
Pediatric Neuroendocrine Neoplasia of The Parathyroid Glands: Delving Into Primary Hyperparathyroidism
Pediatric Neuroendocrine Neoplasia of The Parathyroid Glands: Delving Into Primary Hyperparathyroidism
You might also like
- Sumar Lucrari MarisiensisDocument103 pagesSumar Lucrari MarisiensisHumaMihaiNo ratings yet
- Clinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaDocument7 pagesClinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaIJAR JOURNALNo ratings yet
- Triple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesDocument10 pagesTriple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesIJAR JOURNALNo ratings yet
- Or 32 6 2836 PDFDocument9 pagesOr 32 6 2836 PDFJose SirittNo ratings yet
- Pituitary Incidentalomas Best Practices and Looking AheadDocument9 pagesPituitary Incidentalomas Best Practices and Looking AheadJulieta LopezNo ratings yet
- Prevalence of Rheumatic Heart Disease Detected by Echocardiographic ScreeningDocument7 pagesPrevalence of Rheumatic Heart Disease Detected by Echocardiographic Screeningandamar0290No ratings yet
- Incidence and Profile of Benign Epithelial Tumors of Salivary Glands From A Single Center in Northeast of BrazilDocument6 pagesIncidence and Profile of Benign Epithelial Tumors of Salivary Glands From A Single Center in Northeast of Brazilmakif18651No ratings yet
- 3 The Risk of Second Primary Tumors in Head and Neck Cancer. A Systematic ReviewDocument11 pages3 The Risk of Second Primary Tumors in Head and Neck Cancer. A Systematic Review2211801733No ratings yet
- HydrocephalusDocument8 pagesHydrocephaluscaliptra36No ratings yet
- A Clinico-Pathological Study of Thyroid Nodules and Correlation Among Ultrasonographic, Cytologic, and Histologic FindingsDocument8 pagesA Clinico-Pathological Study of Thyroid Nodules and Correlation Among Ultrasonographic, Cytologic, and Histologic FindingsFaisal AhmedNo ratings yet
- 05.natural Course of Low Risk NeuroblastomaDocument5 pages05.natural Course of Low Risk Neuroblastomavalentina rojasNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Research Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryDocument5 pagesResearch Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryAyu Septiari ArtatiNo ratings yet
- As Trocito MaDocument10 pagesAs Trocito Majeimy_carolina4163No ratings yet
- A Novel Method For Rapid Molecular Subgrouping of MedulloblastomaDocument10 pagesA Novel Method For Rapid Molecular Subgrouping of MedulloblastomaelleNo ratings yet
- Parik H 2015Document12 pagesParik H 2015Victor CorreaNo ratings yet
- Clinical Presentations, Diagnosis, Mortality and Prognostic Markers of Tuberculous Meningitis in Vietnamese Children: A Prospective Descriptive StudyDocument10 pagesClinical Presentations, Diagnosis, Mortality and Prognostic Markers of Tuberculous Meningitis in Vietnamese Children: A Prospective Descriptive StudySilva Dicha GiovanoNo ratings yet
- Caselli 2014Document5 pagesCaselli 2014AdrianaGallardoTapiaNo ratings yet
- (1479683X - European Journal of Endocrinology) Cancer Risk in Hyperprolactinemia Patients - A Population-Based Cohort StudyDocument7 pages(1479683X - European Journal of Endocrinology) Cancer Risk in Hyperprolactinemia Patients - A Population-Based Cohort Studygeng gengNo ratings yet
- Antenat Hydronephr-4Document8 pagesAntenat Hydronephr-4Ioannis ValioulisNo ratings yet
- Javali2018 en IdDocument10 pagesJavali2018 en IdDona Ratna SariNo ratings yet
