Download as pdf or txt
You might also like
- Calibration Procedure Crowcon Xgard Gas Detectors - 5720273 - 01Document16 pagesCalibration Procedure Crowcon Xgard Gas Detectors - 5720273 - 01Daniel Rolando Gutierrez FuentesNo ratings yet
- 1951 New York State Building CodeDocument292 pages1951 New York State Building Codekip2001No ratings yet
- Oxford Handbook of NeonatologyDocument575 pagesOxford Handbook of Neonatologybalyaibnu_690869145100% (5)
- ENDOMETRICS Root Canal Working Length DeterminationDocument51 pagesENDOMETRICS Root Canal Working Length DeterminationDhanavel Chakravarthy100% (1)
- Importance of Pat Ency in Endo Don TicsDocument8 pagesImportance of Pat Ency in Endo Don TicsMohammed OmoshNo ratings yet
- Anat of Root Apex - Review ArticleDocument9 pagesAnat of Root Apex - Review ArticleRevathy ParthasarathyNo ratings yet
- Importance of Patency in EndodonticsDocument8 pagesImportance of Patency in EndodonticsJAYASOORYAN S P M.D.S. CONSERVATIVE DENTISTRY AND ENDODONTICSNo ratings yet
- Significant of Apical Third: A ReviewDocument5 pagesSignificant of Apical Third: A ReviewJim Christover NiqNo ratings yet
- Digital Working Length in Endodontics - A ReviewDocument6 pagesDigital Working Length in Endodontics - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- EJMCM Volume 7 Issue 3 Pages 2086-2092Document7 pagesEJMCM Volume 7 Issue 3 Pages 2086-2092Mosab BabikirNo ratings yet
- Adts Guidelines For Access CavityDocument7 pagesAdts Guidelines For Access Cavityrojek63No ratings yet
- Working Length Determination of TeethDocument5 pagesWorking Length Determination of TeethMohammed Salih Al DolimeNo ratings yet
- Apical Limit 2009Document7 pagesApical Limit 2009wanda oktariaNo ratings yet
- Informe Endo 2Document7 pagesInforme Endo 2Angel LampreaNo ratings yet
- Adts Guidelines For Access CavityDocument9 pagesAdts Guidelines For Access CavityOmuraiNo ratings yet
- June 2007 CE2Document8 pagesJune 2007 CE2Faisal H RanaNo ratings yet
- Endodontic AccessDocument5 pagesEndodontic AccessShyambhavi SrivastavaNo ratings yet
- Working Length and Instrumentation: BY: Ahmed Abdulkhaliq Hiba Mahmood Zahraa Ali Ban AlaaDocument53 pagesWorking Length and Instrumentation: BY: Ahmed Abdulkhaliq Hiba Mahmood Zahraa Ali Ban AlaaahmedNo ratings yet
- Electronic Apex LocatorDocument13 pagesElectronic Apex LocatorEmilio CorderoNo ratings yet
- Ex Vivo Microbial Leakage Analysis of Polytetrafluoroethylene Tape and Cotton Pellet As Endodontic Access Cavity SpacersDocument7 pagesEx Vivo Microbial Leakage Analysis of Polytetrafluoroethylene Tape and Cotton Pellet As Endodontic Access Cavity SpacersAbhishek Isaac MathewNo ratings yet
- Antonis Chaniotis Doble CurvaturaDocument8 pagesAntonis Chaniotis Doble CurvaturaVitall Dent Endodoncia Odontologia integralNo ratings yet
- Determination of Working LengthDocument81 pagesDetermination of Working LengthANUBHA100% (2)
- 116 Guidelines For Access CavityDocument8 pages116 Guidelines For Access CavityYodha AdityaNo ratings yet
- JPediatrDent4251-3856361 104243Document4 pagesJPediatrDent4251-3856361 104243DrAditya BansalNo ratings yet
- Endodontic Managment of Curved CanalDocument3 pagesEndodontic Managment of Curved Canalfun timesNo ratings yet
- Endodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesDocument5 pagesEndodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Working Length DeterminationDocument56 pagesWorking Length DeterminationDrdrNo ratings yet
- Study of Endodontic Working Length of Korean Posterior TeethDocument7 pagesStudy of Endodontic Working Length of Korean Posterior TeethPavan TenglikarNo ratings yet
- Working LengthDocument67 pagesWorking LengthnishthaNo ratings yet
- WL DeterminationDocument12 pagesWL Determinationdr asiyaNo ratings yet
- Management of C Shaped CanalsDocument4 pagesManagement of C Shaped CanalsJot KhalsaNo ratings yet
