Download as pdf or txt
You might also like
- Philippines, For The Year. of Notarial Register of MR.: Pilipinas, para Sa Taon. NGDocument1 pagePhilippines, For The Year. of Notarial Register of MR.: Pilipinas, para Sa Taon. NGDexterQ.Tualla100% (1)
- Carly FiorinaDocument9 pagesCarly FiorinasnbtccaNo ratings yet
- 05 JUNE QuestionDocument10 pages05 JUNE Questionkhengmai100% (1)
- Validation Vs QualificationDocument1 pageValidation Vs QualificationKiran ChokshiNo ratings yet
- Ivi-Tec AdmonDocument2 pagesIvi-Tec AdmonNathan-Ross AdamsNo ratings yet
- Term Paper: On A Rising Market Giant of BangladeshDocument46 pagesTerm Paper: On A Rising Market Giant of BangladeshSanjeed Ahamed SajeebNo ratings yet
- Alternative AssessmentDocument5 pagesAlternative AssessmentKaneki KenNo ratings yet
- FORM 11 Accident BookDocument1 pageFORM 11 Accident Bookvidyadhara reddyNo ratings yet
- Saplagio1 Deedn of SaleDocument1 pageSaplagio1 Deedn of SalefrimmsallybanaNo ratings yet
- Paysheet FormatDocument3 pagesPaysheet Formatrohan dixitNo ratings yet
- Atzec MP DITDocument3 pagesAtzec MP DITClaudia SandovalNo ratings yet
- Plantilla Con Formulas V3-1-InTRENADocument7 pagesPlantilla Con Formulas V3-1-InTRENAthaliasotosstNo ratings yet
- Form 29 Accidents RegisterDocument1 pageForm 29 Accidents RegisterNazry TanNo ratings yet
- Adobe Scan 06 Sep 2023Document3 pagesAdobe Scan 06 Sep 2023nokubongamagagula99No ratings yet
- Partnership Chapter 1Document15 pagesPartnership Chapter 1Margie Booc PajaroNo ratings yet
- CS Form No. 34-C Plantilla of Casual Appointment - LGU RegulatedDocument1 pageCS Form No. 34-C Plantilla of Casual Appointment - LGU RegulatedBhabes Belen CreusNo ratings yet
- Form29 - March 2024Document1 pageForm29 - March 2024Pardeep pooniaNo ratings yet
- CONSTRUCTION OF (Name of Project and Location) : DPWH Standard Project BillboardDocument1 pageCONSTRUCTION OF (Name of Project and Location) : DPWH Standard Project Billboardcristian gonzalesNo ratings yet
- Sirsa: Hazards While Transporting 10/we Declare That This Consignment9Document1 pageSirsa: Hazards While Transporting 10/we Declare That This Consignment9jftydcNo ratings yet
- BUENOS AIRES - TUESDAY, MAROH 13, 1883. Udesa - Thestandard - 1883 - 03 - 13Document4 pagesBUENOS AIRES - TUESDAY, MAROH 13, 1883. Udesa - Thestandard - 1883 - 03 - 13ManoloPantalonNo ratings yet
- Injury AnalysisDocument8 pagesInjury AnalysisAkhtar QuddusNo ratings yet
- Nominal Roll For July, 2017Document22 pagesNominal Roll For July, 2017Bamidele AremoNo ratings yet
- New FileDocument3 pagesNew Filesatya8851691224No ratings yet
- CS Form No. 34-C Plantilla of Casual Appointment - LGU RegulatedDocument1 pageCS Form No. 34-C Plantilla of Casual Appointment - LGU Regulatednoreen basmayorNo ratings yet
- Hydraulic Computation TemplateDocument3 pagesHydraulic Computation Templatemihiretu TeferaNo ratings yet
- Summary of Blasting Activity & Explosives Usage Prepared By, Approved ByDocument8 pagesSummary of Blasting Activity & Explosives Usage Prepared By, Approved Bydidi setiawanNo ratings yet
- Pages From Dorman Longs - Handbook For Constructional Engineers - 1895-89Document1 pagePages From Dorman Longs - Handbook For Constructional Engineers - 1895-89Fornvald TamasNo ratings yet
- Backgrounder: Transformative Urban Recovery From COVID-19Document2 pagesBackgrounder: Transformative Urban Recovery From COVID-19Aliya RahmanNo ratings yet
- Altnaharra in SoSDocument1 pageAltnaharra in SoSHotelPRNo ratings yet
- Pc-Hse-Fm 05 Extingusher Inspection RecordDocument2 pagesPc-Hse-Fm 05 Extingusher Inspection RecordM AFZAL YASEENNo ratings yet