- March 2024 - The Management of Phaeochromocytomas and Paragangliomas in the Era of Precision Medicine Where Are We Now Evidence-Based Systemic Treatment Options and Future Cluster Oriented PerspectivesDocument22 pagesMarch 2024 - The Management of Phaeochromocytomas and Paragangliomas in the Era of Precision Medicine Where Are We Now Evidence-Based Systemic Treatment Options and Future Cluster Oriented PerspectivesAndrei MarianNo ratings yet
- Operative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-AnalysisDocument9 pagesOperative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-Analysisyarianna2No ratings yet
- Ref 6Document10 pagesRef 6Andri ArdhanyNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author Manuscriptdini kusmaharaniNo ratings yet
- Cripe2017 2750523Document4 pagesCripe2017 2750523فرجني موغNo ratings yet
- Patients and General Practitioner Knowledge and Perception of Testicular Self Examination For CancerDocument7 pagesPatients and General Practitioner Knowledge and Perception of Testicular Self Examination For CancerbumblecitoNo ratings yet
- Treatment For Benign Thyroid Nodules With A CombinDocument7 pagesTreatment For Benign Thyroid Nodules With A CombindarthjesussithNo ratings yet
- LGM LGM D 09 1Document7 pagesLGM LGM D 09 1Rully SyahrizalNo ratings yet
- Perilongo 1997Document7 pagesPerilongo 1997Gustav RSRNo ratings yet
- Adults Brain Tumor in Cipto Mangunkusumo General Hospital A Descriptive EpidemiologyDocument5 pagesAdults Brain Tumor in Cipto Mangunkusumo General Hospital A Descriptive EpidemiologyHarun NANo ratings yet
- Maris 2007Document15 pagesMaris 2007asialoren74No ratings yet
- Precocious Puberty: Epidemiology, Clinical Presentation, Diagnosis, and EtiologiesDocument5 pagesPrecocious Puberty: Epidemiology, Clinical Presentation, Diagnosis, and EtiologiesIJAR JOURNALNo ratings yet
- Summary of Fukushima Thyroid Cancer Cases As of November 29Document6 pagesSummary of Fukushima Thyroid Cancer Cases As of November 29Yuri HiranumaNo ratings yet
- Male Breast Cancer: An Institutional ExperienceDocument5 pagesMale Breast Cancer: An Institutional ExperienceIJAR JOURNALNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 pagesClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaNo ratings yet
- Management Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaDocument4 pagesManagement Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breast Cancer and Biomedical Informatics: The Prognochip ProjectDocument6 pagesBreast Cancer and Biomedical Informatics: The Prognochip ProjectRuanita VeigaNo ratings yet
- JURNALDocument11 pagesJURNALdiklat.rsakademis2024No ratings yet
- Strokeaha 118 021301Document6 pagesStrokeaha 118 021301Rahma Nur AmeliaNo ratings yet
- ArticleDocument16 pagesArticleobbyNo ratings yet
- Prognostic Factors For Recurrence in Patients With Papillary Thyroid CarcinomaDocument8 pagesPrognostic Factors For Recurrence in Patients With Papillary Thyroid CarcinomaLeonardo LeónNo ratings yet
- Adrenal Neuroblastoma With Bone Marrow Metastasis in Anadult: A Case Report and Review of The LiteratureDocument5 pagesAdrenal Neuroblastoma With Bone Marrow Metastasis in Anadult: A Case Report and Review of The LiteratureIJAR JOURNALNo ratings yet
- Validity of A Minimally Invasive Autopsy For CoD Determination On Stillborn Babies and Neonates in MozambiqueDocument17 pagesValidity of A Minimally Invasive Autopsy For CoD Determination On Stillborn Babies and Neonates in MozambiqueDenys PutraNo ratings yet
- ClinicalCharacteristicsAndProgrognostic AstrocytomaDocument12 pagesClinicalCharacteristicsAndProgrognostic AstrocytomaDesty PurnamasariNo ratings yet
- JournalDocument6 pagesJournalnaelarizqiNo ratings yet
- Kim 2017Document14 pagesKim 2017Cota AncutaNo ratings yet
