Professional Documents
Culture Documents
A&P Study Guide Test 3
A&P Study Guide Test 3
Uploaded by
meaghan22150 ratings0% found this document useful (0 votes)
2 views25 pagesCopyright
© © All Rights Reserved
Available Formats
PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
Download as pdf or txt
0 ratings0% found this document useful (0 votes)
2 views25 pagesA&P Study Guide Test 3
A&P Study Guide Test 3
Uploaded by
meaghan2215Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
Download as pdf or txt
You are on page 1of 25
CHAPTER 22 Lymphatic System and Immunity
1. Immunity: Resistance/ability to ward off damage/disease through defenses
1. Innate/Nonspecific: defenses present at birth, not specific, acts against almost all microbes
the same way; Components: physical and chemical barriers (Skin, mucous membranes),
second line of defense= antimicrobial substances, NK cells, phagocytes, inflammation, fever
2. Adaptive (specific): Involve specific recognition of microbe once it has breached innate
immunity defenses. Adapts/adjusts to handle specific microbe w/lymphocytes (T&B)
--Pathogens: Disease producing microbes
2. COMPONENTS of the Lymphatic/Lymphoid System:
1. Lymph, Lymphatic vessels (transport lymph), Lymphatic tissues (in organs), RBM.
2. Assists in circulating body fluids and helps defend the body against disease-causing agents.
3. Lymph: After bl plasma is filtered through capillaries into interstitial fluid, it passes into
lymphatic vessels and is known as Lymph. Only difference is location: Interstitial (between
cells), lymph (w/n lymphatic vessels and tissues)
4. Lymphatic Tissue: specialized form of reticular conn tissue w/large numbers of
lymphocytes.
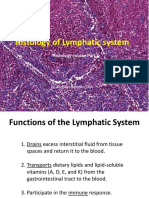
3. FUNCTIONS:
1. Drains excess interstitial fluid: from tissue spaces, return it to blood, maintains bl vol
2. Transports dietary lipids: Lipids and lipid soluble vitamins (A, D, E, K) from GI
3. Carries out immune responses: specific, directed against microbes or abnormal cells
4. Returns lost plasma proteins to blood
4. LYMPHATIC CAPILLARIES & VESSELS
Located in spaces btn cells, *closed at one end*, combine to form lymphatic vessels
1. Lymphatic vessels: resemble veins but have thinner walls and more valves. At intervals
lymph flows through lymph nodes (encapsulated organs consisting of masses of B and T
cells. Vessels lie in subcutaneous tissue in skin, follow veins. In viscera, follow arteries and
form plexuses around them.
2. NO LYMPH CAPILLARIES: Avascular tissues (cartilage, epidermis, cornea), portions of
spleen, RBM
3. Differences from Blood Capillaries:
1. Greater permeability: can absorb large proteins and lipids
2. Larger in diameter
3. One-way structure: allows interstitial fluid to flow in but not out
4. Endothelial cells: Make up walls of capillaries, overlap in L Cap, separate slightly
when pressure is greater in interstitial fluid than in lymph to allow interstitial fluid to
enter. When pressure is greater in L Cap, cells adhere more closely and lymph cannot
escape into interstitial fluid. Further down capillary, pressure is relieved.
5. Anchoring filaments: Attached to L Cap, contain elastic fibers that extend from L Cap
and attach L Endothelial cells to surrounding tissues. If excess interstitial fluid causes
swelling, anchoring filaments are pulled making openings btn cells even larger to allow
more fluid to enter lymphatic capillary
6. Lacteals: In S Int, carry dietary lipids into lymphatic vessels and ultimately into blood.
Presence causes lymph draining from S Int to be creamy white chyle juice. Elsewhere is
typically clear, pale-yellow.
5. LYMPH TRUNKS AND DUCTS
1. Lymph Trunks: Lymphatic vessels exiting lymph nodes unite to form these. (Lumbar,
Intestinal, Bronchomediastinal, Subclavian, Jugular)
1. Lumbar Trunks: drain lymph from lower limbs, wall and viscera of pelvis, kidneys,
adrenal glands, ambdominal wall.
2. Intestinal Trunk: Drains lymph from stomach, intestines, pancreas, spleen, part of liver
3. Bronchomediastinal: thoracic wall, lung, heart
4. Subclavian: upper limbs
5. Jugular: head and neck
2. FLOW OF LYMPH: Lymphatic capillaries to junction of Internal Jugular vein and
Subclavian vein.
**Differs on right and left:
R: 3 lymph trunks (jugular, subcl, broncho) open independently into venous system on
anterior surface of the junction of the internal jugular and subclavian veins.
L: Largest lymph vessel (thoracic/left lymphatic duct) forms main duct for return of
lymph to blood. Begins as dilation of cisterna chyli (receives from lumbar+Interstitial
trunks, in neck from L jugular and L subclavian) opens into anterior surface of junction
of L internal jugular and subclavian
**Lymph from upper R quadrant returns to SVC from R brachiocephalic vein, Lymph
from upper L side and the rest of the body returns to SVC via L brachiocephalic vein**
--Excess filtered fluid drains into lymphatic vessels and becomes lymph. Proteins that can't
return to blood due to concentration gradient can move readily through L Cap into lymph.
1. Bl Capillaries (blood) → Interstitial Spaces (interstitial fluid) → L Cap (Lymph)
2. L Cap (lymph) → L Vessels (lymph) → L Trunks/Ducts (lymph) → junction of internal
jugular & Subclavian veins (Blood)
**Flow is assisted by respiratory pump and skeletal muscle pump**
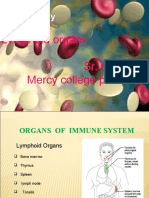
6. LYMPHATIC ORGANS AND TISSUES
Primary: Sites where stem cells divide and become immunocompetent (capable of
mounting and immune response) (RBM, Thymus) Pluripotent in RBM → B and pre-T, pre-
T become T cells in Thymus.
Secondary: Sites where immune responses occur. Lymph nodes, spleen, lymphatic nodules
(follicles)
**Thymus, spleen, L nodes are organs bc have conn tissue capsule, L nodules don't and are
tissues
1. THYMUS: Bilobed organ in mediastinum btn sternum and aorta
--Enveloped by conn tissue, capsule of conn tissue encloses each lobe separately. Capsule
has extensions called trabeculae that penetrate inward and divide each lobe into lobules.
--Reddish appearance due to lymphoid tissue and bl supply. Age can make fatty infiltrations
replace lymphoid tissue and make it more yellow and look smaller but size doesn't change.
(Starts as thymic, at puberty replace this w/adipose and areolar conn tiss and continues to
atrophy but before it does so it populates other 2nd L organs & tissues w/T cells.)
1. Lobules: Consist of deeply staining outer cortex and lighter staining medulla
1. Cortex: Composed of large numbers of T cells and scattered dendritic cells,
epithelial cells, and macrophages. Immature T cells from RBM migrate here,
proliferate, and mature.
1. Dendritic Cells: Derived from monocytes, have long branched projections that
resemble dendrites of a neuron. Assist in maturation of T cells and immune resp
2. Epithelial Cells: Have several long processes surrounding and serving as a
frame for <50 T cells. “Educate” the pre-T cells through positive selection,
produce thymic H thought to aid in maturation of T cells. Only 2% of T cells
survive development in cortex, others undergo apoptosis and are cleared by
Thymic Macrophages. Surviving T cells enter medulla.
2. Medulla: Widely scattered, more mature T cells, epithelial, dendritic, macrophages.
1. Thymic/Hassall's Corpuscles: Epithelial become arranged in concentric layers
of flat cells that denegrate and fill w/keratohyalin granules and keratin. Role is
uncertain but may be site of T cell death in medulla.
2. T cells that leave thymus via bl migrate to L nodes, spleen, L tissues & colonize
2. Lymph Nodes: 600 scattered throughout the body superficially and deeply in groups. Lots
of them near mammary glands and in axillae and groin.
--Function as a filter: Foreign substances are trapped by reticular fibers w/n sinuses of node,
macrophages destroy some foreign substances, lymphocytes destroy some, and then the
filtered lymph leaves the other side.
--Covered w/capsule of conn tissue that extends into node as trabeculae that divide node
into compartments, provide support, and provide route for bl vess into interior of node.
--Internal to capsule is supporting network of reticular fibers & fibroblasts that (along
w/trabeculae) form stroma (supporting framework of conn tissue)
--Parenchyma: The functioning part of a lymph node
1. Superficial Cortex: Outer and Inner
1. Outer Cortex: consists of egg-shaped aggregates of B cells (lymphatic
nodules/follicles)
1. Primary lymphatic nodule: Consists of primarily B cells. Once these
recognize an antigen, they develop into 2nd L nodule
2. Secondary lymphatic nodule: (Majority) form in response to antigen and
are site of plasma cell and memory B cell formation.
--Center contains region of light-staining cells called germinal center that
consists of B cells, follicular dendritic cells, macrophages.
--Follicular dendritic cells present an antigen and B cells proliferate and
develop into antibody-producing plasma cells or memory B cells.
--Memory B cells persist after initial immune response and remember
encountering specific antigen. If they do not develop properly, macrophages.
--Region surrounding germinal center is composed of dense accumulations
of B cells that have migrated away from site of origin w/n nodule.
2. Inner/Deep Cortex: No L Nodules. Mainly T cells and dendritic cells that enter
a L node from other tissues.
--Dendritic Cells: present antigens to T cells & cause their proliferation. Newly
formed T cells then migrate from L node to areas of body w/antigenic activity
1. Medulla: B cells (antibody-producing plasma cells that have migrated out of
cortex into medulla) and macrophages both embedded in network of reticular
fibers and reticular cells.
2. Afferent L Vessels: Lymph enters through these which penetrate convex surface of
the node at several points. Contain valves that open toward the center of the node,
directing lymph inward to sinuses.
3. Sinuses: w/n L node, are a series of irregular channels that contain branching
reticular fibers, lymphocytes, and macrophages.
1. Subcapsular Sinus: Directly after afferent L Vess, immediately beneath capsule.
2. Trabecular Sinuses: These extend through cortex parallel to trabeculae
3. Medullary Sinusees: Extend throughout medulla, drain into efferent L Vess
4. Efferent L Vessels: Wider and fewer in number than afferent vess, contain valves
that open away from center of L node to convey lymph, antibodies from plasma
cells, and activated T cells out of the node. Emerge from slight depression on lymph
node called Hilum where bl vess also enter and leave the node.
**Many afferent and few efferent means that flow of lymph is slow through node
and this allows time for filtration and exposure to multiple filtering events before
returning to blood.**
7. THE SPLEEN
Largest mass of lymphatic tissue in the body. Located between stomach and diaphragm.
--Superior surface is smooth & convex
--Gastric impression: stomach indents it; renal impression (kidney); colic impression (L colic
flexure of L intestine)
--Surrounded by dense conn tiss covered by serous mem
1. Hilum of spleen (slight depression) is where splenic artery, s vein, and efferent l vess pass.
2. Stroma: capsule plus trabeculae, reticular fibers, fibroblasts
3. Parenchyma of the spleen:
1. White pulp: lymphatic tiss of mostly lymphocytes and macrophages arranged around
branches of central arteries (splenic artery)
2. Red pulp: blood filled venous sinuses and cords of splenic tissue called splenic
cords/Billroth's cords that consist of RBC, macrophages, lymphocytes, plasma cells,
and granulocytes. Veins are closely associated w/red pulp
4. FUNCTIONS:
1. Bl flowing into spleen through splenic artery enters central arteries of w. pulp.
2. In w pulp, B and T cells carry out immune functions while spleen macrophages destroy
blood-borne pathogens by phagocytosis.
3. Red pulp
1. Macrophages remove ruptured/worn out/damaged RBC and platelets
2. Stores platelets (up to 1/3 body's supply)
3. Hemopoiesis (produces RBC) during fetal life
8. LYMPHATIC NODULES (Mucosa Associated Lymphatic Tissue (MALT))
–Egg-shaped masses of lymphatic tissue w/o a capsule. Scattered in lamina propria (conn tiss)
of mucous mem lining of GI, urinary, reproductive, respiratory airways.
