Download as pdf or txt
You might also like
- Test Bank For Integrated Cardiopulmonary Pharmacology 3rd Edition ColbertDocument24 pagesTest Bank For Integrated Cardiopulmonary Pharmacology 3rd Edition ColbertTylerSmithirnx100% (58)
- NAPLEX NoteDocument58 pagesNAPLEX Notebapimirab654100% (1)
- TWU Anesthesia Cheat SheetDocument2 pagesTWU Anesthesia Cheat Sheetinvading_jam7582100% (6)
- NAPLEX Random Notes 68 PagesDocument51 pagesNAPLEX Random Notes 68 PagesZehra Amir100% (4)
- Pediatric Airway Card (Dual)Document1 pagePediatric Airway Card (Dual)Brian CloughNo ratings yet
- Required Formulas Look ThruDocument6 pagesRequired Formulas Look Thrukaylakmills_10135868No ratings yet
- Coagulación Analizador de Alto Rendimiento OUS Sysmex CS 2500 Spec Sheet 03 2016 - 152083723 - 11 - CompressedDocument3 pagesCoagulación Analizador de Alto Rendimiento OUS Sysmex CS 2500 Spec Sheet 03 2016 - 152083723 - 11 - CompressedAlemontse JiménezNo ratings yet
- Template Pasien OK 1 Template Pasien OK 1 Template Pasien OK 1Document1 pageTemplate Pasien OK 1 Template Pasien OK 1 Template Pasien OK 1Aulian syahNo ratings yet
- Pharmacokinetic Calculations Pharmacokinetic CalculationsDocument1 pagePharmacokinetic Calculations Pharmacokinetic CalculationsJoshua LaoNo ratings yet
- شرح بسيط - 100252Document2 pagesشرح بسيط - 100252magedsaif88No ratings yet
- Sympathomimetics: Noradrenaline Adrenaline Dopamine Isoprenaline DobutamineDocument4 pagesSympathomimetics: Noradrenaline Adrenaline Dopamine Isoprenaline DobutamineTomNo ratings yet
- Chemical Process Principles (CLB10904) : Chapter 2 Material Balance: (PART 4) : Recycle, Bypass & PurgeDocument25 pagesChemical Process Principles (CLB10904) : Chapter 2 Material Balance: (PART 4) : Recycle, Bypass & PurgeFATMIENo ratings yet
- Pharmaceutical Calculations: Metric SystemDocument8 pagesPharmaceutical Calculations: Metric SystemPrincess PasajolNo ratings yet
- SHC Antimicrobial Dosing GuideDocument7 pagesSHC Antimicrobial Dosing GuideHelder LopesNo ratings yet
- Digoxin Phenytoin Cyclosporin e Tacrolimu S Sirolimus Lithium CBZ VA PhenobarbDocument5 pagesDigoxin Phenytoin Cyclosporin e Tacrolimu S Sirolimus Lithium CBZ VA PhenobarbDana MradNo ratings yet
- CK MBDocument1 pageCK MBStacy SmithNo ratings yet
- CK-MB Liquiuv: Liquid Nac Activated Uv Test Creatine Kinase (Ec 2.7.3.2)Document1 pageCK-MB Liquiuv: Liquid Nac Activated Uv Test Creatine Kinase (Ec 2.7.3.2)Maher100% (1)
- WBW WBW M WBW A M UM ENDocument28 pagesWBW WBW M WBW A M UM ENAiniah Nur RahmanNo ratings yet
- 38054 台北市聯合醫院抗生素商品名對照表 PDFDocument99 pages38054 台北市聯合醫院抗生素商品名對照表 PDFka timNo ratings yet
- Rizzo1988 VD TeofilinDocument8 pagesRizzo1988 VD Teofilinike kurniaNo ratings yet
- Neonate: TPR of Newborns BW 1500gDocument9 pagesNeonate: TPR of Newborns BW 1500gAnne Lorraine BringasNo ratings yet
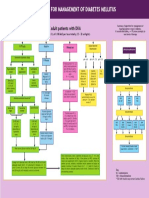
- Guideline For The Management of Adults Patients With DKA or HHSDocument3 pagesGuideline For The Management of Adults Patients With DKA or HHSJonard GiloNo ratings yet