- Cancer - 2014 - Hallet - Exploring The Rising Incidence of Neuroendocrine Tumors A Population Based Analysis ofDocument9 pagesCancer - 2014 - Hallet - Exploring The Rising Incidence of Neuroendocrine Tumors A Population Based Analysis ofRepositorioNo ratings yet
- Accepted Manuscript: 10.1016/j.bpa.2016.12.002Document21 pagesAccepted Manuscript: 10.1016/j.bpa.2016.12.002Indra WijayaNo ratings yet
- Clinical Course of Untreated Cerebral Cavernous MalformationsDocument8 pagesClinical Course of Untreated Cerebral Cavernous MalformationsMalaspulgasNo ratings yet
- HydrocephalusDocument9 pagesHydrocephalusDeby AnditaNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Pediatrics 2013 Penson E1897 907Document11 pagesPediatrics 2013 Penson E1897 907Hugo RoldanNo ratings yet
- Ijms 25 00732Document26 pagesIjms 25 00732Alaa TahaNo ratings yet
- Paradigm Shift A Comprehensive Review of Ovarian Cancer ManagementDocument28 pagesParadigm Shift A Comprehensive Review of Ovarian Cancer Managementevapruvost2No ratings yet
- Guideline - Diagnosis - Genetic - Pheochromocytomas 2021Document25 pagesGuideline - Diagnosis - Genetic - Pheochromocytomas 2021mehidimed1889No ratings yet
- Multidisciplinary Practice Guidelines For The Diagnosis, Genetic Counseling and Treatment of Pheochromocytomas and ParagangliomasDocument19 pagesMultidisciplinary Practice Guidelines For The Diagnosis, Genetic Counseling and Treatment of Pheochromocytomas and ParagangliomasLaura Marina IlincaNo ratings yet
- Medicina 59 01151Document9 pagesMedicina 59 01151Lissaberti AmaliahNo ratings yet
- Parathyroid Adenoma in Children: A Rare Cause of Primary HyperparathyroidismDocument3 pagesParathyroid Adenoma in Children: A Rare Cause of Primary HyperparathyroidismTimothy supitNo ratings yet
- Molecular and Clinical Spectrum of Primary HyperparathyroidismDocument40 pagesMolecular and Clinical Spectrum of Primary HyperparathyroidismTimothy supitNo ratings yet
- The Role and Need For Psychological Support in The Treatment of Adolescents and Young People Suffering From Type 1 DiabetesDocument7 pagesThe Role and Need For Psychological Support in The Treatment of Adolescents and Young People Suffering From Type 1 DiabetesTimothy supitNo ratings yet
- International Consensus Guideline On Small For Gestational Age: Etiology and Management From Infancy To Early AdulthoodDocument27 pagesInternational Consensus Guideline On Small For Gestational Age: Etiology and Management From Infancy To Early AdulthoodTimothy supitNo ratings yet
- Small For Gestational Age Preterm Neonates Exhibit Defective GH:IGF1 Signaling PathwayDocument8 pagesSmall For Gestational Age Preterm Neonates Exhibit Defective GH:IGF1 Signaling PathwayTimothy supitNo ratings yet
- Critical Appraisal of Medical Literature - Kuntjoro HarimurtiDocument53 pagesCritical Appraisal of Medical Literature - Kuntjoro HarimurtiTimothy supitNo ratings yet
- Glycemic Control, Associated Factors, Acute Complications of Type 1 Diabetes Mellitus in Children, Adolescents and Young Adults in TanzaniaDocument8 pagesGlycemic Control, Associated Factors, Acute Complications of Type 1 Diabetes Mellitus in Children, Adolescents and Young Adults in TanzaniaTimothy supitNo ratings yet
- Factors Associated With Glycemic Control in Children and Adolescents With Type 1 Diabetes Mellitus at A Tertiary Care Center in ThailandDocument8 pagesFactors Associated With Glycemic Control in Children and Adolescents With Type 1 Diabetes Mellitus at A Tertiary Care Center in ThailandTimothy supitNo ratings yet
- Journal Reading Congenital HypogonadotropicDocument13 pagesJournal Reading Congenital HypogonadotropicTimothy supitNo ratings yet
- DV - Dr. Sri AwaliaDocument30 pagesDV - Dr. Sri AwaliaTimothy supitNo ratings yet
