJ k1950 FullDocument6 pagesBMJ k1950 FullMUHAMMAD09No ratings yet
- Neurobiologic Causes of Mental Illness and PsychopharmacologyDocument64 pagesNeurobiologic Causes of Mental Illness and PsychopharmacologymikaelairisaizonNo ratings yet
- LoperamidaDocument19 pagesLoperamidaGlo RyndaNo ratings yet
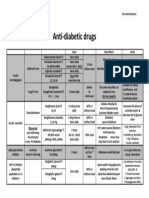
- Anti Diabetic DrugsDocument1 pageAnti Diabetic DrugsWael hadNo ratings yet
- Understanding The Disease of AddictionDocument7 pagesUnderstanding The Disease of AddictionJoão MaiaNo ratings yet
- Gondar, EthiopiaDocument27 pagesGondar, Ethiopianegussie birieNo ratings yet
- Low Flow AnesthesiaDocument92 pagesLow Flow Anesthesiaeliezer_89100% (1)
- Ref 12Document12 pagesRef 12Tiago BaraNo ratings yet
- Kitty MagicDocument3 pagesKitty MagicIordana StoicaNo ratings yet
- DA (SA) Past - Papers 2020 1st SemesterDocument81 pagesDA (SA) Past - Papers 2020 1st SemesterYudhika NaidooNo ratings yet
- List of Look-Alike MedicationsDocument5 pagesList of Look-Alike MedicationsAhmad TaramsyNo ratings yet
- Cirrhosis NEJMDocument11 pagesCirrhosis NEJM張雅婷No ratings yet
- Case AKIDocument5 pagesCase AKIVivi DeviyanaNo ratings yet
- Niper Jee SyllabusDocument9 pagesNiper Jee SyllabusChaitanya PawarNo ratings yet
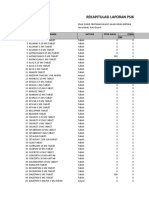
- Rekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFDocument9 pagesRekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFlarasNo ratings yet
- Open Access ToxCast/Tox21, Toxicological Priority Index (ToxPi) and Integrated Chemical Environment (ICE) Models Rank and Predict Acute Pesticide Toxicity: A Case StudyDocument24 pagesOpen Access ToxCast/Tox21, Toxicological Priority Index (ToxPi) and Integrated Chemical Environment (ICE) Models Rank and Predict Acute Pesticide Toxicity: A Case StudyPremier PublishersNo ratings yet
- Pharmaceutical Care PDFDocument3 pagesPharmaceutical Care PDFFersan AngelesNo ratings yet
- GlycosidesDocument124 pagesGlycosidesMooma fatimaNo ratings yet
- The Concept of Social PharmacyDocument3 pagesThe Concept of Social PharmacyAsmaa AbdelatyNo ratings yet
- Dr. Ni Made Indri - CC For Ovulation InductionDocument26 pagesDr. Ni Made Indri - CC For Ovulation InductionAPOTEK Sarah FarmaNo ratings yet
- NRNP 6635 Final Exam EditedDocument86 pagesNRNP 6635 Final Exam Editedkandiezein88No ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- COX-1 and COX-2 Inhibitory Activity in Extracts Prepared From Eucomis Species, With Further Reference To Extracts From E. Autumnalis AutumnalisDocument6 pagesCOX-1 and COX-2 Inhibitory Activity in Extracts Prepared From Eucomis Species, With Further Reference To Extracts From E. Autumnalis AutumnalisFatima RiveraNo ratings yet
- Daftar Keluar Obat Harian ExcelDocument5 pagesDaftar Keluar Obat Harian ExcelPutri MeutiaNo ratings yet
- Seizure ThresholdDocument5 pagesSeizure ThresholdannNo ratings yet