--Can be small and solitary or large aggregations:
1. Peyer's Patches (aggregated lymphatic follicles in ileum of s intestine)
2. Appendix has aggregates
3. Tonsils form ring at junction of oral cavity/oropharynx and nasal cavity/nasopharynx
1. Pharyngeal (adenoid): embedded in posterior wall of nasopharynx
2. Palatine: 2 at posterior region of oral cavity, one on either side, commonly removed
3. Lingual: 2 at base of tongue, also may be removed
9. INNATE IMMUNITY: (nonspecific): Includes external and chemical barriers of the skin and
mucous membranes as well as internal defenses like antimicrobial substances, NK cells,
phagocytes, inflammation, fever
1. First Line of Defense: Skin and Mucous Membranes
1. Epidermis: Layers of packed keratinized squamous cells are physical barrier to
microbes, shedding removes microbes from surface, only get in rarely or if broken.
Acidity is caused by secretion of fatty acids and lactic acid
2. Mucous Mem: epithelial layer secretes lubricating mucus that moistens and is viscous
enough to trap microbes and foreign substances. Swollowing mucus sends pathogens to
stomach to be destroyed
1. Hair: in nose, traps and filters microbes, dust, pollutants
2. Cilia: upper respiratory tract, waving action propells dust, microbes that were
inhaled to throat. Coughing and sneezing enhance this.
3. Lacrimal Apparatus: eyes, manufactures tears in response to irritants. Blinking spreads
them over entire eye, continual washing like this dilutes microbes and keeps them from
steeling on the eye. Tears contain lysozyme (breaks down cw of bacteria)
4. Saliva: mouth, functions like tears. Lysozyme here and in perspiration, nasal secretions,
tissue fluids and they work similarly.
5. Urine: flow cleanses urethra and retards colonization
6. Vaginal Secretions: Slightly acidic, discourages bacterial growth, flushes bact out
7. Defecation: Lower GI tract can contract rapidly causing diarrhea in response to toxins
8. Vomiting
9. Sebum: oily secretion of sebaceous glands forms protective film over skin. Unsaturated
acids in sebum inhibit growth of certain pathogenic bacteria and fungi.
10. Gastric juice: Hydrochloric acid, enzymes, mucus; acidity destroys bacteria and toxins
2. Secondary Line of Defences: Internal Antimicrobial substances, phagocytes, NK cells,
inflammation, fever
1. Antimicrobial Substances:
1. Inerferons (IFNs): produced by lymphocytes, macrophages, fibrobalsts infected
w/viruses. Once released, IFNs diffuse to uninfected neighboring cells where the
induce synth of antiviral prot that interfere w/viral replication. Do not prevent
attachment but prevent replication. 3 kinds (Alpha, Beta, Gamma)
2. Complement System: Normally inactive proteins in bl plasma and on p mem.
When activated, complement or enhance certain immune reactions. Causes cytolysis
(bursting) of microbes, promotes phagocytosis, contributes to inflammation.
3. Iron-Binding Proteins: Inhibits growth of certain bacteria by reducing available
amount of iron. Includes transferrin (bl and tissue fluids), lactoferrin (milk, saliva,
mucus), ferritin (liver, spleen, RBM), hemoglobin (RBC)
4. Antimicrobial proteins (AMPs): Short peptides w/broad spectrum of antimicrobial
activity. Kill wide range of microbes, attract dendritic cells and mast cells. Microbes
do not seem to develop resistance. Examples: dermicidin (sweat glands),
defensins/cathelicids (neutrophils, macroph, epithelia), thrombocidin (platelets).
2. Natural Killer Cells and Phagocytes: Next defense after skin/mucous mem,
antimicrobial substances in blood.
1. NK Cells: Found in blood, spleen, l nodes, RBM. Lack membrane molecules that ID
them like B&T Cells have, can kill wide variety of infected cells and tumors, attack
body cells that display abnormal/unusual p mem properties
--Binding to target cells releases granules that may contain:
1. Perforin: protein that inserts into p mem and causes perforations in mem
causing cytolysis
2. Granzymes: protein digesting enzymes that induce target cell to undergo
apoptosis. Kills infected cells but not microbes inside which are released and
may or may not be intact.
2. Phagocytes: phagocytosis of microbes or particles like cellular debris. Both innate
and adaptive immunity.
1. Neutrophils: First to the site of infection
2. Macrophages: Come to the site as monocytes, during migration enlarge and
develop into actively phagocytic wandering macrophages. Others are fixed
macrophages that guard specific tissues (histocytes: conn tiss; stellate
reticuloendothelial cells/Kupffer cells: liver; alveolar macrophages: lungs;
microglial cells: nervous system; tissue macrophages: spleen, l nodes, RBM
Five stages of phagocytosis:
1. Chemotaxis: chemically stimulated movement to site of damage. May come
from microbes, WBC, damaged tissue cells, activated complement proteins
2. Adherence: Attachment to the microbe/foreign material. Binding of
complement proteins to the pathogen enhances adherence
3. Ingestion: P mem of phagocyte exteneds pseudopods (projections) that
engulf the microbe (ingestion). When pseudopods meet, they fuse and
surround microorganism in sac called a phagosome.
4. Digestion: Phagosome enters cytoplasm and merges w/lysosomes to form
single larger phagolysosome. Lysozyme breaks down c w and other
digestive enzymes degrade carbs, prot, lipids, nuc acids. Phagocyte also
forms lethal oxidants (superoxide anion (O2-), hyperchlorite anion (OCl-),
hydrogen peroxide (H2O2) in process called oxidative burst.
5. Killing: Chemical onlaught kills many types of microbes. Any that cannot be
degraded remain in residual bodies.
3. Inflammation: nonspecific defensive response to tissue damage. May be caused by
pathogens, abrasions, chemical irriations, disortion/disturbances of cells, extreme temps
--Works as an attempt to dispose of microbes, toxins, foreign material at site of injury,
prevent their spread to other tissues, and prepare site for tissue repair in attempt to
restore homeostasis.
--Response is the same for a cut, burn, radiation, bacteria/virus
Signs and symptoms: PRISH
1. Pain due to release of certain chemicals
2. Redness because more blood is rushed to affected area
3. Immobility from some loss of function in sever inflammation
4. Swelling caused by accumulation of fluids
5. Heat due to more blood in affected area
(1) Vasodiation, increased permeability of blood vess (2) Emigration of phagocytes from
blood to interstitial fluid (3) Tissue repair
10. Adaptive Immunity: Ability of the body to defend itself against specific invading agents such
as bacteria, toxins, viruses, foreign tissues.
Antigens (Ags): (Antibody generators) Substances recognized as foreign and provoke
immune response.
Distinguished from innate because: (1) Specificity for particular foreign molecules
(antigens) involves distinguishing self from nonself. (2) Memory for most previously
encountered antigens so that second encounter prompts even more rapid/vigorous response.
Immunology: Study of the responses of the body when challenged with antigens.
Immune system: cells and tissues that carry out immune response
1. B and T cells: develop from primary lymphatic organs (RBM, thymus) from pluripotent
stem cells that originate in RBM. B matures in RBM, T migrate to thymus to mature.
1. T cells: Helper T cells (CD4), Cytotoxic T cells (CD8)
CHAPTER 23: THE RESPIRATORY SYSTEM
1. Steps of respiration:
1. Pulmonary ventilation: (breathing) inhalation (allows O2 to enter lungs) and exhalation
(permits CO2 to exit lungs) involving exchange of air btn atmosphere and alveoli of lungs.
2. External (pulmonary) respiration: exchange of gases btn alveoli and bl in pulmonary
capillaries across respiratory membrane. Blood gains O2 and loses CO2
3. Internal (tissue) respiration: exchange btn bl in systemic capillaries and tissue cells. Bl
loses O2 and gains CO2. Cells metabolic reactions consume O2 and give off CO2 during
cellular respiration for the production of ATP
2. COMPONENTS of the respiratory system (Studies by otorhinolaryngology)
Structural components:
1. Upper respiratory system: nose, nasal cavity, pharynx, associated structures
2. Lower respiratory system: larynx, trachea, bronchi, lungs
Funtional Componenets:
1. Conducting zone: series of interconnecting cavities and tubes outside and within lungs
(nose, nasal cavity, pharynx, larynx, trachea, bronchi, bronchioles, terminal bronchioles)
--Funtion: Filter, warm, moisten air and conduct it to the lungs
2. Respiratory zone: tubes and tissues w/n the lungs where gas exchange occurs.
(respiratory bronchioles, alveolar ducts, alveolar sacs, alveoli)
--Function: Main sites of gas exchange between air and blood
3. FUNCTIONS of the respiratory system:
(1) Gas exchange, (2) regulation of pH, (3) sense of smell (4) filtration of inhaled air (5)
phonation (vocal sounds) (6) excretion of small amounts of water and heat
4. UPPER RESPIRATORY SYSTEM:
Ciliated cells move mucus and trapped particles DOWN to pharynx
1. Nose: specialized organ at entrance of respiratory system
1. External Nose: visible on face, supporting bony framework (frontal bone, nasal bones,
maxillae) and cartilaginous framework (hyaline cartilage pieces connected to ea other
and some skull bones by fibrous conn tiss) covered w/muscle and skin and lined
w/mucous mem.
--External nares (nostrils): lead into cavities called nasal vestibules
Cartilaginous framework:
1. Septal nasal cartilage: anterior portion of nasal septum
2. Lateral nasal cartilages: inferior to nasal bones
3. Alar cartilages: form portion of walls of nostrils.
FUNCTIONS: (1) warm, moisten, filter air (2) detect olfactory stimuli (3) modify
speech vibrations. (resonance: amplifying, prolonging, modifying sound vibration)
2. Internal Nose (Nasal Cavity): large space in anterior aspect of skull inferior to nasal
bone, superior to oral cavity. Lined w/mucous mem.
--Divided by nasal septum: anterior portion of septum is hyaline cartilage, remainder is
formed by vomer and perpendicular plate of ethmoid, maxillae, palatine bones.
--Anteriorly merges w/external lose and posteriorly communicates w/pharynx through
internal nares (choanae).
--Ducts from paranasal sinuses (drain mucus) and nasolacrimal ducts (drain tears)
open into nasal cavity. Paranasal sinuses are cavities continuous w/lining of nasal cavity
and also serves as resonating chambers.
--Bony and cartilaginous framework of nose helps keep nose patent (open,
unobstructed)
1. Respiratory Region: Inferior portion of nasal cavity, lined with respiratory
epithelium: ciliated pseudostratified columnar epithelium, numerous goblet cells
2. Olfactory Region: Smaller, superior portion.
3. Nasal vestibule: anterior portion of nasal cavity surrounded by cartilage, superior
portion of nasal cavity is surrounded by bone.
3. Passage of Air:
1. Vestibule: lined w/skin containing coarse hairs that filter dust
2. Superior, middle, inferior conchae: extend out of each lateral wall of n cavity
3. Superior, middle, inferior nasal meatuses: conchae subdivide each side of nasal
cavity forming these groovelike air passages
**Conchae and meatuses increase surface area and prevent dehydration by trapping
water droplets during exhalation**
--Air in meatuses and conchae whirls around and is warmed by blood in capillaries.
--Mucus secreted by goblet cells moistens air and traps dust, drainage from
nasolacrimal ducts also moistens air and sometimes secretions from paranasal
sinuses help, too.
--Cilia move mucus and trapped dust toward pharynx to be swallowed or spit out
4. Olfactory epithelium: Cilia, olfactory receptor cells, supporting cells, and basal
cells are found here in superior nasal conchae and adjacent septum. NO goblet cells
2. PHARYNX (throat): funnel shaped tube from internal nares to level of cricoid cartilage
(inferior cartilage of larynx). Posterior to nasal/oral cavities, superior to larynx, anterior to
cervical vertibrae.