- ALERGI OBAT Prof. Dr. HardyantoDocument51 pagesALERGI OBAT Prof. Dr. HardyantoTimothy supitNo ratings yet
- Semen Quality Obesity PlusDocument23 pagesSemen Quality Obesity PlusPOPA EMILIANNo ratings yet
- Glucagon-Like Peptide 1 수용체작용제 최신지견Document8 pagesGlucagon-Like Peptide 1 수용체작용제 최신지견이호원No ratings yet
- NMAT Perceptual Acuity Module 3 WojrkehjDocument4 pagesNMAT Perceptual Acuity Module 3 Wojrkehjlorrainebarandon100% (2)
- ThyroidectomyDocument50 pagesThyroidectomyKyle Jingco100% (2)
- Coordination and Control (Ch#12) (1) .PDF FinalDocument19 pagesCoordination and Control (Ch#12) (1) .PDF FinalUmme AbdullahNo ratings yet
- Acth Stimulation Testing Protocol CanineDocument2 pagesActh Stimulation Testing Protocol CanineSpital Veterinar AndivetNo ratings yet
- HucogDocument3 pagesHucogSairam EdupugantiNo ratings yet
- Glandular EpitheliumDocument34 pagesGlandular EpitheliumAnonymous WBMLOgPNo ratings yet
- Thyroid Ultrasound, State of The ArtDocument15 pagesThyroid Ultrasound, State of The ArtDe DawnNo ratings yet
- Sex Book Urdu PDFDocument124 pagesSex Book Urdu PDFKhalid Almas75% (8)
- Birth Control Made Simple 2010Document5 pagesBirth Control Made Simple 2010Richard WahlNo ratings yet
- TDAH ADHD e Def de Iodo 2004Document7 pagesTDAH ADHD e Def de Iodo 2004Pollyana Furtado JunqueiraNo ratings yet
- NNYGDocument13 pagesNNYGrose ONo ratings yet
- Ultrasound in The Prevention, Diagnosis and Management of Ovarian Hyperstimulation Syndrome in BamakoDocument9 pagesUltrasound in The Prevention, Diagnosis and Management of Ovarian Hyperstimulation Syndrome in BamakoIJAR JOURNALNo ratings yet
- Neuropeptido YDocument8 pagesNeuropeptido YAngela Del Castillo AriasNo ratings yet
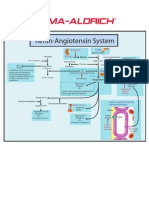
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Diabetes RoadmapDocument8 pagesDiabetes Roadmapwuryan dewiNo ratings yet
- 5.0 Sessions of Interest: Wednesday, November 16Document17 pages5.0 Sessions of Interest: Wednesday, November 16api-340273587No ratings yet
- Hubungan Riwayat Keluarga, Stres, Kualitas Tidur, Makanan, Dan Kadar Zinc Pada Derajat Keparahan Akne VulgarisDocument8 pagesHubungan Riwayat Keluarga, Stres, Kualitas Tidur, Makanan, Dan Kadar Zinc Pada Derajat Keparahan Akne VulgarisIna Eta AyenNo ratings yet
- 2023 IABO Scientific Paper - TemplateDocument3 pages2023 IABO Scientific Paper - TemplateKayla Jihan NamiroNo ratings yet
- The Neuroendocrinology of The Microbiota-Gut-BrainDocument74 pagesThe Neuroendocrinology of The Microbiota-Gut-BrainSandraosoNo ratings yet
- VIR0815 Suprelorin FAQ Sheet A4Document1 pageVIR0815 Suprelorin FAQ Sheet A4Solo PubliNo ratings yet
- Menopause GUI201606V1.0FINALDocument5 pagesMenopause GUI201606V1.0FINALKhalilKhaliNo ratings yet
- Secretin Hormone Activates Satiation by Triggering Brown FatDocument1 pageSecretin Hormone Activates Satiation by Triggering Brown FatTalal ZariNo ratings yet
- Review Notes - Endocrine ConditionsDocument3 pagesReview Notes - Endocrine ConditionsKarol De La CruzNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveDocument5 pagesLaboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveP Nagaraju RajuNo ratings yet
- Pharmacotherapy of Thyroid DisordersDocument6 pagesPharmacotherapy of Thyroid DisordersShaden -No ratings yet
- Acromegaly PDFDocument7 pagesAcromegaly PDFBudi AthAnza SuhartonoNo ratings yet
- Blocked Fallopian TubesDocument2 pagesBlocked Fallopian TubesPreethi JoseNo ratings yet
- Thyrotoxicosis: By: DR Mukesh Kumar Samota PG (M.D. Medicine) Medical College Jhalawar (RajasthanDocument40 pagesThyrotoxicosis: By: DR Mukesh Kumar Samota PG (M.D. Medicine) Medical College Jhalawar (RajasthanShravani ShagapuramNo ratings yet




































































