- LUM IiCR48V 4000Document3 pagesLUM IiCR48V 4000dremymark26No ratings yet
- BCA-Based Protein Assay ProtocolDocument2 pagesBCA-Based Protein Assay Protocol이형우No ratings yet
- Grafik Antidiabetes-1Document2 pagesGrafik Antidiabetes-1Anggit PramitaNo ratings yet
- Cholinesterase - Dibucaine: Quantitative Determination of Cholinesterase With Dibucaine InhibiciónDocument2 pagesCholinesterase - Dibucaine: Quantitative Determination of Cholinesterase With Dibucaine InhibiciónAldair VillegasNo ratings yet
- Sports NutritionDocument29 pagesSports NutritionAnonymous jLY1EXDNo ratings yet
- Ipipe Queries May 2024Document10 pagesIpipe Queries May 2024irc.indusNo ratings yet
- Antimicrobial Dosing GuideDocument7 pagesAntimicrobial Dosing GuideMuhammad RawasNo ratings yet
- Pedia Stickers PDFDocument8 pagesPedia Stickers PDFAshNo ratings yet
- General Surgery Syllabus 5Document133 pagesGeneral Surgery Syllabus 5Steven GodelmanNo ratings yet
- Fluids and Electrolytes: MaintenanceDocument8 pagesFluids and Electrolytes: MaintenanceKarren Taquiqui PleteNo ratings yet
- Stanford Health Care Antimicrobial Dosing Reference GuideDocument7 pagesStanford Health Care Antimicrobial Dosing Reference GuideKarl Martin PinedaNo ratings yet
- ETC16Document30 pagesETC16EmilyRose YanezNo ratings yet
- Intracoronary Adenosine DosageDocument6 pagesIntracoronary Adenosine DosageKitchanan KosalathipNo ratings yet
- 3 - Teori Pemasangan Infus (Dr. Ranjan)Document31 pages3 - Teori Pemasangan Infus (Dr. Ranjan)Metha KemalaNo ratings yet
- Map DkaDocument1 pageMap DkaSH PrageethNo ratings yet
- Suxamethonium Atracurium Cisatracurium Pancuronium Vecuronium RocuroniumDocument1 pageSuxamethonium Atracurium Cisatracurium Pancuronium Vecuronium Rocuroniumicen00bNo ratings yet
- Albumin & Total Protein: (Page 1 - ALBUMIN) 4 X 50 ML 11002001Document2 pagesAlbumin & Total Protein: (Page 1 - ALBUMIN) 4 X 50 ML 11002001N. K. MandilNo ratings yet
- SHC ABX Dosing GuideDocument7 pagesSHC ABX Dosing GuideDanielVillaNo ratings yet
- This Study Resource Was: Light Activity 50-60 PercentDocument2 pagesThis Study Resource Was: Light Activity 50-60 PercentAisha MarieNo ratings yet
- SHC ABX Dosing GuideDocument7 pagesSHC ABX Dosing GuideDeena AlJawamisNo ratings yet
- Oneway: ONEWAY RBC BY Perlakuan /statistics Descriptives Homogeneity /missing Analysis /POSTHOC TUKEY ALPHA (0.05)Document4 pagesOneway: ONEWAY RBC BY Perlakuan /statistics Descriptives Homogeneity /missing Analysis /POSTHOC TUKEY ALPHA (0.05)Rani silviaNo ratings yet
- Erba ALBUMIN PDFDocument2 pagesErba ALBUMIN PDFAniket dubeyNo ratings yet
- Household MeasurementDocument4 pagesHousehold MeasurementYna EstabilloNo ratings yet
- Blender Feeding Calulations Worksheet Nutricalcs DraftDocument5 pagesBlender Feeding Calulations Worksheet Nutricalcs DraftHuelang HokageuchihaNo ratings yet
- TBS-CW Basic Version CatalogDocument1 pageTBS-CW Basic Version Catalogphat nguyen minh100% (1)
