Download as pdf or txt
You might also like
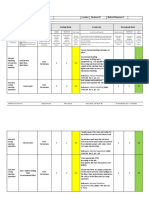
- Revised Risk Assessment-Concrete Coring-1Document5 pagesRevised Risk Assessment-Concrete Coring-1riyazkader83% (12)
- Evaluation of Change ProcessDocument12 pagesEvaluation of Change ProcessThe Hoopers100% (1)
- COURSE SYLLABUS P.E. Management Supervisory Practices in Physical EducationDocument3 pagesCOURSE SYLLABUS P.E. Management Supervisory Practices in Physical EducationRoger Salvador100% (4)
- The Impact of Therapeutic Community in The Perception of A Probationer in Quirino Province PhilippinesDocument5 pagesThe Impact of Therapeutic Community in The Perception of A Probationer in Quirino Province PhilippinesMelissa BubosNo ratings yet
- Legal Basis: Effectiveness of The Community-Based Rehabilitation Programs For Drug Surrenderees in Tacloban CityDocument9 pagesLegal Basis: Effectiveness of The Community-Based Rehabilitation Programs For Drug Surrenderees in Tacloban CityMateo BrazilNo ratings yet
- Health Eco AssignmentDocument41 pagesHealth Eco Assignmentregie cuaresmaNo ratings yet
- Literature Review-Racial DiscriminationDocument10 pagesLiterature Review-Racial Discriminationapi-31663638975% (4)
- Jurnal Canada 2Document9 pagesJurnal Canada 2Ikaputri fNo ratings yet
- SW450 Literature Review - Ashley SchultzDocument9 pagesSW450 Literature Review - Ashley Schultzashleyschultz12345No ratings yet
- Bridging The Care CascadeDocument13 pagesBridging The Care CascadePaul Karonji (Apollo)No ratings yet
- Addiction Research & TherapyDocument7 pagesAddiction Research & TherapyAlfredo MorenoNo ratings yet
- Care For Elderly PDFDocument10 pagesCare For Elderly PDFDzulfiqarNo ratings yet
- Health Social Care Comm - 2021 - Pedersen - Public Involvement in The Planning Development and Implementation of CommunityDocument27 pagesHealth Social Care Comm - 2021 - Pedersen - Public Involvement in The Planning Development and Implementation of Communitysri arnilasariNo ratings yet
- EJ1271926Document10 pagesEJ1271926iqra13866No ratings yet
- Grappling With Our Therapeutic Relationship and Professional Self Doubt During COVID 19 Will We Use Video Therapy AgainDocument13 pagesGrappling With Our Therapeutic Relationship and Professional Self Doubt During COVID 19 Will We Use Video Therapy AgainRo M OyarzúnNo ratings yet
- Experiences of Peer Workers and Mental Health Service Users With A Peer Support Intervention Applying and Critiquing A Behaviour Change TechniquesDocument12 pagesExperiences of Peer Workers and Mental Health Service Users With A Peer Support Intervention Applying and Critiquing A Behaviour Change TechniquesMariaLuanaNo ratings yet
- 12 Step GroupsDocument32 pages12 Step Groupsmichael rosaNo ratings yet
- Sozialforschung: Forum: Qualitative Social ResearchDocument32 pagesSozialforschung: Forum: Qualitative Social ResearchValeska OrellanaNo ratings yet
- Care Coordination PlanDocument6 pagesCare Coordination Planwalter1simonsNo ratings yet
- Journal of Substance Abuse Treatment: Lori J. Ducharme, PH.D., Redonna K. Chandler, PH.D., Alex H.S. Harris, PH.DDocument9 pagesJournal of Substance Abuse Treatment: Lori J. Ducharme, PH.D., Redonna K. Chandler, PH.D., Alex H.S. Harris, PH.DCorina IcaNo ratings yet
- Service InnovationDocument2 pagesService InnovationMae GamzNo ratings yet
- Promoting Mobile Health Adoption To Hospital Patients Through Social InfluencersDocument15 pagesPromoting Mobile Health Adoption To Hospital Patients Through Social InfluencersAli AhmedNo ratings yet
- Ding Et Al. - 2019 - Effect of Patient Participation On Nurse and Patient Outcomes in Inpatient HealthcareDocument16 pagesDing Et Al. - 2019 - Effect of Patient Participation On Nurse and Patient Outcomes in Inpatient Healthcare2208053044No ratings yet
- Therapeutic CommunitiesDocument15 pagesTherapeutic CommunitiesDanilo PerralNo ratings yet
- GAYDA PEDROSAasdDec 4Document32 pagesGAYDA PEDROSAasdDec 4Jude Ryan GaydaNo ratings yet
- Perceptions of Professionals Regarding Interventions Invol - 2021 - InternationaDocument10 pagesPerceptions of Professionals Regarding Interventions Invol - 2021 - InternationaenriggrNo ratings yet
- Hebert 2008 PDFDocument15 pagesHebert 2008 PDFAndrew GilbertNo ratings yet