Download as pdf or txt
You might also like
- Sumar Lucrari MarisiensisDocument103 pagesSumar Lucrari MarisiensisHumaMihaiNo ratings yet
- Clinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaDocument7 pagesClinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaIJAR JOURNALNo ratings yet
- Triple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesDocument10 pagesTriple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesIJAR JOURNALNo ratings yet
- Or 32 6 2836 PDFDocument9 pagesOr 32 6 2836 PDFJose SirittNo ratings yet
- Pituitary Incidentalomas Best Practices and Looking AheadDocument9 pagesPituitary Incidentalomas Best Practices and Looking AheadJulieta LopezNo ratings yet
- Prevalence of Rheumatic Heart Disease Detected by Echocardiographic ScreeningDocument7 pagesPrevalence of Rheumatic Heart Disease Detected by Echocardiographic Screeningandamar0290No ratings yet
- Incidence and Profile of Benign Epithelial Tumors of Salivary Glands From A Single Center in Northeast of BrazilDocument6 pagesIncidence and Profile of Benign Epithelial Tumors of Salivary Glands From A Single Center in Northeast of Brazilmakif18651No ratings yet
- 3 The Risk of Second Primary Tumors in Head and Neck Cancer. A Systematic ReviewDocument11 pages3 The Risk of Second Primary Tumors in Head and Neck Cancer. A Systematic Review2211801733No ratings yet
- HydrocephalusDocument8 pagesHydrocephaluscaliptra36No ratings yet
- A Clinico-Pathological Study of Thyroid Nodules and Correlation Among Ultrasonographic, Cytologic, and Histologic FindingsDocument8 pagesA Clinico-Pathological Study of Thyroid Nodules and Correlation Among Ultrasonographic, Cytologic, and Histologic FindingsFaisal AhmedNo ratings yet
- 05.natural Course of Low Risk NeuroblastomaDocument5 pages05.natural Course of Low Risk Neuroblastomavalentina rojasNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Research Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryDocument5 pagesResearch Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryAyu Septiari ArtatiNo ratings yet
- As Trocito MaDocument10 pagesAs Trocito Majeimy_carolina4163No ratings yet
- A Novel Method For Rapid Molecular Subgrouping of MedulloblastomaDocument10 pagesA Novel Method For Rapid Molecular Subgrouping of MedulloblastomaelleNo ratings yet
- Parik H 2015Document12 pagesParik H 2015Victor CorreaNo ratings yet
- Clinical Presentations, Diagnosis, Mortality and Prognostic Markers of Tuberculous Meningitis in Vietnamese Children: A Prospective Descriptive StudyDocument10 pagesClinical Presentations, Diagnosis, Mortality and Prognostic Markers of Tuberculous Meningitis in Vietnamese Children: A Prospective Descriptive StudySilva Dicha GiovanoNo ratings yet
- Caselli 2014Document5 pagesCaselli 2014AdrianaGallardoTapiaNo ratings yet
- (1479683X - European Journal of Endocrinology) Cancer Risk in Hyperprolactinemia Patients - A Population-Based Cohort StudyDocument7 pages(1479683X - European Journal of Endocrinology) Cancer Risk in Hyperprolactinemia Patients - A Population-Based Cohort Studygeng gengNo ratings yet
- Antenat Hydronephr-4Document8 pagesAntenat Hydronephr-4Ioannis ValioulisNo ratings yet
- Javali2018 en IdDocument10 pagesJavali2018 en IdDona Ratna SariNo ratings yet
- March 2024 - The Management of Phaeochromocytomas and Paragangliomas in the Era of Precision Medicine Where Are We Now Evidence-Based Systemic Treatment Options and Future Cluster Oriented PerspectivesDocument22 pagesMarch 2024 - The Management of Phaeochromocytomas and Paragangliomas in the Era of Precision Medicine Where Are We Now Evidence-Based Systemic Treatment Options and Future Cluster Oriented PerspectivesAndrei MarianNo ratings yet