- Apical Terminus Location of Root Canal Treatment ProceduresDocument5 pagesApical Terminus Location of Root Canal Treatment ProceduresbubuvulpeaNo ratings yet
- Endodontic Treatment of Mandibular Second Molar With Diversed Root Canal AnatomyDocument3 pagesEndodontic Treatment of Mandibular Second Molar With Diversed Root Canal AnatomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cleaning and Shaping: William T. Johnson D.D.S., M.S. W. Craig Noblett D.D.S., M.SDocument60 pagesCleaning and Shaping: William T. Johnson D.D.S., M.S. W. Craig Noblett D.D.S., M.SMonika LohakpureNo ratings yet
- A Tactile Method For Canal Length Determination in EndodonticsDocument3 pagesA Tactile Method For Canal Length Determination in EndodonticsdrtoothNo ratings yet
- Apical Foramen Morphology According To The Length of Merged Canal at The ApexDocument5 pagesApical Foramen Morphology According To The Length of Merged Canal at The Apexdany0001No ratings yet
- Apical Limit and Working Length in EndodonticsDocument6 pagesApical Limit and Working Length in EndodonticszaheerbdsNo ratings yet
- Detecting The Apical Constriction in Curved Mandibular Molars Roots - Preflared Vs Nonpreflared CANALSDocument4 pagesDetecting The Apical Constriction in Curved Mandibular Molars Roots - Preflared Vs Nonpreflared CANALSJoel Vázquez-BarrónNo ratings yet
- Management of Open ApexDocument7 pagesManagement of Open ApexMineet KaulNo ratings yet
- 5.wonderful World of Endodontic Working Width The Forgotten Dimension - A ReviewDocument7 pages5.wonderful World of Endodontic Working Width The Forgotten Dimension - A ReviewSiva Kumar100% (1)
- Comparison of Working Length Determination Using Apex Locator and Manual Method StudyDocument5 pagesComparison of Working Length Determination Using Apex Locator and Manual Method StudysaniaNo ratings yet
- DentHypotheses5384-434005 120320Document14 pagesDentHypotheses5384-434005 120320preethi.badamNo ratings yet
- 1.MB2 in Upperr Max 1st MolarDocument4 pages1.MB2 in Upperr Max 1st MolarSoham DattaNo ratings yet
- Ex Vivo Evaluation of The Ability of Four Different ElectronicDocument5 pagesEx Vivo Evaluation of The Ability of Four Different ElectronicJing XueNo ratings yet
- 10 1016@j Joen 2019 10 009Document8 pages10 1016@j Joen 2019 10 009fatimahNo ratings yet
- Applied Sciences: Plywood Jig-A New Technique For Root Canal Curvature MeasurementDocument8 pagesApplied Sciences: Plywood Jig-A New Technique For Root Canal Curvature MeasurementKarissa NavitaNo ratings yet
- Endodontics Modern Endodontic Principles Part 3: PreparationDocument10 pagesEndodontics Modern Endodontic Principles Part 3: Preparationiulian tigauNo ratings yet
- ANATOMIE 23RadixEntomolarispp87 90.20190614125011Document4 pagesANATOMIE 23RadixEntomolarispp87 90.20190614125011doctorlupuNo ratings yet
- Working WidthDocument4 pagesWorking WidthLira Wiet JayantiNo ratings yet
- Guide AccessDocument7 pagesGuide AccessDarianNo ratings yet
- Jurnal KasusDocument4 pagesJurnal KasusDena SeptianiNo ratings yet
- Contemporary Endodontic Obturation Techniques A Comprehensive Literature ReviewDocument8 pagesContemporary Endodontic Obturation Techniques A Comprehensive Literature ReviewMegha GhoshNo ratings yet
- Clinical Management of Endodontic CasesDocument91 pagesClinical Management of Endodontic CasesSharlene OngNo ratings yet
- Endodontic Management of Mandibular Third Molar With Radix EntomolarisDocument6 pagesEndodontic Management of Mandibular Third Molar With Radix EntomolarisismetNo ratings yet
- Determination of Working Length Lec. 7: Al-Mustansiriya University College of Dentistry Endodontics Lectures 4 YearDocument8 pagesDetermination of Working Length Lec. 7: Al-Mustansiriya University College of Dentistry Endodontics Lectures 4 YearSinggih HarsenoNo ratings yet
- Intricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewDocument10 pagesIntricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewManjeevNo ratings yet