- Direct Bilirubin ENDocument1 pageDirect Bilirubin ENRakib Hossain 3A-159No ratings yet
- Dosis Pemberian Obat Untuk Di Tempel Di ERDocument6 pagesDosis Pemberian Obat Untuk Di Tempel Di ERHutomo 75No ratings yet
- Bodyfat Calories Macro Energy Calculator - Fredrik Gain v3Document20 pagesBodyfat Calories Macro Energy Calculator - Fredrik Gain v3GellaNo ratings yet
- Pharmaceutical CalculationsDocument8 pagesPharmaceutical CalculationsdrugdrugNo ratings yet
- Electrolytes Policy - April 30Document11 pagesElectrolytes Policy - April 30ElissaNo ratings yet
- Pedia StickersDocument8 pagesPedia Stickersmkct111100% (1)
- GA4256 00 - Direct BilirubinDocument2 pagesGA4256 00 - Direct BilirubinTrần Thanh ViệnNo ratings yet
- OPPANOL® B GradesDocument9 pagesOPPANOL® B GradesAndre SantillanaNo ratings yet
- Bbgrey SheildDocument3 pagesBbgrey Sheildiga.adoleNo ratings yet
- Alat (GPT) Fs : Order Information Materials RequiredDocument6 pagesAlat (GPT) Fs : Order Information Materials RequiredHadi BitarNo ratings yet
- Technical Document - AquaSnap Microbial DetectionDocument1 pageTechnical Document - AquaSnap Microbial DetectionanjukkuttiNo ratings yet
- Naplex - Math FormulasDocument1 pageNaplex - Math FormulasbooseeyNo ratings yet
- Nuclear EnergyDocument25 pagesNuclear EnergyMohab GarawanyNo ratings yet
- General Organic ExerciseDocument2 pagesGeneral Organic ExerciseMohab GarawanyNo ratings yet
- Ap Notes Nuclear RVWDocument53 pagesAp Notes Nuclear RVWMohab GarawanyNo ratings yet
- General Organic ExerciseDocument2 pagesGeneral Organic ExerciseMohab GarawanyNo ratings yet
- Organic Chemistry NotesDocument1 pageOrganic Chemistry NotesMohab GarawanyNo ratings yet
- Grade 9 Biology ProjectDocument2 pagesGrade 9 Biology ProjectMohab GarawanyNo ratings yet
- +egyptian Drug Guide 3rd EditionDocument65 pages+egyptian Drug Guide 3rd Edition2288R100% (1)
- Body Organization 1Document4 pagesBody Organization 1Mohab GarawanyNo ratings yet
- International - Programmes in Austria PDFDocument36 pagesInternational - Programmes in Austria PDFMohab GarawanyNo ratings yet
- Summary of The Psychology of SellingDocument8 pagesSummary of The Psychology of SellingMohab Garawany100% (1)
- DM PDFDocument27 pagesDM PDFMohab GarawanyNo ratings yet
- Must University College of Dentistry GMED 402 FALL 2012 Midterm ExamDocument5 pagesMust University College of Dentistry GMED 402 FALL 2012 Midterm ExamMohab GarawanyNo ratings yet
- Psychiatry Dr. Osama Mahmoud PDFDocument59 pagesPsychiatry Dr. Osama Mahmoud PDFMohab GarawanyNo ratings yet
- Facets of Sneha Murchhana Sanskara A RevDocument8 pagesFacets of Sneha Murchhana Sanskara A RevBhavana GangurdeNo ratings yet
- Aerosol Hair Spray Formulation and Production ProcessDocument7 pagesAerosol Hair Spray Formulation and Production Processhamid eissaNo ratings yet
- Pharma Graphs-1Document22 pagesPharma Graphs-1Aranya BhandaryNo ratings yet