- Operative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-AnalysisDocument9 pagesOperative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-Analysisyarianna2No ratings yet
- Ref 6Document10 pagesRef 6Andri ArdhanyNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author Manuscriptdini kusmaharaniNo ratings yet
- Cripe2017 2750523Document4 pagesCripe2017 2750523فرجني موغNo ratings yet
- Patients and General Practitioner Knowledge and Perception of Testicular Self Examination For CancerDocument7 pagesPatients and General Practitioner Knowledge and Perception of Testicular Self Examination For CancerbumblecitoNo ratings yet
- Treatment For Benign Thyroid Nodules With A CombinDocument7 pagesTreatment For Benign Thyroid Nodules With A CombindarthjesussithNo ratings yet
- LGM LGM D 09 1Document7 pagesLGM LGM D 09 1Rully SyahrizalNo ratings yet
- Perilongo 1997Document7 pagesPerilongo 1997Gustav RSRNo ratings yet
- Adults Brain Tumor in Cipto Mangunkusumo General Hospital A Descriptive EpidemiologyDocument5 pagesAdults Brain Tumor in Cipto Mangunkusumo General Hospital A Descriptive EpidemiologyHarun NANo ratings yet
- Maris 2007Document15 pagesMaris 2007asialoren74No ratings yet
- Precocious Puberty: Epidemiology, Clinical Presentation, Diagnosis, and EtiologiesDocument5 pagesPrecocious Puberty: Epidemiology, Clinical Presentation, Diagnosis, and EtiologiesIJAR JOURNALNo ratings yet
- Summary of Fukushima Thyroid Cancer Cases As of November 29Document6 pagesSummary of Fukushima Thyroid Cancer Cases As of November 29Yuri HiranumaNo ratings yet
- Male Breast Cancer: An Institutional ExperienceDocument5 pagesMale Breast Cancer: An Institutional ExperienceIJAR JOURNALNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 pagesClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaNo ratings yet
- Management Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaDocument4 pagesManagement Outcomes of Hydrocephalus Among Under Five Children in A Tertiary Hospital in Gombe North Eastern NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breast Cancer and Biomedical Informatics: The Prognochip ProjectDocument6 pagesBreast Cancer and Biomedical Informatics: The Prognochip ProjectRuanita VeigaNo ratings yet
- JURNALDocument11 pagesJURNALdiklat.rsakademis2024No ratings yet
- Strokeaha 118 021301Document6 pagesStrokeaha 118 021301Rahma Nur AmeliaNo ratings yet
- ArticleDocument16 pagesArticleobbyNo ratings yet
- Prognostic Factors For Recurrence in Patients With Papillary Thyroid CarcinomaDocument8 pagesPrognostic Factors For Recurrence in Patients With Papillary Thyroid CarcinomaLeonardo LeónNo ratings yet
- Adrenal Neuroblastoma With Bone Marrow Metastasis in Anadult: A Case Report and Review of The LiteratureDocument5 pagesAdrenal Neuroblastoma With Bone Marrow Metastasis in Anadult: A Case Report and Review of The LiteratureIJAR JOURNALNo ratings yet
- Validity of A Minimally Invasive Autopsy For CoD Determination On Stillborn Babies and Neonates in MozambiqueDocument17 pagesValidity of A Minimally Invasive Autopsy For CoD Determination On Stillborn Babies and Neonates in MozambiqueDenys PutraNo ratings yet
- ClinicalCharacteristicsAndProgrognostic AstrocytomaDocument12 pagesClinicalCharacteristicsAndProgrognostic AstrocytomaDesty PurnamasariNo ratings yet
- JournalDocument6 pagesJournalnaelarizqiNo ratings yet
- Kim 2017Document14 pagesKim 2017Cota AncutaNo ratings yet