--Composed of skeletal muscles, lined w/ mucous mem. Relaxed sk muscle keep pharynx
patent (open). Contraction assists in deglutition (swallowing).
--Functions as a passage for air and food, resonating chamber for speech, houses tonsils
1. Nasopharynx: posterior to nasal cavity, extends to soft palate which forms posterior
portion of roof of the mouth (serves as muscular partition btn nasopharynx and
oropharynx)
--Five openings: 2 internal nares, 2 lead into audiotory (pharyngotympanic) tubes,
one opens into oropharynx.
--Posterior wall also contains pharyngeal tonsil (adenoid)
--Receives air through internal nares and nasal cavity along w/packages of dusty mucus,
moves dust to inferior part, exchanges small amounts of air w/auditory tubes to equalize
pressure btn middle ear and atmosphere
--Lined w/ciliated pseudostratified columnar epithelium.
2. Oropharynx: Intermediate portion, posterior to oral cavity, extends from soft palate
inferiorly to level of hyoid bone.
--Fauces: opening of oropharynx from the mouth.
--Functions in both respiration and digestion (passage for air, food, drink)
--Nonkeratinized stratified squamous epithelium
--Palatine and lingual tonsils are found here
3. Laryngopharynx (hypopharynx): Inferior portion, begins at level of hyoid bone,
inferiorly opens into esophagus posteriorly and larynx anteriorly.
--Both respiratory and digestive functions
--Nonkeratinized stratified squamous epithelium
5. LOWER RESPIRATORY SYSTEM
Ciliated cells move dust and trapped particles UP toward pharynx
1. LARYNX: Short passageway connecting laryngopharynx with trachea in midline of neck,
anterior to esophagus and 4-6 cervical vertibrae.
--Superior to vocal folds: Nonkeratinized stratified squamous epithelium.
--Inferior to vocal folds: pseudostratified columnar epithelium made up of ciliated columnar
cells, goblet cells (mucus), basal cells
--Extrinsic muscles of larynx connect cartilages to other structures in throat, intrinsic
connect cartilages to one another.
--Cavity of the larynx: Space extending from entrance into larynx down to inferior border
of cricoid cartilage
--Laryngeal vestibule: Portion of cavity of larynx above vestibular folds (false vocal cords)
--Infraglottic cavity: portion of cavity of larynx below vocal folds
9 Pieces of Cartilage
1. Singular cartilages:
1. Thyroid cartilage (Adam's apple): 2 fused plates of hyaline cartilage that form
anterior wall of larynx, give triangular shape. Present in M and F but larger in M due
to sex hormones. Thyrohyoid membrane connects t cartilage to hyoid bone
2. Epiglottis: Large, leaf shaped piece of elastic cartilage covered w/epithelium.
“Stem” is tapered inferior portion attached to anterior rim of thyroid cartilage.
“Leaf” is broader superior portion unattached and moves up and down, elevation of
pharynx/larynx during swallowing widening pharynx and raising larynx causing
epiglottis to move down and form lid over glottis (pair of folds of mucous mem,
vocal folds (true vocal cords), and space between them rima glottidis).
--Keeps liquids and foods out of larynx/airways. Cough reflex
3. Cricoid cartilage: Ring of hyaline cartilage forming inferior wall of larynx.
Attached to first ring of cartillage of trachea by cricotracheal ligaments and
connected to thyroid cartilage by cricothyroid ligament.
--Functions as landmark for making emergency airway (tracheotomy)
2. Paired cartilages:
1. Arytenoid: Triangular pieces of mostly hyaline cartilage in posterior superior border
of cricoid cartilage. Form synovial joints w/cricoid cartilage, wide range of mobility.
--Most important because influence changes in position and tension of vocal folds
(true vocal cords) for speech.
2. Cuneiform: cube-shaped elastic cartilage anterior to cornicunate, support vocal
folds and lateral aspects of epiglottis
3. Corniculate: Horn-shaped pieces of elastic cartilage located in apex of each
arytenoid cartilage.
3. UNKNOWN OTHER 3?
2. VOICE PRODUCTION:
1. Vestibular Folds (False vocal cords): Superior fold of larynx mucous mem. Do not
function in voice production, but when brought together function in holding breath
against pressure of thoracic cavity.
1. Rima Vestibuli: Space between the vestibular folds
2. Vocal Folds (True vocal cords): Inferior fold of larynx mucous mem. Principal
structures of voice production. Made up of m mem of nonkeratinized strat squam
epithelium, deep to this are bands of elastic ligaments stretched btn rigid cartilages of
larynx like strings on a guitar.
--Intrinsic laryngeal muscles attach to cartilages and v folds and when contracted, causes
cartilages to move, elastic ligaments to tighten, v folds to stretch, rima glottidis to
narrow. Variation in pitch is due to tension on folds.
3. Laryngeal Ventricle: lateral expansion of middle portion of laryngeal cavity inferior to
vestibular folds and superior to vocal folds.
3. TRACHEA (Windpipe): tubular passageway for air anterior to esophagus, extends from
larynx to superior border of 5th thoracic vertebra where it divides into R and L pulmonary
bronchi.
LAYERS of the TRACHEA
1. Mucosa: Epithelial layer of ciliated pseudostratified columnar epithelium, underlying
layer of lamina propria with elastic and reticular fibers
--Provides protection against dust and particulates
2. Submucosa: areolar conn tiss with seromucous glands and their ducts
3. Hyaline Cartilage: 16-20 incomplete horizontal rings stacked on above the other
connected by dense conn tissue.
--Open part of each C-ring faces posteriorly toward esophagus and is spanned by
fibromuscular membrane.
--Fibromuscular mem contains transverse sm muscle fibers (trachealis muscle) and
elastic conn tiss that allow diameter of trachea to change subtly during inhalation and
exhalation (maintains efficient airflow).
--Solid curve of C-ring providessemirigid support to maintain patency (stops tracheal
wall from collapsing inward during inhalation and obstructing airway).
4. Adventitia: Areolar conn tiss that joins trachea to surrounding tissues
4. BRONCHIAL TREE
Extensive branching from tracea through terminal bronchioles resembling inverted tree.
First Generation
1. Right Main (Pulmonary) Bronchus: Goes to R lung, more vertical, shorter, wider than
L, more likely to have aspirated object enter this side.
2. Left main (Pulmonary) Bronchus: Goes to L lung
--Both bronchi contain incomplete rings of cartilage and are lined by ciliated
pseudostratified columnar epithelium
**M MEM: ciliated pseudostratified columnar epithelium
3. Carina: Internal ridge where trachea divides into R and L Main Bronchi. Formed by
posterior kinda inferior projection of last tracheal cartilage.
--M mem is most sensitive area of entire larynx and trachea for triggering cough reflex
--Widening and distortion can indicate carcinoma of l nodes around this region
ENTER LUNGS; Second Generation
1. Lobar (secondary) Bronchi: smaller, one for each lung.
**M MEM: ciliated pseudostratified columnar epithelium
2. Segmental (tertiary) Bronchi: branches of secondary, supply specific
bronchopulmonary segments w/n th lobes. (third generation)
**M MEM: ciliated pseudostratified columnar epithelium
3. Bronchioles: Divisions of tertiary, branch repeatedly (4-22 generations)
**M MEM: ciliated simple columnar epithelium w/some goblet cells in larger bronc,
ciliated simple cuboidal epithelium w/o goblet cells in smaller bronchioles
4. Terminal bronchioles: Smallest divisions of bronchioles (23rd generation)
--Club (Clara) Cells: columnar nonciliated cells interspersed among terminal
bronchiole epithelial cells. May (1) protect against harmful effects of inhaled
toxins/carcinogens, (2) produce surfactant, (3) function as stem cells (reserve cells)
that give rise to epithelial cells.
--These are the end of the conducting zone of respiratory system, branches beyond
these become microscopic and called respiratory bronchioles and alveolar ducts
**M MEM: nonciliated simple cuboidal epithelium
--Mucus from goblet cells traps particles, cilia moves it, w/o cilia particles are removed via
macrophages
--Plates of cartilage gradually replace incomplete rings of cartilage in main bronchi and
disappear in distal bronchioles
--As cartilage decreases, sm muscle increases and encircles lumen in spiral bands. Helps
maintain patency, but w/o cartilage muscle spasms can close airways (asthma)
STIMULATION
1. Sympathetic: ANS increases during exercise and adrenal medulla releases
epinephrine, norepinephrine. This relaxes sm muscle in bronchioles, dilates airways,
air reaches lungs quickly, ventilation improves.
2. Parasympathetic: ANS and mediators of allergic reactions (histamine) cause
contraction of bronchiolar sm muscle and causes constriction of distal bronchioles
6. LUNGS: paired, cone-shaped organs in thoracic cavity separated from each other by the heart
other structures in mediastinum so that trauma to one lung doesn't damage the other's ability to
expand.
1. Pleural Membrane (Pleura): double-layered serous membrane that surrounds each lung
1. Parietal Pleura: First layer, lines wall of thoracic cavity
2. Visceral Pleura: Second layer, covers the lungs
3. Pleural Cavity: between the two pleura layers, contains lubricating fluid secreted by the
membranes that reduces friction allowing easy movement while breathing AND causes
two membranes to adhere to one another due to surface tension (like water and slides)
**Lungs do not completely fill cavity, so excess fluid can be removed via thoracentesis
Pleurisy (Pleuritis): inflammation of the pleural mem that can cause friction btn pleura
Pleural effusion: excess fluid accumulated in pleural space
2. Base: Broader inferior portion of lung, concave, fits over convex area of the diaphragm
3. Apex: Narrow superior portion of lungs, lies superior to medial third clavicles and is the
only area that can be palpated.
4. Costal surface: Surface of lungs lying against the ribs and matching their curve
5. Mediastinal (medial) surface: contains a region (hilum) through which bronchi,
pulmonary bl vess, lymphatic vess, and nerves enter and exit. Held together by pleura and
conn tiss and constitute the root of the lung.
6. Cardiac notch: concavity in the L lung in which apex of the heart lies. Because of this, L
lung is 10% smaller than R lung. R lung is thicker, broader, and shorter (bc diaphragm is
higher on R side to accommodate the liver)
7. FISSURES AND LOBES
Fissures: divide each lung into lobes.
1. Oblique fissure: In both lungs, extends inferiorly and anteriorly
1. In L lung, separates superior lobe from inferior lobe
2. In R lung, superior part of oblique fiss separates superior lobe from inferior lobe,
inferior part of oblique fiss separates inferior lobe from the middle lobe which is
bordered superiorly by horizontal fissure.
2. Horizontal fissure: In R lung
--Each lobe receives its own lobar bronchus.
1. R main bronchus gives rise to superior, middle, inferior lobar bronchi
2. L main bronchus gives rise to superior and inferior lobar bronchi
Lobar bronchi give rise to segmental bronchi (10 in each lung) that supply their
respective portions of lung tissue called a bronchopulmonary segment
LOBULES: Bronchopulmonary segments have smaller compartments called
lobules that are each wrapped in elastic conn tissue and contain a lymphatic vessle,
an arteriole, venule, and a branch from a terminal bronchiole.
--Respiratory bronchioles: microscopic branches from the subdivision of
terminal bronchioles and lobules. They have alveoli budding from walls that
participate in gas exchange so respiratory bronchioles begin the respiratory zone.
--Res bronch have an epithelial lining changes from simp cuboidal to simp
squam and divide into alveolar ducts that consist of simple squamous epithelium.
8. ALVEOLAR SACS AND ALVEOLI
Alveolar sac: terminal dilation of an alveolar duct analagous to a cluster of grapes.
1. Alveoli: outpouching of alveolar sac analagous to the individual grapes. Account for
spongy texture. Walls of ea alveolus (singular) consists of two types of epithelial cells:
1. Type I alveolar (squamous pulmonary epithelial) cells: simple squamous
epithelial cells that form nearly continuous lining of alveolar walls. Majority. Thin,
main sites of gas exchange. Have elastic basement mem underlying them.