- GILCHER e COLS, 2020 - The Strategies Are The Same, The Problems May Be Different" - A Qualitative Study Exploring The ExperiencesDocument11 pagesGILCHER e COLS, 2020 - The Strategies Are The Same, The Problems May Be Different" - A Qualitative Study Exploring The Experienceswellington contieroNo ratings yet
- Benchmarks For Outpatient Dialectical Behavioral Therapy in Adults With Borderline Personality DisorderDocument12 pagesBenchmarks For Outpatient Dialectical Behavioral Therapy in Adults With Borderline Personality DisorderAnna RodríguezNo ratings yet
- Nediskriminacija - RadDocument11 pagesNediskriminacija - RadivanNo ratings yet
- Maya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewDocument18 pagesMaya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewsukmarahastriNo ratings yet
- Art 20204135Document6 pagesArt 20204135John Francis Arellano BatohanonNo ratings yet
- 0rder 271 NRS-493 - PROFESSIONAL CAPSTONE & PRACTICUMDocument18 pages0rder 271 NRS-493 - PROFESSIONAL CAPSTONE & PRACTICUMjoshua chegeNo ratings yet
- Developing A Clinical Decision Support For Opioid Use Disorders: A NIDA Center For The Clinical Trials Network Working GroupDocument12 pagesDeveloping A Clinical Decision Support For Opioid Use Disorders: A NIDA Center For The Clinical Trials Network Working GroupivanNo ratings yet
- Substance AbuseDocument3 pagesSubstance AbusePrincess QumanNo ratings yet
- 1.6 JustificationDocument10 pages1.6 JustificationSakariyeFarooleNo ratings yet
- PA15 Case1Document1 pagePA15 Case1mariaalumawagNo ratings yet
- Pelayo, Shannel C.Document2 pagesPelayo, Shannel C.shannelpelayoNo ratings yet
- Managing Healthcare OrganisationsDocument16 pagesManaging Healthcare OrganisationsSamuel Josafat Olam100% (1)
- NGA Roadmap On MOUD For People in The Justice SystemDocument73 pagesNGA Roadmap On MOUD For People in The Justice Systemepraetorian100% (1)
- Consultorios Médicos en Farmacias PrivadasDocument12 pagesConsultorios Médicos en Farmacias PrivadasAristegui NoticiasNo ratings yet
- How Effective Are Social Norms Interventions in Changing The Clinical Behaviours of Healthcare Workers? A Systematic Review and Meta-AnalysisDocument19 pagesHow Effective Are Social Norms Interventions in Changing The Clinical Behaviours of Healthcare Workers? A Systematic Review and Meta-AnalysisSendhil RevuluriNo ratings yet
- Implementation of A Supervised Injection FacilityDocument13 pagesImplementation of A Supervised Injection FacilityjohnmorriscryptoNo ratings yet
- Building A Path To Sobriety Challenges and Strategies of Rehabilitation Workers in The Aftercare Process of Substance-Abuse IndividualsDocument9 pagesBuilding A Path To Sobriety Challenges and Strategies of Rehabilitation Workers in The Aftercare Process of Substance-Abuse IndividualsJournal of Interdisciplinary PerspectivesNo ratings yet
- Impact of Nursing Diagnoses On Patient and Organisational Outcomes: A Systematic Literature ReviewDocument43 pagesImpact of Nursing Diagnoses On Patient and Organisational Outcomes: A Systematic Literature ReviewLucas Teles IanniNo ratings yet
- Occupational Therapy's Value in Provision of Quality Care To Prevent ReadmissionsDocument9 pagesOccupational Therapy's Value in Provision of Quality Care To Prevent ReadmissionsMikeNo ratings yet
- Rémi Coignard-Friedman - Stine Hoj - Delivering Opioid Use Disorder - Abstract For Paris Contemporary Drug Problems ConferenceDocument1 pageRémi Coignard-Friedman - Stine Hoj - Delivering Opioid Use Disorder - Abstract For Paris Contemporary Drug Problems ConferenceRémi Coignard-FriedmanNo ratings yet
- Ohtas 13 33bDocument33 pagesOhtas 13 33bChristian MolimaNo ratings yet
- Reasearchchapter One To ThreeDocument32 pagesReasearchchapter One To ThreeEljay ManidlanganNo ratings yet
- Barier and EnablesDocument52 pagesBarier and EnablesAnonymous 8rsxG4No ratings yet
- Implementation of An Online Relatives ' Toolkit For Psychosis or Bipolar (Impart Study) : Iterative Multiple Case Study To Identify Key Factors Impacting On Staff Uptake and UseDocument13 pagesImplementation of An Online Relatives ' Toolkit For Psychosis or Bipolar (Impart Study) : Iterative Multiple Case Study To Identify Key Factors Impacting On Staff Uptake and UseLau DíazNo ratings yet
- Arden University: BA (Hons) Health Care ManagementDocument10 pagesArden University: BA (Hons) Health Care ManagementArslan JoiyaNo ratings yet