- Cancer - 2014 - Hallet - Exploring The Rising Incidence of Neuroendocrine Tumors A Population Based Analysis ofDocument9 pagesCancer - 2014 - Hallet - Exploring The Rising Incidence of Neuroendocrine Tumors A Population Based Analysis ofRepositorioNo ratings yet
- Accepted Manuscript: 10.1016/j.bpa.2016.12.002Document21 pagesAccepted Manuscript: 10.1016/j.bpa.2016.12.002Indra WijayaNo ratings yet
- Clinical Course of Untreated Cerebral Cavernous MalformationsDocument8 pagesClinical Course of Untreated Cerebral Cavernous MalformationsMalaspulgasNo ratings yet
- HydrocephalusDocument9 pagesHydrocephalusDeby AnditaNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Pediatrics 2013 Penson E1897 907Document11 pagesPediatrics 2013 Penson E1897 907Hugo RoldanNo ratings yet
- Ijms 25 00732Document26 pagesIjms 25 00732Alaa TahaNo ratings yet
- Paradigm Shift A Comprehensive Review of Ovarian Cancer ManagementDocument28 pagesParadigm Shift A Comprehensive Review of Ovarian Cancer Managementevapruvost2No ratings yet
- Guideline - Diagnosis - Genetic - Pheochromocytomas 2021Document25 pagesGuideline - Diagnosis - Genetic - Pheochromocytomas 2021mehidimed1889No ratings yet
- Multidisciplinary Practice Guidelines For The Diagnosis, Genetic Counseling and Treatment of Pheochromocytomas and ParagangliomasDocument19 pagesMultidisciplinary Practice Guidelines For The Diagnosis, Genetic Counseling and Treatment of Pheochromocytomas and ParagangliomasLaura Marina IlincaNo ratings yet
- Medicina 59 01151Document9 pagesMedicina 59 01151Lissaberti AmaliahNo ratings yet
- Parathyroid Adenoma in Children: A Rare Cause of Primary HyperparathyroidismDocument3 pagesParathyroid Adenoma in Children: A Rare Cause of Primary HyperparathyroidismTimothy supitNo ratings yet
- Molecular and Clinical Spectrum of Primary HyperparathyroidismDocument40 pagesMolecular and Clinical Spectrum of Primary HyperparathyroidismTimothy supitNo ratings yet
- The Role and Need For Psychological Support in The Treatment of Adolescents and Young People Suffering From Type 1 DiabetesDocument7 pagesThe Role and Need For Psychological Support in The Treatment of Adolescents and Young People Suffering From Type 1 DiabetesTimothy supitNo ratings yet
- International Consensus Guideline On Small For Gestational Age: Etiology and Management From Infancy To Early AdulthoodDocument27 pagesInternational Consensus Guideline On Small For Gestational Age: Etiology and Management From Infancy To Early AdulthoodTimothy supitNo ratings yet
- Small For Gestational Age Preterm Neonates Exhibit Defective GH:IGF1 Signaling PathwayDocument8 pagesSmall For Gestational Age Preterm Neonates Exhibit Defective GH:IGF1 Signaling PathwayTimothy supitNo ratings yet
- Critical Appraisal of Medical Literature - Kuntjoro HarimurtiDocument53 pagesCritical Appraisal of Medical Literature - Kuntjoro HarimurtiTimothy supitNo ratings yet
- Glycemic Control, Associated Factors, Acute Complications of Type 1 Diabetes Mellitus in Children, Adolescents and Young Adults in TanzaniaDocument8 pagesGlycemic Control, Associated Factors, Acute Complications of Type 1 Diabetes Mellitus in Children, Adolescents and Young Adults in TanzaniaTimothy supitNo ratings yet
- Factors Associated With Glycemic Control in Children and Adolescents With Type 1 Diabetes Mellitus at A Tertiary Care Center in ThailandDocument8 pagesFactors Associated With Glycemic Control in Children and Adolescents With Type 1 Diabetes Mellitus at A Tertiary Care Center in ThailandTimothy supitNo ratings yet
- Journal Reading Congenital HypogonadotropicDocument13 pagesJournal Reading Congenital HypogonadotropicTimothy supitNo ratings yet
- DV - Dr. Sri AwaliaDocument30 pagesDV - Dr. Sri AwaliaTimothy supitNo ratings yet
