
Ref 05
Ref 05
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Saturn Time Cube SimulationDocument67 pagesThe Saturn Time Cube Simulationtriple7inc100% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ราคาอ้างอิงของยา เดือนมกราคม-มีนาคม 2561Document143 pagesราคาอ้างอิงของยา เดือนมกราคม-มีนาคม 2561Tommy PanyaratNo ratings yet
- Feedback Part of A System (Dylan Wiliam)Document4 pagesFeedback Part of A System (Dylan Wiliam)ajmccarthynzNo ratings yet
- XRAYDocument9 pagesXRAYraniakjsNo ratings yet
- Khalida - Clinical Significance of Early Repolarization On Long QT SyndromeDocument7 pagesKhalida - Clinical Significance of Early Repolarization On Long QT SyndromeraniakjsNo ratings yet
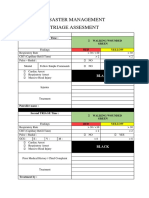
- Disaster Management Triage Assesment: Person's Name: Initial TRIAGE Time: Green RED YellowDocument1 pageDisaster Management Triage Assesment: Person's Name: Initial TRIAGE Time: Green RED YellowraniakjsNo ratings yet
- Macam Jarum HectingDocument1 pageMacam Jarum HectingraniakjsNo ratings yet
- Laporan Faal UrinDocument6 pagesLaporan Faal UrinraniakjsNo ratings yet
- Ni Based Superalloy: Casting Technology, Metallurgy, Development, Properties and ApplicationsDocument46 pagesNi Based Superalloy: Casting Technology, Metallurgy, Development, Properties and ApplicationsffazlaliNo ratings yet
- Bicycle Owner's Manual: ImportantDocument55 pagesBicycle Owner's Manual: ImportantAnderson HenriqueNo ratings yet
- 66 - Series Singer 66 Sewing Machine ManualDocument16 pages66 - Series Singer 66 Sewing Machine ManualCynthia PorterNo ratings yet
- Origami Symbols: (Fold The Paper Towards You)Document6 pagesOrigami Symbols: (Fold The Paper Towards You)Ian De La CruzNo ratings yet
- OutputDocument39 pagesOutputRuben Condori Canaviri100% (2)
- List - Parts of Bahay Na Bato - Filipiniana 101Document7 pagesList - Parts of Bahay Na Bato - Filipiniana 101Eriellynn Liza100% (1)
- Ep English Teachers GuideDocument180 pagesEp English Teachers GuideJessy ChrisNo ratings yet
- Safety Data Sheet Versamul Ic: 1. Identification of The Substance/Preparation and Company/UndertakingDocument4 pagesSafety Data Sheet Versamul Ic: 1. Identification of The Substance/Preparation and Company/UndertakingJose Rafael Martinez PerezNo ratings yet
- ECOi SPW-CR485GXH56BDocument10 pagesECOi SPW-CR485GXH56BJesus Raul Murillo EspinozaNo ratings yet
- Dimaampao Tax NotesDocument69 pagesDimaampao Tax NotestinctNo ratings yet
- United Republic of Tanzania Tanzania Civil Aviation Authority Application For Renewal of An Instrument RatingDocument4 pagesUnited Republic of Tanzania Tanzania Civil Aviation Authority Application For Renewal of An Instrument Ratingcapt.sahaagNo ratings yet
- Basic Rules and Tips in Group DiscussionsDocument2 pagesBasic Rules and Tips in Group Discussionssudarsanamma89% (9)
- Oblicon Reviewer Q and ADocument13 pagesOblicon Reviewer Q and ARussel SirotNo ratings yet
- HRM1Document13 pagesHRM1Niomi GolraiNo ratings yet
- Sec 3 Welding Imperfections (Defects)Document31 pagesSec 3 Welding Imperfections (Defects)Abdullah100% (1)
- Tyler's Curriculum Evaluation ModelDocument13 pagesTyler's Curriculum Evaluation Modelmashabalerato26No ratings yet
- Task 1 - PCK8Document8 pagesTask 1 - PCK8Andrea SantosNo ratings yet
- #SyallabusDocument33 pages#SyallabusSandeep B MNo ratings yet
- Fuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FutureDocument18 pagesFuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FuturecriscazanNo ratings yet
- Worksheet 9 - ClimateChangeDocument1 pageWorksheet 9 - ClimateChangeVanessa MondejarNo ratings yet
- Addmrpt 1 36558 36559Document7 pagesAddmrpt 1 36558 36559Anonymous ZGcs7MwsLNo ratings yet
- Clinical and Diagnostic Imaging Findings in Police Working Dogs Referred For Hip OsteoarthritisDocument11 pagesClinical and Diagnostic Imaging Findings in Police Working Dogs Referred For Hip OsteoarthritisEquilibrium EduardoNo ratings yet
- Perfetti Van MelleDocument24 pagesPerfetti Van MelleYahya Niazi100% (1)
- Touch FootballDocument75 pagesTouch FootballIon Balda MarinNo ratings yet
- Microlearning Lesson Plan IntelDocument3 pagesMicrolearning Lesson Plan IntelAditi JadhavNo ratings yet
- Taxation Law Compile 07-18 PDFDocument85 pagesTaxation Law Compile 07-18 PDFOshin Noleal SabacoNo ratings yet
- Antioxidant Activity of Medicinal Herb Zygophyllum Potaninii Maxim On Carbon Tetra Chloride InduceDocument11 pagesAntioxidant Activity of Medicinal Herb Zygophyllum Potaninii Maxim On Carbon Tetra Chloride InduceАмар ЭрдэнэцогтNo ratings yet











