- Form 2 - PF NominationDocument2 pagesForm 2 - PF NominationChandrima GhoshNo ratings yet
- Huguenot Family List-1Document17 pagesHuguenot Family List-1elsie zinsseNo ratings yet
- New Document (4) .Ar - enDocument2 pagesNew Document (4) .Ar - enM"MNo ratings yet
- Arrest Affidavit For Miami Beach Police Officer Steven SerranoDocument3 pagesArrest Affidavit For Miami Beach Police Officer Steven SerranoAndreaTorresNo ratings yet
- Fise TerminologiceDocument1 pageFise TerminologiceAna-Maria CemurtanNo ratings yet
- Lgu-Borbon, Cebu: Plantilla of Casual AppointmentsDocument1 pageLgu-Borbon, Cebu: Plantilla of Casual AppointmentsRickyNo ratings yet
- Kseb Senioritylist OldDocument244 pagesKseb Senioritylist Oldhiteshmohakar15No ratings yet
- Adobe Scan 06 Oct 2023Document1 pageAdobe Scan 06 Oct 2023satya8851691224No ratings yet
- Flowchart of Usul Al-FiqhDocument1 pageFlowchart of Usul Al-FiqhImran AliNo ratings yet
- Administrators Screen - Top Secret NWO PDFDocument2 pagesAdministrators Screen - Top Secret NWO PDFCarlo SeixasNo ratings yet
- None - FORM 14 - REGISTER OF LEAVE WITH WAGES FOR THE YEARDocument1 pageNone - FORM 14 - REGISTER OF LEAVE WITH WAGES FOR THE YEARSarvesh Mishra100% (1)
- Año de La Lucha Contra La Corrupcion Y La ImpunidadDocument3 pagesAño de La Lucha Contra La Corrupcion Y La ImpunidadJanina BaldeonNo ratings yet
- CSS Screening Test Challan Form 2023Document1 pageCSS Screening Test Challan Form 2023AdeelBaigNo ratings yet
- Board PosterDocument1 pageBoard PosterEmilda IzhnyNo ratings yet
- 15PG-09-YM - MLO-IBE-001 Rev 2 Mechanical Equipment ListDocument3 pages15PG-09-YM - MLO-IBE-001 Rev 2 Mechanical Equipment Listahmed.pobakrNo ratings yet
- Primary Customer: M M D D Yyyy YyyyDocument5 pagesPrimary Customer: M M D D Yyyy YyyySavita ShNo ratings yet
- UntitledDocument1 pageUntitledRURAL MARKETING ASSOCIATION OF INDIANo ratings yet
- Midsem Notes GrammarDocument4 pagesMidsem Notes GrammarFarid AshaariNo ratings yet
- EIA WarehouseDocument3 pagesEIA WarehouseAnnabella1234No ratings yet
- LotR CSheetDocument4 pagesLotR CSheetColin BraddockNo ratings yet
- Beng & TanDocument1 pageBeng & TanJeck NicdaoNo ratings yet
- Second Floor Plan: Legal ServiceDocument1 pageSecond Floor Plan: Legal ServicePrecious UmingaNo ratings yet
- Client Details:: Date of Previous TestDocument2 pagesClient Details:: Date of Previous TestBradley WainwrightNo ratings yet
- Source Info Bearin GDocument5 pagesSource Info Bearin GbanjoletNo ratings yet
- Ascendit Deus Carlo Carturan SSBDocument1 pageAscendit Deus Carlo Carturan SSBThaïs MarquesNo ratings yet
- CSS MPT 2024 Challan FormDocument1 pageCSS MPT 2024 Challan FormhoorNo ratings yet
- JS Bank Limited: Annexure-ADocument50 pagesJS Bank Limited: Annexure-ASheikh Hasnain AliNo ratings yet
- Birth Doc 137944866561979151033Document1 pageBirth Doc 137944866561979151033The CafeNo ratings yet
- Pt. Multi Karya Engineering: Pt. Riau Andalan Pulp & PapperDocument1 pagePt. Multi Karya Engineering: Pt. Riau Andalan Pulp & PapperImade Subagianta100% (1)
- WPRK Pack Preparation PDFDocument42 pagesWPRK Pack Preparation PDFYusufNo ratings yet
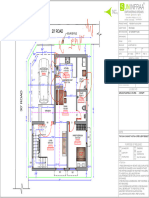
- MR - Ragu Residence GFDocument1 pageMR - Ragu Residence GFAmzathNo ratings yet
- CS Form No. 34-B Plantilla of Casual Appointment - AccreditedDocument3 pagesCS Form No. 34-B Plantilla of Casual Appointment - AccreditedAngelic RecioNo ratings yet
- School Form 1 SF 1 Smaw 11 1 NewDocument8 pagesSchool Form 1 SF 1 Smaw 11 1 NewJOHN BEBON YAPNo ratings yet