2. Type II alveolar cells (septal cells): fewer, found between type I. Rounded/cuboidal
--Free surfaces contain microvilli
--Secrete alveolar fluid that keeps surface btn cells and air moist and contains
surfactant: complex mixture of phospholipids and lipoproteins that lowers surface
tension of alveolar fluid thereby reducing tendency of alveoli to collapse and thus
maintains their patency.
3. Alveolar macrophages (dust cells): Also in alveolar walls, remove fine dust
particles and other debris from alveolar spaces.
4. Fibroblasts: also in walls, produce reticular and elastic fibers
**Outer surface of alveoli has capillary network from the branching of the lobule's
arteriiole and venule. Like all capillaries, these just have epithelium and b mem
2. Respiratory Membrane: Alveolar walls and capillary walls that exchange gases via
diffusion. Very thin to allow rapid diffusion of gas. Extends from alveolar air space to bl
plasma and has four layers:
1. Alveolar wall: Layer of Type I and Type II alveolar cells & alveolar macrophages
2. Epithelial B Mem: underlying alveolar wall
3. Capillary B Mem: Often fused to epithelial basement membrane
4. Capillary Edothelium
9. BLOOD SUPPLY TO THE LUNGS
1. Receive blood via pulmonary arteries and bronchial arteris. Deoxygenated bl passes
through pulmonary trunk → L/R pulmonary art → L/R lung. Bronchial arteries deliver
O2 to the lungs and this mainly perfuses the muscular walls of the bronchi and
bronchioles.
2. Return blood to heart via four pulmonary veins that drain into L atrium. Most blood
returns to heart via pulmonary veins. Some blood drains into bronchial veins, branches
of azygos system, and returns to heart via superior vena cava
3. Pulmonary blood vessels: constrict in response to localized hypoxia (low O2). Other
body tissues dilate bl vess in response to this.
--Ventilation-perfusion coupling: Vasoconstriction in lungs diverts pulmonary blood
from poorly ventilated areas of lungs to well ventilated areas for more efficient gas
exchange. Perfusion (bl flow) to each area of the lungs matches the extend of ventilation
(airflow) to alveoli in that area.
7. Patency: Maintained by bony and cartilageouns frameworks of nose, sk muscles of pharynx,
cartilages of larynx, C-rings of trachea/bronchi, sm muscle in bronchioles, surfactant in alveoli.
--Compromised by: crushing bone/cartillage, deviated septum, nasal polyps, inflammation of
m mem, spasms of sm muscle, deficiency of surfactant.
8. PULMONARY VENTILATION (Breathing):
Flow of air into and out of the lungs. Air flows btn atmosphere and alveoli of lungs bc of
alternating pressure differences created by contraction and relaxation of respiratory muscles.
--Rate of airflow influenced by alveolar surface tension, compliance of lungs, airway resistance
Pressure Changes during Pulmonary Ventilation
1. INHALATION/Inspiration: Just before inhalation, air pressure inside lungs equals air
pressure of atmosphere (760mmHg/1atm). For air to flow in, pressure inside alveoli must
become lower than atmospheric pressure, achieved by increasing the size of the lungs.
--Boyle's Law: Gas in a closed container is inversely proportional to the vol of the
container. AKA: Increasing size (of the lungs) decreases pressure inside of it.
*The same number of molecules in half the vol produce 2x the pressure
--First step in expanding the lungs involves contraction of diaphragm w/resistance from
external intercostals.
1. Diaphragm: Most important muscle of inhalation. Innervated by phrenic nerves.
Contraction causes it to flatten which increases vertical diameter of the thoracic cavity.
Responsible for around 75% of air that enters the lungs during quiet breathing.
2. External Intercostals: Contraction elevates the ribs and causes increase in
anteroposterior and lateral diameters of the chest cavity. Responsible for 25% air flow.
3. Intrapleural Pressure: pressure w/n pleural cavity (btn parietal and visceral pleura).
Always negative pressure (lower than atmosphere) during quiet normal breathing, so
functions as a vacuum that suctions and attaches visceral pleura to the chest wall.
--This means if chest expands, lungs expand. When diaphragm/intercostals expand
thoracic cavity, volume of pleural cavity increases and intrapleural press decreases.
4. Alveolar Pressure (intrapulmonic): Pressure w/n alveoli of the lungs. Drops as
volume of lungs increases so lowered pressure causes air to flow into lungs.
--Most of the increase in volume of the lungs is due to lengthening and expansion of the
alveolar ducts and increase in size of openings into alveoli.
--Accessory muscles: participate in increasing size of thoracic cavity during forceful
inhalations, but make little (if any) contribution to normal quiet breathing.
Include: Sternocleidomastoid, scalene, pectoralis minor,
**Both normal quiet inhalation and exercise/forced inhalation involve muscular contraction
and are said to be active.
2. EXHALATION/Expiration: Breathing out due to pressure gradient in opposite direction.
--Passive process because normal quiet exhalation does not involve muscular contraction
1. Elastic Recoil: Natural tendency of the chest wall and lungs to spring back after being
stretched. Influenced by
(1) Recoil of elastic fibers stretched during inhalation
(2) Inward pull of surface tension due to film of intrapleural fluid btn visc/par pleurae
--Starts when inspiratory muscles relax, diaphragm moves superiorly and intercostals
depress the ribs both decreasing vertical, lateral, anteroposterior diameters of the thoracic
cavity which decreases lung volume. Increases pressure, air flows out to lower pressure.
--Forceful exhalation is active and recruits muscles of exhalation: abdominal and internal
intercostals which contract and pulls ribs inferiorly, compresses viscera forcing diaphragm
superiorly.
**Intrapleural pressure is always less than alveolar, but may exceed it during coughs
3. OTHER FACTORS affecting pulmonary ventilation
1. Surface Tension of Alveolar Fluid: arises at all air-water interfaces due to polarity of
H20 making them more attracted to each other than to gas in air.
--When surrounding a sphere of air (as in alveolus or soap bubble,) tension produces
inward directed force. Surface tension causes alveoli to assume smallest possible
diameter and surface tension must be overcome to expand lungs in inhalation.
--Accounts for 2/3 elsatic recoil which decreases size of alveoli in exhalation
--Surfactant: Phospholipids and lipoproteins present in alveolar fluid reduces surface
tension below the surface tension of pure water. Higher surface tension may cause
alveoli to collapse at the end of each exhalation and great effot to reopen them.
2. Compliance of Lungs: How much effort is required to stretch lungs and chest wall.
1. High compliance: Lungs and chest wall expand easily due to elastic fibers that are
easily stretched and surfactant that reduces surface tension. May also be due to
destruction of elastic fibers in alveolar walls (emphysema)
2. Low compliance: Resist expansion. May be due to scar tissue, fluid in tissue,
deficiency in sufactant, or impeded lung expansion due to paralysis, etc.
--Related to elasticity and surface tension
3. Airway Resistance: Rate of airflow through airways depends on both pressure
difference and resistance.
--Airflow: pressure difference between alveoli and atmosphere divided by the resistance
--Walls of airways offer resistance to normal flow. Bronchioles enlarge during inhalation
bc their walls are pulled outward in all directions and larger diameters offer decreased
resistance. During exhalation, their resistance increases as their diameters decrease.
--Airway diameter is regulated by degree of contraction or relaxation of sm muscle in
walls of the airways. Signals from sympathetic division of the ANS causes relaxation
of bronchiolar sm muscle (bronchodilation) that decreases resistance. Signals from the
parasympathetic division cause contraction (bronchoconstriction) and increased res.
9. LUNG VOLUMES AND CAPACITIES
1. Lung Volumes: amount of air that can be measured directly by use of a spirometer
--Spirometer: Measures volumes and capacites, records a spirogram
1. Tidal Volume (Vt): Volume of one breath, varies from one person to another and at
different times in same person.
--About 70% of the tidal vol actually reaches respiratory zone of resp system
(bronchioles, alveolar ducts, alveolar sacs, alveoli) and participates in external
respiration. Other 30% stays in conducting airways of nose, pharynx, larynx, trachea,
bronchi, bronchioles, terminal bronchioles.
2. Anatomic (respiratory) Dead Space: all conducting airways with air that does not
undergo respiratory exchange. This means not all air inhaled can be used for exchange
3. Inspiratory Reserve Volume (IRV): Additional inhaled air over normal capacity (tidal
volume of 500mL) that can be taken in after forced exhalation.
4. Expiratory Reserve Volume (ERV):
5. Residual Volume (RV):Volume of air that remains in the lungs due to subatmospheric
intrapleural pressure that keeps alveoli slightly inflated and some air in noncollapsable
airways even after expiratory reserve is exhaled. Cannot be measured w/spirometry
6. Minimal Volume: Air remaining after thoracic cavity is opened and intrapleaural
pressure rises to equal atmospheric pressure and forces out some residual volume. Can
tell if baby was born dead or died after birth
2. Lung Capacities: combinations of different lung volumes
1. Inspiratory Capacity (IC): Sum of tidal vol and inspiratory reserve vol
2. Functional residual Capacity (FRC): sum of residual vol and expiratory reserve vol
3. Vital Capacity (VC): sum of inspiratory reserve vol, tidal vol, expiratory reserve vol
4. Total Lung Capacity (TLC): Sum of vital capacity and residual vol
5. Minute Ventilation (V): Total vol of air inspired and expired each minute calculated by
tidal vol multiplied by respiratory rate.
6. Alveolar Ventilation (Va): Vol of air per minute that actually reaches the respiratory
zone becausee not all of the minute ventilation can be used in gas exchange.
10. EXCHANGE OF O2 and CO2
1. DALTON'S LAW: Helps us understand how gases move down pressure gradients by
diffusion. States that each gas in a mixture of gases exerts its own pressure as if no other
gases were present.
Pressure of a specific gas in a mix is its partial pressure which is added to other gases'
partial pressures to find total pressure. Atmosphere: N2, O2, Ar, CO2, H2O, etc.
--Partial pressure determines the movement of O2 and CO2 btn atmosphere and lungs,
lungs and blood, and btn body cells and blood bc they move from area of higher p press
to lower pp.
--Alveolar air: less O2 and more CO2 because (1) gas exchange increases CO2 content
and decreases O2; (2) when air is inhaled it becomes humidified across mucosal linings
and water vapor content increases decreasing the relative percent of O2.
--Exhaled air: contains more O2 than alveolar air bc some exhaled air was in anatomic
dead space and did not participate in gas exchange.
2. HENRY'S LAW: Explains how the solubility of gas relates to its diffusion. States that the
quantity of gas that will dissolve in a liquid is proportional to pp of the gas and its solubility.
--Ability of gas to stay in solution is greater when pp is higher & high solubility in H2O
--Higher solubility, higher pp = more gas will stay in solution. More CO2 dissolved in bl
plasma bc 24x greater solubility than O2. N2 has little effect on our bodies because it
has a very low solubility so very little dissolves in bl plasma.
--Explains why increase of total air press causes pp of all its gases to increase. (Scuba
diver breathing compressed air can have bad effects of nitrogen which will dissolve
more in the bl plasma and interst fluid, ascending too rapidly causes the bends when
bubbles in nervous tissue are formed due to N2 coming out of solution too quickly.)
3. EXTERNAL RESPIRATION/Pulmonary gas exchange: diffusion of O2 from air in
alveoli of lungs to blood in pulmonary capillaries and the diffusion of CO2 in opp direction.
--Converts deoxygenated blood coming from R side of heart into oxygenated.
**Only occurs in the lungs**
1. O2 diffuses from alveolar air into bl in pulmonary capillaries bc pp is lower (esp if
exercising). Diffusion will continue until pp of O2 of pulmonary capillary blood
matches ppO2 of alveolar air.