- Social Worker in Substance AbuseDocument40 pagesSocial Worker in Substance AbuseAmit Kumar100% (2)
- Rapid PEER Study To Strengthen The Injecting Drug Users' Quality of Life ProgrammeDocument88 pagesRapid PEER Study To Strengthen The Injecting Drug Users' Quality of Life ProgrammePascal TanguayNo ratings yet
- Need Assessment - EditedDocument5 pagesNeed Assessment - Editedidealexperts01No ratings yet
- HasanuzzamanDocument11 pagesHasanuzzamanSultan PasolleNo ratings yet
- WorkDocument7 pagesWorkDominic NkumNo ratings yet
- Experiences and Narratives Drug Users With Antisocial Personality Disorder Retelling The Process of Treatment and ChangeDocument9 pagesExperiences and Narratives Drug Users With Antisocial Personality Disorder Retelling The Process of Treatment and Changedoriszhang2014auNo ratings yet
- Couns and Psychother Res - 2021 - Hanley - Researching Online Counselling and Psychotherapy The Past The Present and TheDocument5 pagesCouns and Psychother Res - 2021 - Hanley - Researching Online Counselling and Psychotherapy The Past The Present and TheDasha GatchalianNo ratings yet
- 277 832 1 PBDocument7 pages277 832 1 PBeliska rahimNo ratings yet
- Jurnal STIKUDocument8 pagesJurnal STIKUHilmanNo ratings yet
- Marshall 2018Document18 pagesMarshall 2018Stella GašparušNo ratings yet
- Disclosure Project PaperDocument8 pagesDisclosure Project PapernazzalinhtinhNo ratings yet
- Indo Petroleum Nurse Grade II AdvertisementDocument4 pagesIndo Petroleum Nurse Grade II AdvertisementjaideepsdNo ratings yet
- RA 10354, Also Known As "The Responsible Parenthood and Reproductive Health Act of 2012", HasDocument9 pagesRA 10354, Also Known As "The Responsible Parenthood and Reproductive Health Act of 2012", HascianNo ratings yet
- Women Studies - 20.08.2020Document26 pagesWomen Studies - 20.08.2020Nargis NajumuNo ratings yet
- Penology Reviewer QuestionnaireDocument35 pagesPenology Reviewer QuestionnaireLowell De Los Reyes100% (1)
- PART 1: Interviews - 2.5 Mins (4 Points) : Top Notch3-SPEAKING QUESTIONS - SPRING 2021 - Part 2 A Face-To-Face ExamDocument2 pagesPART 1: Interviews - 2.5 Mins (4 Points) : Top Notch3-SPEAKING QUESTIONS - SPRING 2021 - Part 2 A Face-To-Face ExamHà PhươngNo ratings yet
- Performing Pain AssessmentDocument58 pagesPerforming Pain Assessmentjannaelemento11No ratings yet
- Task 3 Multiple Intelligence TheoryDocument11 pagesTask 3 Multiple Intelligence TheorySvetlanaNo ratings yet
- Topic 9 ObsDocument7 pagesTopic 9 ObsHannan SyedNo ratings yet
- V. B.A.,D.D.S. : Complete DenturesDocument10 pagesV. B.A.,D.D.S. : Complete DenturesbarbieNo ratings yet
- Biology ProjectDocument19 pagesBiology ProjectHussain Zohar0% (3)
- DRRR Q1 Module 4 08082020 - 5 1Document8 pagesDRRR Q1 Module 4 08082020 - 5 1donabypadida18No ratings yet
- Petunjuk Pengisian: Laporan Stock Dan Pemakaian Logistik MalariaDocument4 pagesPetunjuk Pengisian: Laporan Stock Dan Pemakaian Logistik MalariaMIN AZWAR UMAKAAPANo ratings yet
- FTC 1Document80 pagesFTC 1Alexis Tondo AlmadronesNo ratings yet
- HEALTH Q4 ReviewerDocument5 pagesHEALTH Q4 ReviewerAlma TatelNo ratings yet
- NCP Ineffective Breathing GunshotDocument3 pagesNCP Ineffective Breathing GunshotMikko Enoc100% (1)
- Population Dynamics and HealthDocument26 pagesPopulation Dynamics and HealthIsmail Andi BasoNo ratings yet
- HBN 25 LaundryDocument69 pagesHBN 25 LaundryMuhammad HarisNo ratings yet
- Agri 1 Presentation Calig&Canon - 20231018 - 174604 - 0000Document9 pagesAgri 1 Presentation Calig&Canon - 20231018 - 174604 - 0000gabrielcalig6No ratings yet
- Medical EthicsDocument25 pagesMedical Ethicsswarajudugade100% (1)
- How Do You Feel About Your BodyDocument21 pagesHow Do You Feel About Your BodyFabio VanuzziNo ratings yet
- Psych Law 2Document8 pagesPsych Law 2Aure, Joshua CaputolNo ratings yet
- Quiz1 KeyDocument8 pagesQuiz1 KeyAli KalyarNo ratings yet
- SO2ndEd PI Unit 6Document2 pagesSO2ndEd PI Unit 6Malek EmadNo ratings yet
- Project PresentationDocument9 pagesProject PresentationmurkNo ratings yet
- A Review of Torque Release Technique®Document5 pagesA Review of Torque Release Technique®Ed RibeiroNo ratings yet
- Zubair Marketing ListDocument18 pagesZubair Marketing ListsalesNo ratings yet