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Saturn Time Cube SimulationDocument67 pagesThe Saturn Time Cube Simulationtriple7inc100% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ราคาอ้างอิงของยา เดือนมกราคม-มีนาคม 2561Document143 pagesราคาอ้างอิงของยา เดือนมกราคม-มีนาคม 2561Tommy PanyaratNo ratings yet
- Feedback Part of A System (Dylan Wiliam)Document4 pagesFeedback Part of A System (Dylan Wiliam)ajmccarthynzNo ratings yet
- XRAYDocument9 pagesXRAYraniakjsNo ratings yet
- Khalida - Clinical Significance of Early Repolarization On Long QT SyndromeDocument7 pagesKhalida - Clinical Significance of Early Repolarization On Long QT SyndromeraniakjsNo ratings yet
- Disaster Management Triage Assesment: Person's Name: Initial TRIAGE Time: Green RED YellowDocument1 pageDisaster Management Triage Assesment: Person's Name: Initial TRIAGE Time: Green RED YellowraniakjsNo ratings yet
- Macam Jarum HectingDocument1 pageMacam Jarum HectingraniakjsNo ratings yet
- Laporan Faal UrinDocument6 pagesLaporan Faal UrinraniakjsNo ratings yet
- Ni Based Superalloy: Casting Technology, Metallurgy, Development, Properties and ApplicationsDocument46 pagesNi Based Superalloy: Casting Technology, Metallurgy, Development, Properties and ApplicationsffazlaliNo ratings yet
- Bicycle Owner's Manual: ImportantDocument55 pagesBicycle Owner's Manual: ImportantAnderson HenriqueNo ratings yet
- 66 - Series Singer 66 Sewing Machine ManualDocument16 pages66 - Series Singer 66 Sewing Machine ManualCynthia PorterNo ratings yet
- Origami Symbols: (Fold The Paper Towards You)Document6 pagesOrigami Symbols: (Fold The Paper Towards You)Ian De La CruzNo ratings yet
- OutputDocument39 pagesOutputRuben Condori Canaviri100% (2)
- List - Parts of Bahay Na Bato - Filipiniana 101Document7 pagesList - Parts of Bahay Na Bato - Filipiniana 101Eriellynn Liza100% (1)
- Ep English Teachers GuideDocument180 pagesEp English Teachers GuideJessy ChrisNo ratings yet
- Safety Data Sheet Versamul Ic: 1. Identification of The Substance/Preparation and Company/UndertakingDocument4 pagesSafety Data Sheet Versamul Ic: 1. Identification of The Substance/Preparation and Company/UndertakingJose Rafael Martinez PerezNo ratings yet
- ECOi SPW-CR485GXH56BDocument10 pagesECOi SPW-CR485GXH56BJesus Raul Murillo EspinozaNo ratings yet
- Dimaampao Tax NotesDocument69 pagesDimaampao Tax NotestinctNo ratings yet
- United Republic of Tanzania Tanzania Civil Aviation Authority Application For Renewal of An Instrument RatingDocument4 pagesUnited Republic of Tanzania Tanzania Civil Aviation Authority Application For Renewal of An Instrument Ratingcapt.sahaagNo ratings yet
- Basic Rules and Tips in Group DiscussionsDocument2 pagesBasic Rules and Tips in Group Discussionssudarsanamma89% (9)
- Oblicon Reviewer Q and ADocument13 pagesOblicon Reviewer Q and ARussel SirotNo ratings yet
- HRM1Document13 pagesHRM1Niomi GolraiNo ratings yet
- Sec 3 Welding Imperfections (Defects)Document31 pagesSec 3 Welding Imperfections (Defects)Abdullah100% (1)
- Tyler's Curriculum Evaluation ModelDocument13 pagesTyler's Curriculum Evaluation Modelmashabalerato26No ratings yet
- Task 1 - PCK8Document8 pagesTask 1 - PCK8Andrea SantosNo ratings yet
- #SyallabusDocument33 pages#SyallabusSandeep B MNo ratings yet
- Fuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FutureDocument18 pagesFuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FuturecriscazanNo ratings yet
- Worksheet 9 - ClimateChangeDocument1 pageWorksheet 9 - ClimateChangeVanessa MondejarNo ratings yet
- Addmrpt 1 36558 36559Document7 pagesAddmrpt 1 36558 36559Anonymous ZGcs7MwsLNo ratings yet
- Clinical and Diagnostic Imaging Findings in Police Working Dogs Referred For Hip OsteoarthritisDocument11 pagesClinical and Diagnostic Imaging Findings in Police Working Dogs Referred For Hip OsteoarthritisEquilibrium EduardoNo ratings yet
- Perfetti Van MelleDocument24 pagesPerfetti Van MelleYahya Niazi100% (1)
- Touch FootballDocument75 pagesTouch FootballIon Balda MarinNo ratings yet
- Microlearning Lesson Plan IntelDocument3 pagesMicrolearning Lesson Plan IntelAditi JadhavNo ratings yet
- Taxation Law Compile 07-18 PDFDocument85 pagesTaxation Law Compile 07-18 PDFOshin Noleal SabacoNo ratings yet
- Antioxidant Activity of Medicinal Herb Zygophyllum Potaninii Maxim On Carbon Tetra Chloride InduceDocument11 pagesAntioxidant Activity of Medicinal Herb Zygophyllum Potaninii Maxim On Carbon Tetra Chloride InduceАмар ЭрдэнэцогтNo ratings yet