--PPO2 of pulmonary veins is slightly less that p capillaries because it mixes w/bl that
has passed through conducting portions of respiratory system where exchange has not
occurred.
2. CO2 diffuses from deoxygenated bl into alveolar air. PPCO2 in deox bl is higher than
alveolar, so diffuses into alveoli until ppCO2 is equal. Exhalation keeps it equal and
oxygenated bl returning to the heart has the same amount.
3. Large number of capillaries means bl flows through them slowly and picks up
maximal amount of O2 and even when moving faster and transit time is shorterit
maintains a goo amount of ppO2.
4. INTERNAL RESPIRATION/Systemic gas exchange: Exchange of O2 and CO2 between
systemic capillaries and tissue cells. Occurs in tissues throughout the body.
1. PPO2 of systemic capillary bl is higher than in tissue cells bc these use O2 for ATP prod.
So O2 diffuses out of capillaries and into cells until equilibrium is reached.
2. CO2 diffuses from tissue cells to capillaries bc cells constantly produce CO2 .
3. At rest, only need 25% available O2 in oxygenated blood. Deoxygenated bl retains
about 75% of O2 content.
5. FACTORS AFFECTING RATE OF PULMONARY & SYSTEMIC EXCHANGE
1. PP difference of the gases: Alveoar ppO2 must be higher than in bl. (1) Rate of
diffusion is faster when difference is larger (exercise, etc). (2) Affected by rate of
airflow into and out of the lungs (slow ventilation decreases amount of gas exchange
possible btn air and blood.) (3) Increasing altitude decreases atmospheric pressure and
ppO2 so O2 diffuses more slowly (high altitude sickness due to lower O2 in bl)
2. Surface area available for gas exchange: Alveoli have huge surface area, capillaries
surround each alveolus. Decreasing surface area decreases rate of external respiration.
3. Diffusion Distance: Respiratory membrane is thin for quick diffusion, capillaries are
narrow to minimize diffusion distance from alveolar air space to hemoglobin in RBC.
Buildup of interstitial fluid btn alveoli (pulmonary edema) slows rate of gas exchange
by increasing diffusion difference.
4. Molecular weight and solubility of the gases: O2 has lower molecular weight than
CO2 so should diffuse faster BUT due to solubility of CO2 net outward movement of
CO2 is 20x greater than net inward movement of O2 diffusion. When diffusion is slower
than normal, hypoxia occurs bc significant retention of CO2 (hypercapnia)
11. TRANSPORT OF O2 and CO2
1. O2 Transport: Doesn't dissolve easily in water, so 98.5% is bound to hemoglobin in RBC
and 1.5% dissolved in bl plasma.
1. Oxyhemoglobin: Hemoglobin bound with oxygen. (Hb-O2)
2. Hemoglobin and O2 PP: Higher the ppO2, the more O2 combines w/Hb.
1. Fully saturated: When Hb is completely converted to Hb-O2.
2. Partially saturated: Hb consists of a mixture of Hb and Hb-O2.
3. Percent Saturation of Hb: expresses average saturation of Hb w/O2.
--Relationship btn % satruation and ppO2 is illustrated w/O2-Hb dissociation
curve. When ppO2 is high (pulmonary capillaries), Hb binds w/large amounts of O2
and is almost 100% saturated. When ppO2 is low (tissue capillaries), Hb is partially
saturated, dissolved O2 is unloaded via diffusion into tissue cells.
--Blood picks up a nearly full load of O2 from the lungs even when ppO2 of alveolar
air is low. When pressure drops too low, large amounts of O2 are released from Hb
in response to only small decreases in ppO2 (exercise).
3. Other factors affecting affinity of Hb and O2
Affinity: tightness with which Hb binds to O2. PPO2 is most important factor to
determine %O2 saturation, but these factors shift entire curve to higher affinity or lower.
1. Acidity: Increase acidity (lower pH) decreases affinity of Hb for O2, O2 dissociates
more readily from Hb.
--Metabolically active tissues produce lactic acid and carbonic acid
--Bohr effect: Decrease in pH (increase in H+) that causes O2-Hb dissociation curve
to shift to the right meaning at any give ppO2, Hb is less saturated w/O2. Hb can act
as a buffer for H+ but when H+ binds to aa in Hb they alter its structure slightly and
decrease O2 carrying capacity. O2 is driven off Hb and becomes more available.
*Increase in H+ causes O2 to unload from Hb, binding O2 to Hb releases H+
**Reverse is also true.
2. PPCO2: CO2 can bind to Hb and shift curve to the right. PPCO2 increase, Hb
releases O2 more readily.
--Related to acidity in that low bl pH results from high ppCO2. When CO2 enters bl,
much of it is temporarily converted into carbonic acid (H2CO3) catalyzed by
carbonic anhydrase (CA) [CO2+H2O ↔ H2CO3 ↔ H+ + HCO3-]
--Carbonic acid thus formed in RBC dissociates into H+ and bicarbonate.
3. Temperature: As temp increases, O2 released from Hb releases to an extent. Heat is
byproduct of metabolism, so metabolically active cells that require more O2 liberate
more acids and heat that in turn promote O2 release from Hb-O2. Fever, too.
4. BPG (2,3-bisphosphoglycerate/diphosphoglycerate): Substance found in RBC
that decrease affinity of Hb for O2 and help unload O2 from Hb. Formed in RBC
when they break down glucose to produce ATP through glycolysis.
--Combines w/Hb by binding to terminal aa groups of two beta globin chains
causing it to bind w/O2 less tightly at heme group sites. More BPG, more O2 is
released. H like thyroxine, HGH, epinephrine, norepinephrine, testosterone increase
production of BPG. Higher at higher altitudes.
4. Fetal and Adult Hemoglobin Affinity
Fetal Hb affinity is higher bc binds to BPG less strongly so when ppO2 is low, Hb in
fetus can carry 30% more O2 than maternal Hb. O2 saturation of placenta is low, so
this is important to avoid hypoxia.
2. CO2 Transport
1. Dissolved CO2: smallest % is dissolved in bl plasma, diffuses into alveolar air in lungs
and is exhaled
2. Carbamino Compounds: A little more CO2 binds w/amino groups of aa and proteins
in blood and forms these compounds. Hb is most prevalent protein, so most of CO2 is
transported in this manner by Hb. CO2 binds to terminal aa in 2 alpha and beta globin
chains to form carbaminohemoglobin (Hb-CO2).
--Formation of Hb-CO2 is greatly influenced by ppCO2 which when high can promote
formation. In pulmonary capillaries ppCO2 is low and CO2 readily splits apart from
globin and enters alveoli via diffusion.
3. Bicarbonate Ions: 70% in HCO3- because as CO2 diffuses into systemic capillaries
and enters RBCs it reacts w/water in presence of enzyme carbonic anhydrase (CA) to
form carbonic acid that dissociates into H+ and HCO3-.
--Chloride shift: As CO2 and HCO3- accumulate in RBC, some HCO3- moves out into
bl plasma down concentration gradient causing exchange of negative ions that maintain
electrical balance btn bl plasma and RBC cytosol.
--Net effect is that CO2 is removed from tissue cells and transported in bl plasma as
HCO3- and all of these reactions reverse as bl passes through pulm capillaries and lungs
--Haldane effect: The lower the amount of Hb-O2, the higher the CO2 carrying
capacity of blood. Deoxyhemoglobin binds to and transports more CO2 than Hb-O2 and
it buffers more H+ than Hb-O2 thereby removing H+ from solution and promoting
conversion of CO2 to HCO3- w/CA.
12. CONTROL OF BREATHING
1. Respiratory Center: widely dispersed group of neurons that are divided based on location
and function and function to control breathing muscles.
1. Medullary Respiratory Center: Made up of 2 collections of neurons
1. Dorsal Respiratory Group (DRG/Inspiratory Area): In normal quite breathing,
generates nerve imp in bursts to diaphragm via phrenic nerves and external
intercostal muscles via intercostal nerves. Bursts begin weakly, increase for 2sec,
stop. Inactivity causes relaxation of muscles and recoil of lungs and thoracic wall.
2. Ventral Respiratory Group (VRG/Expiratory Area): Contains the pre-Bötzinger
complex that may be important in generation of rhythm of breathing, contains
pacemaker cells that set basic rhythm of breathing. These input to the DRG and
drive rate of AP generated by neurons there.
--The rest of the neurons in the VRG do not do normal breathing but are active
during forceful breathing. Activated by the DRG, neurons here send impulses to
accessory muscles of inhalation (sternocleidomastoid, scalenes, pectoralis minor).
--Forceful exhalation: DRG inactive, VRG neurons for forceful inhalation are
inactive, but other VRG neurons send imp to accessory muscles of exhalation
(internal intercostals, external/internal oblique, transversus abdominus, rectus
abdominus)
2. Pontine Respiratory Group (PRG/Pneumotaxic Area): collection of neurons in the
pons active during inhalation/exhalation, transmits imp to DRG in medulla, may play a
role in modifying the basic rhythm of breathing generated by the VRG.
13. REGULATION OF THE RESPIRATORY CENTER
1. Corticol Influences: Cerebral cortex connections enable voluntary breathing which is a
protective element but is limited by buildup of CO2 and H+
--DRG neurons in medulla are activated by buildup of ppCO2 and H+, send strong impulses
sent along phrenic and intercostal nerves to inspiratory muscles and breathing resumes
involuntarily.
--Hypothalamus and limbic centers also stimulate resp center allowing emotional stimuli to
alter breathing as in laughing.
2. Chemoreceptor Regulation: Modulates how quickly and deeply we breathe
1. Central chemoreceptors: near medulla oblongata in the CNS, responds to changes in
H+ concentration, ppCO2, or both.
2. Peripheral chemoreceptors: in aortic bodies in wall of aorta and carotid bodies in wall
of L and R common carotid arteries where they divide to internal & external carotid
bodies and both are part of the PNS. Sensitive to changes in ppO2, H+, ppCO2 in blood.
--Aortic body sensory neuron axons are part of vagus X nerves
--Carotid body sensory neuron axons are part of R and L glossopharyngeal IX nerves
--CO2 is lipid-soluble and diffuses, but w/CA, forms H2CO3 and then H+ and HCO3-,
so increase in CO2 causes increase of H+ and vv.
--Hypercapnia/Hypercarbia: increase in ppCO2 (even slightly) stimulates central
chemoreceptors which respond to increasing H+ and CO2.
Peripheral chemoreceptors are also stimulated and respond to not only increasing H+
and CO2 but also to O2 deficiency when ppO2 in arterial blood falls from normal level
of 100mmHg but is above 50mmHg.
--Severe O2 deficiency depresses activity of central chemoreceptors and DRG which do
not respond well to ANY inputs and send fewer impulses to muscles of inhalation. When
breathing decreases or ceases, ppO2 falling establishes positive feedback loop (fatal)
--Negative feedback loop: regulates levels of CO2, O2, H+
1. Increase in ppCO2, decreased pH (increase H+), decreased ppO2 makes input from
central/peripheral chemoreceptors cause DRG to be highly active/increase breathing.
Hyperventilation: Rapid deep breathing allows inhalation of more O2, exhalation
of CO2 until ppCO2 and H+ levels are normal.
2. Hypocapnia/hypocarbia: Arterial ppCO2 is lower than 40mmHg, central and
peripheral chemoreceptors aren't stimulated, no impulses to DRG. DRG neurons set
their own pace until CO2 accumulates and ppCO2 rises to 40mmHg. DRG more
strongly stimulated when ppCO2 is rising above normal than when ppO2 is falling
below normal, so voluntary hyperventilation causes hypocapnia and ability to hold
breath longer.
CHAPTER 26: THE URINARY SYSTEM
1. Components of the Urinary System:
Kidneys [filter wastes, excrete into urine (nephrology study of the kidneys], ureters [carries
urine to bladder], urinary bladder [stores urine], urethra [excretes urine]
2. KIDNEYS: do major work of urinary system
1. Excrete wastes: form urine and exrete wastes from metabolic processes (nitrogenous
wastes) urea, ammonia from deamination of aa; creatinine from creatine phosphate, uric
acid from catabolism of nucleic acids, urobilin from Hb. Others are foreign like drugs.