- ALERGI OBAT Prof. Dr. HardyantoDocument51 pagesALERGI OBAT Prof. Dr. HardyantoTimothy supitNo ratings yet
- Semen Quality Obesity PlusDocument23 pagesSemen Quality Obesity PlusPOPA EMILIANNo ratings yet
- Glucagon-Like Peptide 1 수용체작용제 최신지견Document8 pagesGlucagon-Like Peptide 1 수용체작용제 최신지견이호원No ratings yet
- NMAT Perceptual Acuity Module 3 WojrkehjDocument4 pagesNMAT Perceptual Acuity Module 3 Wojrkehjlorrainebarandon100% (2)
- ThyroidectomyDocument50 pagesThyroidectomyKyle Jingco100% (2)
- Coordination and Control (Ch#12) (1) .PDF FinalDocument19 pagesCoordination and Control (Ch#12) (1) .PDF FinalUmme AbdullahNo ratings yet
- Acth Stimulation Testing Protocol CanineDocument2 pagesActh Stimulation Testing Protocol CanineSpital Veterinar AndivetNo ratings yet
- HucogDocument3 pagesHucogSairam EdupugantiNo ratings yet
- Glandular EpitheliumDocument34 pagesGlandular EpitheliumAnonymous WBMLOgPNo ratings yet
- Thyroid Ultrasound, State of The ArtDocument15 pagesThyroid Ultrasound, State of The ArtDe DawnNo ratings yet
- Sex Book Urdu PDFDocument124 pagesSex Book Urdu PDFKhalid Almas75% (8)
- Birth Control Made Simple 2010Document5 pagesBirth Control Made Simple 2010Richard WahlNo ratings yet
- TDAH ADHD e Def de Iodo 2004Document7 pagesTDAH ADHD e Def de Iodo 2004Pollyana Furtado JunqueiraNo ratings yet
- NNYGDocument13 pagesNNYGrose ONo ratings yet
- Ultrasound in The Prevention, Diagnosis and Management of Ovarian Hyperstimulation Syndrome in BamakoDocument9 pagesUltrasound in The Prevention, Diagnosis and Management of Ovarian Hyperstimulation Syndrome in BamakoIJAR JOURNALNo ratings yet
- Neuropeptido YDocument8 pagesNeuropeptido YAngela Del Castillo AriasNo ratings yet
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Diabetes RoadmapDocument8 pagesDiabetes Roadmapwuryan dewiNo ratings yet
- 5.0 Sessions of Interest: Wednesday, November 16Document17 pages5.0 Sessions of Interest: Wednesday, November 16api-340273587No ratings yet
- Hubungan Riwayat Keluarga, Stres, Kualitas Tidur, Makanan, Dan Kadar Zinc Pada Derajat Keparahan Akne VulgarisDocument8 pagesHubungan Riwayat Keluarga, Stres, Kualitas Tidur, Makanan, Dan Kadar Zinc Pada Derajat Keparahan Akne VulgarisIna Eta AyenNo ratings yet
- 2023 IABO Scientific Paper - TemplateDocument3 pages2023 IABO Scientific Paper - TemplateKayla Jihan NamiroNo ratings yet
- The Neuroendocrinology of The Microbiota-Gut-BrainDocument74 pagesThe Neuroendocrinology of The Microbiota-Gut-BrainSandraosoNo ratings yet
- VIR0815 Suprelorin FAQ Sheet A4Document1 pageVIR0815 Suprelorin FAQ Sheet A4Solo PubliNo ratings yet
- Menopause GUI201606V1.0FINALDocument5 pagesMenopause GUI201606V1.0FINALKhalilKhaliNo ratings yet
- Secretin Hormone Activates Satiation by Triggering Brown FatDocument1 pageSecretin Hormone Activates Satiation by Triggering Brown FatTalal ZariNo ratings yet
- Review Notes - Endocrine ConditionsDocument3 pagesReview Notes - Endocrine ConditionsKarol De La CruzNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveDocument5 pagesLaboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveP Nagaraju RajuNo ratings yet
- Pharmacotherapy of Thyroid DisordersDocument6 pagesPharmacotherapy of Thyroid DisordersShaden -No ratings yet
- Acromegaly PDFDocument7 pagesAcromegaly PDFBudi AthAnza SuhartonoNo ratings yet
- Blocked Fallopian TubesDocument2 pagesBlocked Fallopian TubesPreethi JoseNo ratings yet
- Thyrotoxicosis: By: DR Mukesh Kumar Samota PG (M.D. Medicine) Medical College Jhalawar (RajasthanDocument40 pagesThyrotoxicosis: By: DR Mukesh Kumar Samota PG (M.D. Medicine) Medical College Jhalawar (RajasthanShravani ShagapuramNo ratings yet