- 118 01881 01 Carbowax Sentry Peg Formulation Guide For CosmeticsDocument4 pages118 01881 01 Carbowax Sentry Peg Formulation Guide For CosmeticsAdriana MariescuNo ratings yet
- Principles and Significance of Professional Ethics. Critical Study of The Code of Pharmaceutical Ethics Drafted by Pharmacy Council in IndiaDocument12 pagesPrinciples and Significance of Professional Ethics. Critical Study of The Code of Pharmaceutical Ethics Drafted by Pharmacy Council in IndiaRahul ThakurNo ratings yet
- SRL Catalogue 2020-21Document288 pagesSRL Catalogue 2020-21akashh1981No ratings yet
- Ok-Kartu Stok Manual (Mutasi Harian) 30062023 NewDocument295 pagesOk-Kartu Stok Manual (Mutasi Harian) 30062023 Newdwi septyaNo ratings yet
- Daftar Obat KemoterapiDocument3 pagesDaftar Obat KemoterapiCharles Nong MakingNo ratings yet
- Advances in Solid Dispersion Techniques For Enhancing Drug Solubility, Bioavailability and Controlled ReleaseDocument5 pagesAdvances in Solid Dispersion Techniques For Enhancing Drug Solubility, Bioavailability and Controlled ReleaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Label Kotak Obat BaruDocument25 pagesLabel Kotak Obat BaruOrin Tri WulanNo ratings yet
- Basic 8 Social Studies 2ND Term E-Note 2017Document19 pagesBasic 8 Social Studies 2ND Term E-Note 2017palmer okiemuteNo ratings yet
- PL Duta 26 Juli 2023Document46 pagesPL Duta 26 Juli 2023Khoridatur RohmahNo ratings yet
- Contoh Pembelian Obat FarmasiDocument70 pagesContoh Pembelian Obat FarmasiapotekbregasNo ratings yet
- Application Number Active Ingredients Trade Name IngredientDocument33 pagesApplication Number Active Ingredients Trade Name IngredientDr-Muhammad Awais ChNo ratings yet
- So Obat-Bmhp All Januari 2019Document191 pagesSo Obat-Bmhp All Januari 2019HabibahNo ratings yet
- Drug Education - G9Document48 pagesDrug Education - G9John Arvie TejanoNo ratings yet
- Recommendations CardiovascularRenal 07.09.2022Document6 pagesRecommendations CardiovascularRenal 07.09.2022Harisankarthekkethil 26No ratings yet
- PBL 513 - Malathion OPDocument19 pagesPBL 513 - Malathion OPAimanRozlanNo ratings yet
- Report RN TGL 07052024Document8 pagesReport RN TGL 07052024Mohamad Zain Mustofa 1902112623No ratings yet
- Effervescent TabletsDocument16 pagesEffervescent TabletsAnkush Bhushan100% (1)
- Prep 24 - Captropil SuspensionDocument3 pagesPrep 24 - Captropil SuspensionThe Dededo NativeNo ratings yet
- Organic Synthesis 3 QP AnsweredDocument9 pagesOrganic Synthesis 3 QP AnsweredmilanaNo ratings yet
- Zebra FishDocument3 pagesZebra FishRatn Deep SinghNo ratings yet
- Tablet CoatingDocument50 pagesTablet CoatingNaufal HanifNo ratings yet
- Exame FMCZDocument44 pagesExame FMCZAnnetNo ratings yet
- Research ArticleDocument4 pagesResearch ArticleJoseph BossaNo ratings yet
- Introduction 2Document5 pagesIntroduction 2saharrmohammed1No ratings yet
- LabelDocument12 pagesLabelDonita Rose CaliwagNo ratings yet
- SPMC ReportDocument6 pagesSPMC ReportArosha RohanapuraNo ratings yet