2. Regulation of blood ionic composition: Na+, K+, Cl-, Ca2+, HPO4*2- [phosphate] adjusts
by altering levels excreted in urine
3. Regulation of blood pH by excretion of H+ into urine and conserving HCO3- [bicarbonate]
4. Regulation of bl vol by conserving or eliminating H2O in urine. Increase bl vol, up bl press
5. Regulation of bl press via enzyme renin that activates renin-angiotensin-aldosterone
pathway and increases bl press
6. Maintains bl osmolarity by separately regulating loss of H2O and loss of solutes in urine.
7. Production of H Calcitriol (active Vit D, regulates Ca2+ homeostasis) and erythropoietin
(stimulates production of RBC)
8. Regulation of bl glucose levels by using aa glutamine in gluconeogenesis and then
releasing glucose into bl to maintain bl glucose.
ANATOMY OF THE KIDNEYS: Just above the waist btn peritoneum and posterior wall of
abdomen. Retroperitoneal because position is posterior to peritoneum.
External:
1. Renal hilum indentation near center of concave border through which ureter emerges from
kidney along w/bl vess, lymph vess, nerves. Expands into cavity w/n kidney called the
renal sinus which contains part of renal pelvis, calyces, branches of renal bl vess/nerves.
Adipose tissue stabilizes position of these structures in the renal sinus.
2. Three tissue layers
1. Renal capsule: Deep, smooth, transparent sheet of dense irregular conn tiss continuous
w/outer coat of ureter. Barrier against trauma and mantains shape
2. Adipose capsule: Middle, mass of fatty tissue surrounding renal capsule protects kidney
from trauma and holds it firmly in place w/n abdominal cavity
3. Renal Fascia: Superficial, thin layer of dense irregular conn tiss anchors kidneys to
surrounding structures and abdominal wall. On anterior surface is deep to peritoneum
Internal: Two distinct regions
1. Renal Cortex: superficial, light red, smooth textured, extends from renal capsule to base of
renal pyramids into spaces btn them (Renal columns). Divided into cortical zone and
inner juxtamedullary zone.
2. Renal medulla: deep, dark red-brown, consists of several cone-shaped renal pyramids.
Base of pyramids face renal cortex, apex is renal papilla and points toward renal hilum
--Together, medulla and cortex are the parenchyma (functional portion) of kidney. Contain
all functional components:
Nephrons: microscopic, forms filtrate and drains it into papillary ducts that extend
through renal papillae of pyramids and drain into cuplike minor and major calyces.
1. Minor calyx: (18-20 of them) receives filtrate from pap ducts of one of the renal
papilla and delivers it to a major calyx.
2. Major calyx: (2-3 of these) urine drains into single large cavity called renal pelvis
and then out through ureter into urinary bladder.
**Once filtrate enters calyces, no further reabsorption can occur bc simple
epithelium of nephron and ducts becomes transitional epithelium in calyces so
filtrate becomes urine.
BLOOD AND NERVE SUPPLY OF THE KIDNEYS
Abundant bl vessels, receive 20-25% of resting cardiac output via R and L renal arteries.
1. Renal artery divides into several segmental arteries that supply different segments of kidn
2. Segmental artery branches enter parenchyma and pass through renal columns between the
renal lobes as interlobular arteries
Renal lobes: renal pyramid, some renal column on sides, renal cortex (base of pyramid)
3. Interlobular arteries arch btn renal medulla and cortex as arcuate arteries (bow-like)
4. Arcuate arteries divide and produce serioes of cortical radiate (interlobular) arteries
5. CR arteries radiate outward and enter renal cortex where they branch into afferent
arterioles.
6. Afferent arterioles supply one nephron each and then divides into tangled ball-shaped
capillary network called a glomerulus.
7. Glomerulus capillaries reunite into efferent arterioles that carry bl out.
**Glomerulus capillaries are unique in that they are positioned btn 2 arterioles rather than
between an arteriole and a venule. They play an important role in urine formation and are
considered part of both cardiovascular and urinary system.
8. Efferent arterioles divide into peritubular capillaries which surround tubular parts of the
nephron and renal cortex. Some efferent arterioles extend long loop-shaped capillaries
called vasa recta that supply tubular portions of nephron in renal medulla.
9. Peritubular capillaries reunite to form cortical radiate (interlobular) veins which also
receive blood from vasa recta.
10. CR veins drain blood through arcuate veins to interlobar veins between pyramids and
leaves through single renal vein that exits at renal hilum and carries bl to inferior vena cava
Abdominal aorta → L/R renal artery → Segmental arteries → interlobular arteries →
arcuate arteries → cortical radiate/interlobular arteries → afferent arterioles → glomerulus
→ efferent arterioles → peritubular capillaries/vasa recta → cortical radiate/interlobular
veins → arcuate veins → interlobular veins → renal vein → [renal hilum] → IVC
--Renal nerves originate in renal ganglion and pass throgh renal plexus into kidneys along
w/renal arteries. Renal nerves are part of the symp division of ANS and are mostly vasomotor
nerves that regulate bl flow through kidneys by vasoconstriction/dilation of arterioles.
3. THE NEPHRON: Functional units of the kidneys
1. Renal corpuscle: bl plasma is filtered
1. Glomerulus (capillary network)
2. Glomerular capsule/Bowman's capsule: double walled epithelial cup surrounding
glom capillaries. Bl plasma is filtered here then passes into tubule
2. Renal tubule: filtered fluid (glomerular filtrate) passes into here
1. Proximal convoluted tubule (PCT): attached to glomerular capsule
2. Nephron loop/Loop of Henle: coiled, along w/r corpuscle lies in renal cortex and
extends into renal medulla, makes hairpin turn, returns to renal cortex
--Nephron loop connects prox and distal convoluted tubules. Begins at point where prox
conv tubule takes final turn downward beginning in renal cortex.
--Descending limb of nephron loop: extension downward into renal medulla
--Ascending limb of nephron loop: After hairpin turn, returns to renal cortex and
terminates at distal convoluted tubule
3. Distal convoluted tubule (DCT): farther from glomerule capsule, these from several
nephrons empty into single collecting duct (CD).
3. Collecting ducts unite and converge into sevearl hundred large papillary ducts that drain
into minor calyces. Collecting and papillary ducts extend from renal cortex through renal
medulla to renal pelvis. Many nephrons, much fewer collecting ducts, even fewer pap ducts
--Cortical Nephrons: 80-85% of nephrons. Renal corpuscles lie in outer portion of renal cortex
and penetrate only into outer region of renal medulla. Short nephron loops receive bl supply
from peritubular capillaries from efferent arterioles
--Juxtamedullary nephrons: renal corpuscles lie deep to cortex, close to medulla, have a
LONG nephron loop from deepest region of medulla which receives bl supply from peritubular
capillaries & vasa recta from efferent arterioles. Ascending limb of nephron loop has two parts:
1. Thin ascending limb: lumen same as other areas of ren tubule but epithelium is thinner
2. Thick ascending limb: follows the thin limb.
**Long nephron loops enable excretion of very dilute or very concentrated urine
HISTOLOGY OF THE NEPHRON
Single layer of epithelial cells forms wall of glomerular capsule, renal tubule, ducts, but each
have distinctive histology reflecting function.
1. GLOMERULAR (BOWMAN'S) CAPSULE
1. Visceral layer: made up of podocytes: modified simple squam epithelial cells with
footlike projections (pedicels) that wrap around the single layer of endothelial cells of
glomerular capillaries and form inner wall of capsule.
2. Parietal layer: simple squam epithelium, forms outer wall.
3. Capsular space: between two layers of capsule, continuous w/lumen of renal tubule,
receives fluid filtered from glom capillaries
2. RENAL TUBULE AND COLLECTING DUCT
1. Proximal Convoluted Tubule: simple cuboidal epithelial cells w/prominent brush
border of microvilli on apical surface facing lumen. Microvilli increase surface area for
reabsorption and secretion.
2. Descending limb of nephron loop (and first part of ascending limb of nephron loop in
the thin limb) are composed of simp squam epith.
**Cortical/short loop nephrons lack thin limb!**
3. Thick limb of ascending limb of nephron: simple cuboidal to low columnar epith
4. Final part of ascending limb of every nephron makes contact w/afferent arteriole
servind that renal corpuscle and columnar tubule cells are crowded together (called
macula densa).
5. Wall of afferent arteriole (and sometimes efferent arteriole) has juxtaglomerular cells
(JG) which are modified sm muscle cells. Together w/macula densa form
juxtaglomerular apparatus (JGA) which helps regulate bl press w/n kidneys.
6. DCT: begins just past macula densa and the last part of it and all of the collecting ducts
have two different cells
1. Principal cells: receptors for ADH and aldosterone which regulate their function
2. Intercalated cells: fewer of these, play a role in homeostasis of bl pH.
7. Papillary ducts then have simple columnar epithelium
**Number of nephrons constant from birth, increase in size is only due to growth of individual
nephron. New one do not form if injured or destroyed. Disfunction may not be evident until
25% less than normal bc remaining functional nephrons adapt to handle larger load. This is why
removing a kidney stimulates hypertrophy of remaining kidney which can fill 80% of rate of
both kidneys.
THREE BASIC FUNCTIONS OF THE NEPHRON
1. Glomerular filtration: first step of urine production: water and solutes in bl plasma move
across wall of glomerular capillaries where they're filtered and move into glom capsule and
then into renal tubule
2. Tubular reabsorption: Filtered fluid flows through tubules and collecting ducts. Tubule
cells reabsorb 99% of filtered water and useful solutes which return to bl as it flows through
peritubular capillaries and vasa recta.
(Reabsorption: return of substances to bl; Absorption: entry of new substances to body)
3. Tubular secretion: Filtered fluid flows through renal tubules and coll ducts and renal
tubules and duct cells secrete other materials (wastes, drugs, excess ions) into fluid. This
removes substances from blood.
**Solutes/fluid that drains into minor/major calyces and renal pelvis constitute urine and are
excreted at rate equivalent to rate of glomerular filtration plus rate of secretion minus
reabsorption**
--Maintains homeostasis of bl vol and composition.
4. GLOMERULAR FILTRATION:
Glomerular filtrate: fluid enters capsular space. <99% is returned to bl in tubular reabsorption
Filtration fraction: fraction of bl plasma in afferent arterioles of kidneys that becomes
glomerular filtrate.
FILTRATION (Endothelial-capsular) MEMBRANE: Glomerular capillaries and podocytes
that completely encircle the capillaries form this sandwhichlike leaky barrier that permits
filtration of water and small solutes but prevents filtration of blost plasma proteins and bl cells
1. Glomerular endothelial cells leaky due to large fenestrations that permit solutes in bl
plasma to exit glom capillaries but prevents filtration of bl cells.
--Mesangial cells: Located among glom cap and in cleft btn afferent and efferent arterioles,
are contractile cells that help regulate glomerular filtration by controling surface area.
2. Basement Membrane: layer of acellular material btn endothelium and podocytes that
consists of minute collagen fibers and negatively charged glycoproteins. Pores in basement
mem allow water and small solutes to pass but negative charges of glycoprot repel plasma
proteins which are typically anionic so their filtration is hindered.
3. Filtration Slit formed by podocyte pedicels which wrap around glom cap. Have a thin slit
membrane which extends across each filtration slit and permits passage of molecules like
water, glucose, vit, aa, very small plasma prot, ammonia, urea, ions. Less than 1% of
albumin (most plentiful plasma prot) passes because is slightly too big to get through.