- SaudiEndodJ 2019 9 2 140 255365Document6 pagesSaudiEndodJ 2019 9 2 140 255365rattih adeliaNo ratings yet
- Chaniotis Endodontic Practice UKDocument8 pagesChaniotis Endodontic Practice UKFebriani Seroja100% (1)
- Endo Pre FinalsDocument18 pagesEndo Pre FinalsRayne Gelle100% (2)
- Working Length Determination Technique For Determination Practical SessionsDocument60 pagesWorking Length Determination Technique For Determination Practical SessionsAtanaz DarvizehNo ratings yet
- Endodontic Treatment of Curved Root Canal Systems PDFDocument3 pagesEndodontic Treatment of Curved Root Canal Systems PDFRăican AlexandruNo ratings yet
- 20 Years of Guided Bone Regeneration in Implant Dentistry: Second EditionFrom Everand20 Years of Guided Bone Regeneration in Implant Dentistry: Second EditionNo ratings yet
- Complete Geography - REVISIONDocument48 pagesComplete Geography - REVISIONreyanshNo ratings yet
- Professor Jayashankar Telangana State Agricultural University Agricultural College, JagtialDocument17 pagesProfessor Jayashankar Telangana State Agricultural University Agricultural College, JagtialShivaji DarlingNo ratings yet
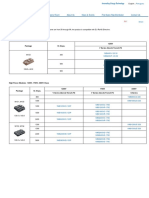
- IGBT Modules 1-Pack Fuji Electric AmericaDocument1 pageIGBT Modules 1-Pack Fuji Electric AmericaSergio MuriloNo ratings yet
- AL PREPARE Advance Directive EnglishDocument15 pagesAL PREPARE Advance Directive EnglishSNo ratings yet
- Borderline Personality Disorder: An Interview With Psychiatrist Dr. Roy KrawitzDocument8 pagesBorderline Personality Disorder: An Interview With Psychiatrist Dr. Roy KrawitzClinton PowerNo ratings yet
- Employment Law in OmanDocument3 pagesEmployment Law in OmanjuliechandruNo ratings yet
- Sika PDS E Plastomix - 705Document2 pagesSika PDS E Plastomix - 705lwin_oo2435No ratings yet
- SEC4 Overhead Conductors PDFDocument106 pagesSEC4 Overhead Conductors PDFKy TaNo ratings yet
- Water Supply SystemDocument52 pagesWater Supply Systemnyagabona goodluckNo ratings yet
- Kew Fdar1Document1 pageKew Fdar1Mariam JubelNo ratings yet
- Murder MemoDocument3 pagesMurder MemoRishika AgarwalNo ratings yet
- Activated Charcoal For Acute OverdoseDocument6 pagesActivated Charcoal For Acute OverdoseTony ChuNo ratings yet
- Assignment 1Document10 pagesAssignment 1Jae StainsbyNo ratings yet
- Banner Research 2018-1Document2 pagesBanner Research 2018-1Hilario Domingo ChicanoNo ratings yet
- Law of Tort NotesDocument7 pagesLaw of Tort NotesKarsin ManochaNo ratings yet
- Cement: N-W.F.P UET, Peshawar 1Document14 pagesCement: N-W.F.P UET, Peshawar 1Angelica Fontamillas SuicoNo ratings yet
- Gas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFDocument4 pagesGas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFsanjeevchhabraNo ratings yet
- A330 FactsDocument2 pagesA330 FactsGermanTobonNo ratings yet
- Curriculum Vitae: Muhammad SaqlainDocument2 pagesCurriculum Vitae: Muhammad SaqlainMuhammad AbbasNo ratings yet
- RPD Daily Incident Report 1/5/23Document5 pagesRPD Daily Incident Report 1/5/23inforumdocsNo ratings yet
- Faradic Type CurrentDocument26 pagesFaradic Type CurrentzainabnoorNo ratings yet
- Enabling Health and Healthcare Through IctDocument416 pagesEnabling Health and Healthcare Through Ictarif candrautamaNo ratings yet
- MAkati HAberdashery Inc Vs NLRCDocument6 pagesMAkati HAberdashery Inc Vs NLRCkc lovessNo ratings yet
- 11-An - Industrial Dehumidifier SizingDocument4 pages11-An - Industrial Dehumidifier Sizingthilangac100% (1)
- AnalogyDocument24 pagesAnalogyTrung TranNo ratings yet
- Importance of Fish CultureDocument14 pagesImportance of Fish Culturedownfree28100% (2)
- Dental Changes in Humans With Untreated Normal Occlusion Throughout Lifetime A Systematic Scoping ReviewDocument26 pagesDental Changes in Humans With Untreated Normal Occlusion Throughout Lifetime A Systematic Scoping ReviewNatasha NascimentoNo ratings yet