- Overall - Jan Site Visit Till 19.05.2024Document253 pagesOverall - Jan Site Visit Till 19.05.2024nithishkumar9443No ratings yet
- Barkatullah University Provisional Migration Degree FormDocument2 pagesBarkatullah University Provisional Migration Degree FormKamleshGolhani100% (3)
- Coco Town Final Layout PlanDocument1 pageCoco Town Final Layout PlanGowthamNo ratings yet
- Model-103 SDS enDocument6 pagesModel-103 SDS enGowthamNo ratings yet
- BDS - Labor - Tariff LatestDocument4 pagesBDS - Labor - Tariff LatestGowthamNo ratings yet
- F 002 A0z 755 Spare PartsDocument17 pagesF 002 A0z 755 Spare PartsGowtham100% (1)
- Delphi Fip NumbersDocument14 pagesDelphi Fip NumbersGowthamNo ratings yet
- Horns & Fanfares BrochureDocument20 pagesHorns & Fanfares BrochureGowthamNo ratings yet
- RedLion RL30E - 2005 PDFDocument12 pagesRedLion RL30E - 2005 PDFEd FalckNo ratings yet
- Case Studies Compilation CA Final (Past Year, MTP & Journal)Document519 pagesCase Studies Compilation CA Final (Past Year, MTP & Journal)Uday BhallaNo ratings yet
- Baroda e GatewayDocument7 pagesBaroda e GatewayRajkot academyNo ratings yet
- Course Collections by Coursera - Digital MarketingDocument11 pagesCourse Collections by Coursera - Digital MarketingJv LozanoNo ratings yet
- 7.elements of A Valid SaleDocument12 pages7.elements of A Valid SaleAnum ShafiqueNo ratings yet
- HRM Questions For PracticeDocument2 pagesHRM Questions For Practicenotes.mcpu80% (5)
- Gs Alliance Sco Rebco Cif Malasia March282021Document2 pagesGs Alliance Sco Rebco Cif Malasia March282021RossFernandez0% (1)
- Sttart Up Company 2012 ArticleDocument5 pagesSttart Up Company 2012 ArticleResearch and Development Tax Credit Magazine; David Greenberg PhD, MSA, EA, CPA; TGI; 646-705-2910No ratings yet
- SOP 3 SOP For EHS LegalDocument6 pagesSOP 3 SOP For EHS LegalRASHA534No ratings yet
- Introduction To Accounting Principles AccountingDocument7 pagesIntroduction To Accounting Principles AccountingAnand PrasadNo ratings yet
- SCL Delay Protocol 2nd Edition PDFDocument85 pagesSCL Delay Protocol 2nd Edition PDFSTNo ratings yet
- Unit CostingDocument3 pagesUnit CostingAnkit YadavNo ratings yet
- Productivity, Output, and EmploymentDocument57 pagesProductivity, Output, and EmploymentMinerva EducationNo ratings yet
- Market Structure Analysis 4Document27 pagesMarket Structure Analysis 4andersonmapfirakupaNo ratings yet
- International Journal of Research Publications Volume-69, Issue-1, January 2021Document29 pagesInternational Journal of Research Publications Volume-69, Issue-1, January 2021Thomas EsguerraNo ratings yet
- Hire Purchase Notes 10 YrDocument80 pagesHire Purchase Notes 10 YrLalitKukreja100% (2)
- eTOM 02 Student Exercises PDFDocument21 pageseTOM 02 Student Exercises PDFSirine KharratNo ratings yet
- 59 FREE CHATGPT PROMPTS (Free Ebook) PDFDocument62 pages59 FREE CHATGPT PROMPTS (Free Ebook) PDFessm14309No ratings yet
- CH1-Developing A Business MindsetDocument40 pagesCH1-Developing A Business Mindsetosama 5xNo ratings yet
- Leading Global Engineering ConsultancyDocument12 pagesLeading Global Engineering Consultancytomc80530% (1)
- Marketing Balaji 111111Document10 pagesMarketing Balaji 111111Hařsh Thakkar HťNo ratings yet
- RFP Sample 1Document17 pagesRFP Sample 1mma23122012No ratings yet
- Pepsi Case AnalysisDocument46 pagesPepsi Case AnalysisSonia KhanNo ratings yet
- Completing The Tests in The Acquisition and Payment Cycle: Verification of Selected AccountsDocument32 pagesCompleting The Tests in The Acquisition and Payment Cycle: Verification of Selected AccountsNhung KiềuNo ratings yet