**Filtration principle is the same here as in bl cap, but vol of fluid filtered by renal
corpuscles is much larger due to:
1. Glom cap present large surface area for filtraion bc are long and extensive. Mesangial
cells regulate surface area availability (relax, max surface area, filtration is high)
2. Filtration mem is thin and porous, 50x leakier than bl capillaries in most other tissues
because of large fenestrations
3. Glom cap bl press is high. Efferent arteriole is smaller in diameter than afferent so
resistance to outflow of bl from glomerulus is high making bl press in glom cap higher
than in bl cap in other parts of the body.
5. NET FILTRATION PRESSURE (NFP)
Glomerular filtration depends on three pressures
1. Glomerular bl hydrostatic pressure (GBHP): bl press in glomerular capillaries. Promotes
filtration by forcing wateer and solutes in bl plasma through filtration mem
2. Capsular hydrostatic pressure (CHP): hydrostatic press against filtration mem fluid
already in caapsular space and renal tube. Opposes filtration
3. Bl colloid osmotic pressure (BCOP): from presence of proteins (albumins, globulins,
fibrinogen) in bl palsma. Opposes filtration, stronger than CHP.
**NFP = GBHP-CHP-BCOP, in favor of filtration into capsular spaces
6. GLOMERULAR FILTRATION RATE (GFR): Amount of filtrate formed in all renal
corpuscles of both kidneys each minute. If too high, substances may pass too quickly through
renal tubules, not reabsorbed, lost in urine. Too low wastes may not be adequately excreted.
--Directly related to pressures that determine NFP: blood loss lowers mean arterial bl press,
decreases GBHP, filtration ceases if GBHP drops to 45mmHg which equals opposing press
--When systematic bl press rises above normal, NFP and GFR increase very little. GFR is
nearly constant when mean arterial bl press is btn 80 and 180mmHg.
Adjust blood flow into and out of the glomerulus. GFR increases when bl flow into glom
cap increases and bl flow is controlled by arterioles.
Alter glomerular capillary surface area available for filtration.
1. RENAL AUTOREGULATION OF GFR
Kidneys maintain constant renal bl flow and GFR via renal autoregulation.
1. Myogenic Mechanism: when stretching triggers contraction of sm muscle cells in walls
of afferent arterioles. Bl press rises, GFR rises bc renal bl flow increases, stretches walls
of arterioles. In response to stretch, sm muscle fibers in afferent arteriole contract and
renal bl flow decreases, GFR decreases. Normalizes bl flow in seconds after change.
2. Tubuloglomular feedback: part of renal tubes (macula densa) and provides feedback to
glomerulus when GFR is above normal due to high bl press, filtered fluid flows more
rapidly in tubules and proximal convoluted tubule and nephron loop have less time to
reabsorb Na+, Cl-, H2O.
--Macula densa cells detect increased delivery of Na+, Cl-, H2O and inhibit release of
NO from JGA. Afferent arterioles constrict when NO declines and less bl flows into
glomerular cap, GFR decreases. Opposite occurs to a lesser degree, happens more
slowly than Myogenic Mechanism.
2. NEURAL REGULATION OF GFR: Sympathetic ANS fibers release norepinephrine that
causes vasoconstriction through acivation of a1 receptors that are plentiful in sm muscle of
afferent arterioles.
--At rest, symp stim is moderately low, arterioles are dilated, renal autoregulation prevails
--With stimulation, arterioles constrict to the same degree, bl flow in and out is restricted to
the same extent and GFR is decreased slightly.
--Greater stimulation causes vasoconstriction of afferent arterioles to predominate and bl
flow in is greatly decreased, lowering GFR significantly. This causes reduced urine output
to conserve bl vol and permits greater bl flow to other body tissues.
3. HORMONAL REGULATION OF GFR:
1. Angiotensin II: potent vasoconstrictor that narrows arterioles and reduces renal bl flow,
decreasing GFR
2. Atrial Natriuretic Peptide (ANP): from atria of heart causes relaxation of glomerular
mesangial cells and increases capillary surface area available for filtration. Glom
filtration rater rises as surface area increases.
7. TUBULAR REABSORPTION and TUBULAR SECRETION
1. Vol of fluid entering prox convoluted tubules is greater than total bl plasma because
total rate of glomerular filtration is so high. For this reason, reabsorption (return of filtered
water and many filtered solutes to bl) returns 99% of water
2. Epithelial cells along renal tubule and duct carry out reabsorption but proximal
convoluted tubules make the largest contribution. Reabsorb: water, glucose, urea, aa, Na+,
K+, Ca2+, Cl-, HCO3-, HPO4^2-
3. After prox conv tubule, distal cells fine-tune the reabsorption process for homeostasis
4. Tubular secretion transfers material from bl/tubule cells into glomerular filtrate. Secrete:
H+, K+, NH4- (ammonium), creatine, drugs like penicillin.
--Secrete H+, control bl pH, secretion of others help eliminate the from the body (urine)
REABSORPTION ROUTES: Fluid can move between adjacent tubule cells or through
individual tubule cells.
Tight junctions: surround and join neighboring cells along renal tubule.
--Apical mem contacts tubular fluid, basolatersl mem contacts interstitial fluid at base and
sides of the cells.
--Solute reabsorption drives water reabsorption because water reabsorption occurs via
osmosis. 90% reabsorbed water occurs w/Na+, Cl-, glucose.
--Obligatory water reabsorption: Water reabsorbed w/solutes in tubular fluid. “Obliged”
to follow solutes. Occurs in proximal conv tubule and descending limb of neph loop bc
segments of nephron are permeable to water.
--Facultative Water Reaborption: capable of adapting, regulated by ADH, occurs in
collecting ducts.
REABSORPTION AND SECRETION: PROXIMAL CONVOLUTED TUBULE (PCT)
**Reabsorption: return of substances to bl; Secretion: Removal from blood**
Reabsorbs the larges amt of water and solutes (Na+, K+, glucose, aa, organic solutes, Cl-,
urea, HCO3-, some Ca2+, Mg2+, HPO4^2-)
--Secretes H+, ammonium (NH4+), urea.
1. Reabsorption of solutes creates osmotic gradient that promotes reabsorption of water)
2. Cells lining PCT and Descending Limb of the Nephron Loop (DLNL) are especially
permeable due to aquaporin-1 molecules that are in p mem and increase rate of water
movement across apical/basolateral mem.
3. Ammonia (NH3) is waste from deamination in hepatocytes which convert it to urea
that is less toxic. Excreted in sweat and urine, In bl they are filtered at glomerulus and
secreted by PCT into tubular fluid.
SUBSTANCES REABSORBED: Na+, K+, glucose, aa, water Cl-, urea, HCO3-, Ca2+,
Mg2+, HPO4^2- (No longer in glomerular filtrate)
SUBSTANCES SECRETED: NH4, H+, urea
REABSORPTION IN THE NEPHRON LOOP
Tubular fluid is now w/o glucose, aa, nutrients, osmolarity is close to osmolarity of the bl bc it
keeps pace w/reabsorption of solutes along PCT.
--REABSORBS: filtered water, Na+, K+, Cl-, HCO3-, some Ca2+, Mg2+.
**First place that water reabsorption is not coupled w/solutes bc part of nephron loop is
impermeable to water. Independent regulation of volume and osmolarity of body fluids.
--Water: reabsorbed in descending limb of n loop, little to no is reabsorbed in ascending limb.
Ions but not water are reabsorbed in this part so osmolarity of tubular fluid decreases as it flwos
to distal end of ascending limb.
REABSORPTION IN EARLY DISTAL CONVOLUTED TUBULE
Reabsorbs: water, Na+, Cl-.
**Major site of parathyroid H stimulation for reabsorption of Ca2+ depending on needs.
REABSORPTION AND SECRETION IN LATE DCT and COLLECTING DUCT
Late DCT: 90-95% solutes and water have been returned to bloodstream. Principal cells
reabsorb Na+, secrete K+, stim by aldosterone and antidiuretic H. Intercalated cells
reabsorb HCO3-, K+, secrete H+. Water depends on body's needs.r3
--principal cells secrete variable amount of K+ in urine.
8. HOMEOSTATIC REGULATION OF TUBULAR REABSORPTION AND SECRETION
1. Renin-Angiotensin-Aldosterone System
Stimulated by lowered bl vol and bl press. Symp stim also causes release of renin
1. Juxtaglomerular cells secrete renin into blood.
2. Renin clips angitensin I peptide off of angiotensinogen that is synth by hepatocytes.
3. Angiotensin-converting enzyme (ACE) In lung capillaries and elsewhere clips off 2+
aa and converts angiotensin I into angiotensin II which is the active form. Angiotensin
II does the following:
1. Decreases glomerular filtration rate by vasoconstriction of afferent arterioles
2. Enhances reabsorption of Na+ and H2O in prox con tubule by stimulating activity
of Na+-H+ antiporters
3. Stimulates adrenal cortex to release aldosterone which stimulates principal cells
in collecting ducts to reabsorb more Na+ (and therefore water) and secrete more K+.
This increases bl volume and pressure.
Angiotensin II: Site of action: Stimulates Na+-H+ antiporters in proximal tubule cells
Effects: increase reabsorption of Na+, wtr, increase bl press/vol
Aldosterone: Stim by angiotensin II, increased plasma K+. Released from adrenal cortex
Site of action: Enhances Na+-K+ ATPases in basolateral mem, Na+ channels in
apical mem of principal cells in collecting duct
Effects: Increases secretion of K+, reabsorption of Na+, water. Increases bl vol
and bl press
2. Antidiuretic H (ADH/Vasopressin):
Released by post pituitary stimulated by high bl omolarity of extracellular fluid, decreased
bl vol (Also pain, stress, nicotine, drugs, anesthetics, etc.) Targets kidneys and smooth
muscle in blood vessel walls.
--Regulates: facultative water reabsorption by increasing water permeability by principal
cells in last part of DCT and throughout collecting duct. W/o ADH are low permeability
--Stimulates: insertion of aquaporin-2-containing vesicles into apical mem via exocytosis.
This causes water perm of principal cell's apical mem to increase. Basolateral cells are
always relatively permeable, so water moves rapidly into bl, increase bl vol, press.
--Aquaporin-2 channels are removed when ADH levels decline
--Regulated by: Negative feedback due to osmolarity or osmotic pressure.
1. Osmolarity/Osmotic press of plasma or interstitial fluid increases (water
concentration decreases) hypothalamus detects the change → stimulate secretion of
ADH → principal cells become more permable.
Osmolarity/Osmotic press falls as facultative water reabsorption increases
2. Decreased bl vol causes stimulation of ADH secretion.
1. Normal hydration: enough ADH is present in bl to cause reabsorption of 99% of
filtered water. Remaining 1% is in urine (slightly hyperosmotic compared to bl)
2. Dehydration: Concentration of ADH is increased which increases the amount of water
reabsorbed in late distal and collecting duct making less than 1% of water unreabsorbed.
Urine is very hyperosmotic bc less water. Max limit is 19.8% in distal tube, c duct and
kidneys only produce a small amount of urine.
3. Overhydration: Concentration of ADH decreases causing decrease in water
reabsorption. More than 1% is unreabsorbed and urine output increases and is
hypoosmotic (dilute). If severe, no ADH in bl, 20% water is excreted in urin, kidneys
produce a large volume of urine.
3. ATRIAL NATRIURETIC PEPTIDE
Stimulated by: large increase in bl vol that stretches atria of the heart
Released from: atria of the heart
Function: in tubular regulation is unclear but can inhibit reabsorption of Na+ and water in
prox con tubule and c duct. Suppresses secretion of aldosterone and ADH. Result is
increased excretion of Na+ in urine (natriuresis) and increase urine output (diuresis) that
decreases bl vol and bl press.
4. PARATHYROID HORMONE (PTH)
Stimulated by: lower than normal Ca2+ in bloodstream.
Released from: parathyroid glands
Function: stimulates cells in early DCT to reabsorb more Ca2+ into bl by opening more
Ca2+ channels in apical mem. Inhibits HPO4- reabsorption in prox con tubules and
promotes its excretion. Result is increased Ca2+ reabsorption.
You might also like
- Francis Ian Salaver, RMT, MD: Study of Tissues, Their Functions and Their ArrangementDocument6 pagesFrancis Ian Salaver, RMT, MD: Study of Tissues, Their Functions and Their ArrangementMay Ann EnoserioNo ratings yet
- 08 - Lymphatic SystemDocument19 pages08 - Lymphatic SystemDanielSenpai69No ratings yet
- 08 - Lymphatic SystemDocument19 pages08 - Lymphatic SystemKonstantinos KosmidisNo ratings yet
- Histology 10 ImmunosystemDocument79 pagesHistology 10 ImmunosystemAbdul RahmanNo ratings yet
- H.Histology Lec1Document10 pagesH.Histology Lec1Marci MunirNo ratings yet
- Histo DR ZahraDocument56 pagesHisto DR Zahraali.mohammed.official.7No ratings yet
- Histology of Lymphoid Organ PDFDocument82 pagesHistology of Lymphoid Organ PDFRionaldy TaminNo ratings yet
- The Lymphatic System and Immunity by Navarro and Orjalo BS Psy 3 1Document27 pagesThe Lymphatic System and Immunity by Navarro and Orjalo BS Psy 3 1markNo ratings yet
- Immune System and Lymphoid OrgansDocument15 pagesImmune System and Lymphoid Organscatalia fuaresNo ratings yet
- 2.3 Lymphatics PPT (Dr. Mattheus)Document39 pages2.3 Lymphatics PPT (Dr. Mattheus)12345karlos ParrasNo ratings yet
- Chapter 2 Basicc Immunology Ppts DZ 2010Document85 pagesChapter 2 Basicc Immunology Ppts DZ 2010TofikNo ratings yet
- Lymphatic SystemDocument20 pagesLymphatic SystemROSE ANN JAWADNo ratings yet
- Lymphoid Organs MedI 2020 HistDocument27 pagesLymphoid Organs MedI 2020 HistsamNo ratings yet
- هستولوجي هبه 2Document36 pagesهستولوجي هبه 2nagyrashad123No ratings yet
- Lymphatic SystemDocument24 pagesLymphatic SystemjabirNo ratings yet
- Thymus and Lymph NodeDocument37 pagesThymus and Lymph NodeJana Moataz Mohamed G02No ratings yet
- Histology, Lecture 12, The Lymphatic System (LEcture Notes)Document6 pagesHistology, Lecture 12, The Lymphatic System (LEcture Notes)Ali Al-QudsiNo ratings yet
- Organs of Immune SystemDocument31 pagesOrgans of Immune Systemspourush100% (2)
- Chapter 2 Basic ImmunologyDocument64 pagesChapter 2 Basic ImmunologykelifamohammadsaniabdulfatahNo ratings yet
- Immune Cells and OrgansDocument8 pagesImmune Cells and OrgansCharlz AriolaNo ratings yet
- White Blood Cells - Components of Lymphatic SystemDocument26 pagesWhite Blood Cells - Components of Lymphatic Systemislamicmedia188No ratings yet
- Lymphatic System 1-1Document37 pagesLymphatic System 1-1Nada Atef KoraitemNo ratings yet
- Thymus - Red Bone Marrow: Primary Lymphoid OrgansDocument7 pagesThymus - Red Bone Marrow: Primary Lymphoid OrgansGerard Dominic ArguellesNo ratings yet
- Lymphoid and Immune Systems: Department of Histology FK UNSRIDocument59 pagesLymphoid and Immune Systems: Department of Histology FK UNSRIMuhammad Ali Ridho ShahabNo ratings yet
- 08 - Lymphatic System TheoryDocument20 pages08 - Lymphatic System TheoryNoor 3laaNo ratings yet
- Lymphatic - StudentDocument9 pagesLymphatic - StudentLeslie CuevasNo ratings yet
- Organs of The Immune SystemDocument19 pagesOrgans of The Immune SystemprabuNo ratings yet
- Cells and Organs of Immune SystemDocument7 pagesCells and Organs of Immune Systemanumaria2024No ratings yet
- Functions:: Four Functions of SpleenDocument5 pagesFunctions:: Four Functions of SpleenRashid DayaoNo ratings yet
- Immuno Notes LectureDocument30 pagesImmuno Notes LectureSteph TabasaNo ratings yet
- Structure of ThymusDocument6 pagesStructure of ThymusShubham Pareshkumar KadiwalaNo ratings yet
- Lymphatic System PPT Notes SBDocument13 pagesLymphatic System PPT Notes SBnoshNo ratings yet
- Lymphatic SystemDocument22 pagesLymphatic SystemdrynwhylNo ratings yet
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocument1 pageHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieNo ratings yet
- Lecture 4 Lymphoid Organs and TissuesDocument24 pagesLecture 4 Lymphoid Organs and Tissuesanuja maliNo ratings yet
- Anatomy& EmbryologyDocument13 pagesAnatomy& EmbryologySravani PeddagangannagariNo ratings yet
- Histology - Immune and Hemopoietic OrgansDocument23 pagesHistology - Immune and Hemopoietic OrgansKacper DaraszkiewiczNo ratings yet
- Primary or Central 33Document23 pagesPrimary or Central 33Mahesh DevarintiNo ratings yet
- Self Test 2Document5 pagesSelf Test 2202310446No ratings yet
- Spleen and Palatine TonsilsDocument19 pagesSpleen and Palatine TonsilsJana Moataz Mohamed G02No ratings yet
- 5 Lymphatic SystemDocument74 pages5 Lymphatic SystemlakshmisareescollectionsNo ratings yet
- Exercise 15 Lymphoid OrganDocument7 pagesExercise 15 Lymphoid OrganJovelou MihangosNo ratings yet
- Lymphatic SystemDocument13 pagesLymphatic SystemBasant karn100% (6)
- Basic Immunology PDFDocument6 pagesBasic Immunology PDFAnastasia ENo ratings yet
- Chapter 22 Summary Chapter 22 SummaryDocument13 pagesChapter 22 Summary Chapter 22 SummarytinecastilloNo ratings yet
- Lecture 3 - Cells and Organs IIDocument30 pagesLecture 3 - Cells and Organs IIAhmed Examination100% (1)
- Lymphatic System Histology 2Document8 pagesLymphatic System Histology 2Ahmed JawdetNo ratings yet
- Lymphatic System TransesDocument6 pagesLymphatic System Transesadrielvamos28No ratings yet
- Review Histologi Sistem Imunologi Feb 2018 UHO - (1) .PPSXDocument47 pagesReview Histologi Sistem Imunologi Feb 2018 UHO - (1) .PPSXAmil MunduNo ratings yet
- Immune SystemDocument21 pagesImmune SystemAbdullah KhanNo ratings yet
- Lymphoid OrganDocument23 pagesLymphoid OrganSwetha RameshNo ratings yet
- Lymphatic System and Immunity: Student Learning OutcomesDocument8 pagesLymphatic System and Immunity: Student Learning Outcomeslily1liang-1No ratings yet
- ImmunoSero Side NotesDocument2 pagesImmunoSero Side NotesReca Marie FRIASNo ratings yet
- Lymphatic System: Prof. Shekhar TeliDocument19 pagesLymphatic System: Prof. Shekhar TeliShekhar TeliNo ratings yet
- Lymphatic Organs and TissuesDocument3 pagesLymphatic Organs and TissuesSaman Bharatha KotigalaNo ratings yet
- Anatomy and Function of Lymphoid Tissues: Wesam Mohammed EmharibDocument7 pagesAnatomy and Function of Lymphoid Tissues: Wesam Mohammed Emharibنسيم حامدNo ratings yet
- Immune System Docs 2019Document13 pagesImmune System Docs 2019David DavidNo ratings yet
- Immunology: Lymphoid Organs Sr. Sarupya Mercy College PalakkadDocument28 pagesImmunology: Lymphoid Organs Sr. Sarupya Mercy College PalakkadTahir AzizNo ratings yet
- Imm Lect 2Document22 pagesImm Lect 2samarsamar6000No ratings yet
- A Simple Guide to the Blood Cells, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Blood Cells, Related Diseases And Use in Disease DiagnosisNo ratings yet
- Growth of Stems: LEC 5: Tissues & The PrimaryDocument6 pagesGrowth of Stems: LEC 5: Tissues & The PrimaryShaira MuksanNo ratings yet
- Pages From SF601 V65 V 25 N 03 3Document15 pagesPages From SF601 V65 V 25 N 03 3Brian GalyanNo ratings yet
- Frog DissectionDocument4 pagesFrog Dissection2110038No ratings yet
- MeristemDocument25 pagesMeristemhazizi100% (3)
- Connective Tissue NotesDocument6 pagesConnective Tissue Notesferdinand padillaNo ratings yet
- Science 9 q1 Mod1 Respiratory and Circulatory System Ver FinalDocument33 pagesScience 9 q1 Mod1 Respiratory and Circulatory System Ver FinalNoah SmithNo ratings yet
- Muscular System 20222023Document29 pagesMuscular System 20222023Danny Mel ManglaylayNo ratings yet
- Neoplasia (Part 1)Document30 pagesNeoplasia (Part 1)يوسف الفيتوريNo ratings yet
- Anatomy PhysiologyDocument8 pagesAnatomy PhysiologyDOROLA CRIS JANELICA R.No ratings yet
- ID Studi Anatomi Daun Dari Tiga Anggota SukDocument8 pagesID Studi Anatomi Daun Dari Tiga Anggota SukAyu Wandira SenyawaNo ratings yet
- Digestive System AnatomyDocument32 pagesDigestive System AnatomyDerrick njugunaNo ratings yet
- 3 - SDocument45 pages3 - SFarnoush ShahriariNo ratings yet
- Has Felületi Topográfiája - AngolDocument43 pagesHas Felületi Topográfiája - Angolsozan.muhamadNo ratings yet
- Papanicolaou StainDocument2 pagesPapanicolaou StaindeblackaNo ratings yet
- Lesson-Science 5-Quarter 2Document24 pagesLesson-Science 5-Quarter 2SHANEDEE ANTONIONo ratings yet
- TissuesDocument6 pagesTissuesRahul SinghNo ratings yet
- Digestive System and Respiratory SystemDocument10 pagesDigestive System and Respiratory SystemKathMae BoaNo ratings yet
- Fistan (Morfologi Dan Anatomi Tanaman)Document49 pagesFistan (Morfologi Dan Anatomi Tanaman)Dwisepti NuramaliahNo ratings yet
- Adobe Scan Mar 27, 2023Document4 pagesAdobe Scan Mar 27, 2023Sahid HaqueNo ratings yet
- LLENAS - DLL Sci 9 - Sept 5 9 KMLDocument6 pagesLLENAS - DLL Sci 9 - Sept 5 9 KMLNicole Eve Pelaez-AbarrientosNo ratings yet
- Mobilizing The Myofascial SystemDocument296 pagesMobilizing The Myofascial System박주영100% (1)
- GENERAL BIOLOGY Cell Types Cell ModificationsDocument4 pagesGENERAL BIOLOGY Cell Types Cell ModificationswenkamuyNo ratings yet
- Exam 2 ReviewDocument17 pagesExam 2 ReviewKaitlyn RobisonNo ratings yet
- Daftar Pustaka UrutDocument3 pagesDaftar Pustaka UrutBian PutriNo ratings yet
- Plant RootsDocument8 pagesPlant RootsAndreaaAAaa TagleNo ratings yet
- Happ Chapter 5 TransesDocument7 pagesHapp Chapter 5 TransesFrencess Kaye SimonNo ratings yet
- 1 - Anatomical Terminology KEYDocument6 pages1 - Anatomical Terminology KEY愛.NiniNo ratings yet
- 3.1 Worksheet Systems, Organs and Tissues in PlantsDocument3 pages3.1 Worksheet Systems, Organs and Tissues in Plantsbkhazma17No ratings yet
- Anatomical Teaching ChartsDocument15 pagesAnatomical Teaching ChartsKennedy Absalom ModiseNo ratings yet